

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Mortality rates for patients with acute myocardial infarction (AMI) decreased dramatically from the 1980s to the 2000s, due to the widespread use of reperfusion strategies and adjuvant pharmacological therapies.1)2) However, cardiogenic shock develops in approximately 7% of patients with AMI, and is a leading cause of death.3) The mortality rate for AMI complicated by cardiogenic shock still remains high, at over 40%.4)5)6) Therefore, current guidelines for AMI recommend early revascularization in both ST-segment elevation myocardial infarction (STEMI) and non-STEMI (NSTEMI) complicated by cardiogenic shock.7)8)
Unfortunately, approximately 4–7% of patients with AMI experience out-of-hospital cardiac arrest (OHCA), and many patients with OHCA and AMI also present with cardiogenic shock.9)10)11) Although immediate revascularization should be performed in patients with AMI and OHCA after successful resuscitation, many patients die without return of spontaneous circulation (ROSC). Furthermore, it is too difficult to perform coronary angiography on resuscitated patients with profound cardiogenic shock, because of the risk of cardiac death during coronary intervention. Venoarterial extracorporeal membrane oxygenation (ECMO) provides both cardiac and respiratory life support in patients with cardiogenic shock.12)13)14) ECMO has a relatively rapid cannulation time; therefore, it can be used in the AMI setting, which requires immediate reperfusion for life saving. Several studies have shown the benefit of ECMO support in patients with AMI complicated by cardiogenic shock. However, few studies have focused on AMI with cardiogenic shock after resuscitated OHCA,15)16)17)18) and only a small number of studies have reported the timing of ECMO support in patients with AMI with cardiogenic shock, who require rapid revascularization.
In the present study, we investigated whether ECMO support before revascularisation is beneficial in patients with AMI complicated by profound cardiogenic shock after resuscitated OHCA using the Korean nationwide registry.
Go to : 
METHODS
Ethical statement
The study protocols were approved by the Ethics Committee of Chonnam National University Hospital Institutional Review Board (CNUH IRB No. CNUH-2018-261) and we have complied with the latest version of the Declaration of Helsinki (2013). A waiver for informed consent was obtained from the IRB.
Study setting and data sources
The Korean emergency medical services (EMS) system is a single-tiered, government-backed system that provides basic-to-intermediate level ambulance services. Emergency medical technicians are able to provide cardiopulmonary resuscitation (CPR) with an automated external defibrillator, evaluate cardiac rhythms, manage advanced airway, and inject intravenous or intraosseous fluids. The current EMS CPR protocol calls for emergency medical technicians to perform on-scene CPR using an automated external defibrillator every 2 minutes for at least 5 minutes. Advanced cardiac life support is not available at the scene, and emergency medical technicians are not permitted to declare death at the scene unless there are signs of irreversible death. EMS providers cannot stop CPR during transport to an emergency department. Consequently, all EMS-assessed patients are transported to a hospital.19)20)
Data were collected from EMS run sheets and hospital medical records using the Utstein-style reporting templates, and these data were extracted by medical record reviewers of the Korea Centers for Disease Control and Prevention.21) EMS run sheets are completed by EMS personnel and include patient information, ambulance operation information, clinical information, and treatment and transport information. The Korea Centers for Disease Control and Prevention visited all hospitals to evaluate medical records and document hospital outcomes electronically. A quality management committee composed of emergency physicians, epidemiologists, statistical experts, representatives from the fire department, and medical record review experts ensured the quality of the medical record review process. The quality management committee educated all medical record reviewers prior to joining the project, provided a standard manual for data abstraction, monthly feedback to the reviewers, and consultation on equivocal cases as needed.22)
Study population
This study used a cross-sectional design based on a nationwide, prospective registry involving all patients who experienced OHCA and were transported to a hospital by EMS, with resuscitation efforts performed in South Korea from 2013 to 2016. A study flow chart is presented in Figure 1. Briefly, a total of 116,374 patients experiencing OHCA in all EMS of South Korea between January 2013 and December 2016 were enrolled. Among these, 37,708 patients with obvious non-cardiac causes, 39,250 with ROSC before the emergency room (ER) visit, and 21,942 who died without ROSC were excluded. Among the remaining 17,474 patients with ROSC after the ER visit, 895 with AMI complicated by profound cardiogenic shock after ROSC, and treated with percutaneous coronary intervention (PCI) or thrombolysis, were selected for this study. After the exclusion of 22 patients who received thrombolysis, 27 who did not receive successful PCI and 662 who were not treated with ECMO, a total of 184 patients who received ECMO therapy before (n=117) or after PCI (n=67) were analyzed.
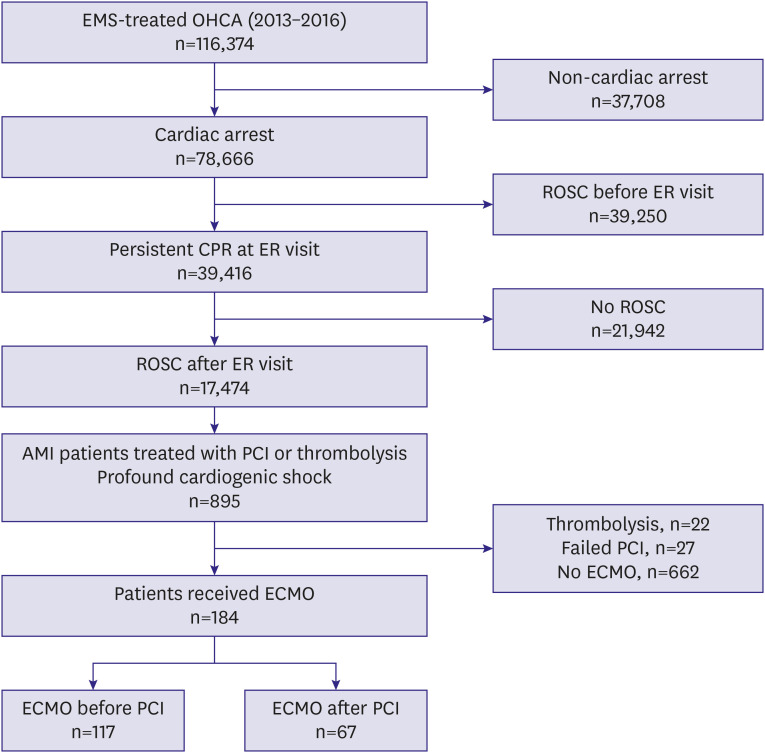 | Figure 1Study flowchart.AMI = acute myocardial infarction; CPR = cardiopulmonary resuscitation; ECMO = extracorporeal membrane oxygenation; EMS = emergency medical services; ER = emergency room; OHCA = out-of-hospital cardiac arrest; PCI = percutaneous coronary intervention; ROSC = return of spontaneous circulation.
|
Study definitions and endpoints
The diagnosis of AMI was based on the criteria for a third universal definition of myocardial infarction.23) Cardiogenic shock was defined as hypotension (<90/60 mmHg) for >30 minutes or a need for vasopressors or inotropes to maintain systolic blood pressure >90 mmHg, pulmonary congestion or elevated left-ventricular filling pressure, and evidence of end organ hypoperfusion (cool extremities, oliguria, lactic acidosis).12) The decision to apply ECMO was made at the physicians' discretion. The ECMO device was implanted by percutaneous or surgical cannulation, using a 14–17 Fr cannula for the femoral artery and a 21–24 Fr cannula for the femoral vein, in the ER, catheterisation room or coronary care unit. Successful PCI was defined when thrombolysis in myocardial infarction flow grade 3, with a minimum stenosis diameter <20%, was achieved, with or without coronary stenting in the culprit artery. Patients received 300 mg aspirin and 300 or 600 mg clopidogrel, 60 mg prasugrel, or 180 mg ticagrelor as a loading dose prior to PCI. After PCI, 100–300 mg aspirin and 75 mg clopidogrel daily, 5 or 10 mg prasugrel once daily, or 90 mg ticagrelor twice daily was prescribed as the maintenance dose. Therapeutic hypothermia was defined as a case receiving hypothermia treatment using external, internal or mixed cooling, with target temperature between 32 and 34°C and a target duration of 12–24 hours.22) Anticoagulation strategy and target for therapeutic hypothermia in patients underwent ECMO were deponed on each institution protocol. The definition of successful hypothermia was a recovery to alert mental status after finish of target temperature management.
The primary endpoint was 30-day mortality. We also analysed the incidence rates of in-hospital mortality and good neurologic function at discharge, with the latter defined as a score of 1 (no neurologic disability) or 2 (moderate disability; able to perform daily activities independently) on the Cerebral Performance Category scale, which is a 5-point scale used to evaluate neurologic functioning.
Statistical analysis
Continuous variables are presented as means±standard deviation and were compared using the unpaired t-test or the Mann–Whitney rank-sum test. Discrete variables are expressed as counts with percentages and were analysed by Pearson's χ2 test or Fisher's exact test. Kaplan-Meier curves were constructed to compare primary endpoints between the ECMO before and after PCI groups; differences were assessed using the log-rank test. Cox's proportional hazards regression model (with adjustment for covariates) was used to assess clinical outcomes. Variables that were significant in the univariate analysis (p<0.1) were included in the multivariate analysis.
All analyses were 2-tailed, and a p value <0.05 was considered to reflect statistical significance. All statistical analyses were performed using SPSS for Windows (ver. 21.0; SPSS Inc., Chicago, IL, USA).
Go to :
RESULTS
Baseline characteristics and in-hospital care according to the timing of extracorporeal membrane oxygenation
Table 1 shows the baseline characteristics and in-hospital care data according to the timing of ECMO. The mean age was similar between the 2 groups, and the rate of male patients was also comparable. In total, 76.1% of patients suffered sudden cardiac death, as observed by a witness, and only 28.8% of patients received bystander CPR. There was no significant difference in the rate of bystander CPR between groups (29.1% vs. 28.4%, p=0.919). Initial shockable rhythm at the scene was seen in 53.8% of patients, with almost all receiving ventricular fibrillation (50.0% of patients). At the ER visit, shockable rhythm was observed in 27.7% of patients, and ventricular fibrillation was documented in 25.5%. The rate of shockable rhythm at the scene or ER was comparable between the 2 groups. Although the total duration of CPR was similar between the 2 groups, door-to-balloon time was significantly longer in the pre-PCI ECMO group (128.5±57.3 vs. 105.5±39.1, p=0.002). Therapeutic hypothermia was attempted with similar frequency between the 2 groups and the success rate was also comparable. Approximately half of patients in the pre-PCI ECMO group received ECMO in the ER; however, 71.6% of patients in the post-PCI ECMO group received ECMO in the catheterization room.
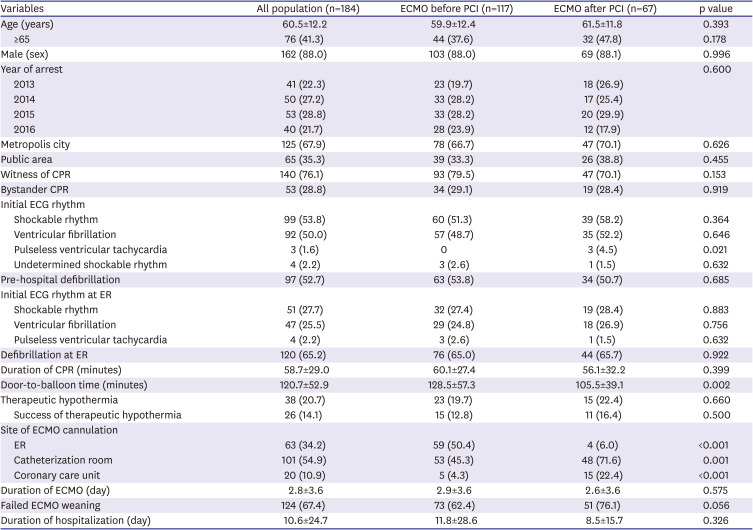
Table 1
Baseline characteristics and in-hospital care of overall population and according to timing of ECMO
Values are expressed as mean±standard deviation or number (%).
CPR = cardiopulmonary resuscitation; ECG = electrocardiogram; ECMO = extracorporeal membrane oxygenation; ER = emergency room; PCI = percutaneous coronary intervention.
![]()
Baseline characteristics and in-hospital care according to survival or death at 30 days
Thirty-day mortality was 80.4% (148 patients). Table 2 shows the baseline characteristics and in-hospital care data according to survival or death at 30 days. Surviving patients were younger and mostly male. Although the rate of witness CPR was similar between the 2 groups, bystander CPR was performed more often in survived patients (47.2% vs. 24.3%, p=0.007). Shockable rhythm, both at the scene and in the ER, was observed more often in survived patients, most of whom received ventricular fibrillation. The total duration of CPR tended to be longer in the death group and door-to-balloon time was comparable between the 2 groups. Therapeutic hypothermia was tried with similar frequency in both groups; however, the success rate was higher in surviving patients. Surviving patients received more pre-PCI ECMO therapy compared to the death group (83.3% vs. 58.8%, p=0.006). In total, 58.3% of surviving patients received ECMO in the ER and 60.1% of expired patients received ECMO in the catheterization room. Although 16.2% (24 patients) of the deceased patients were successfully weaned from ECMO, they eventually died of cardiac or non-cardiac problems after ECMO weaning. The total durations of ECMO and hospitalization were much longer in survived patients.
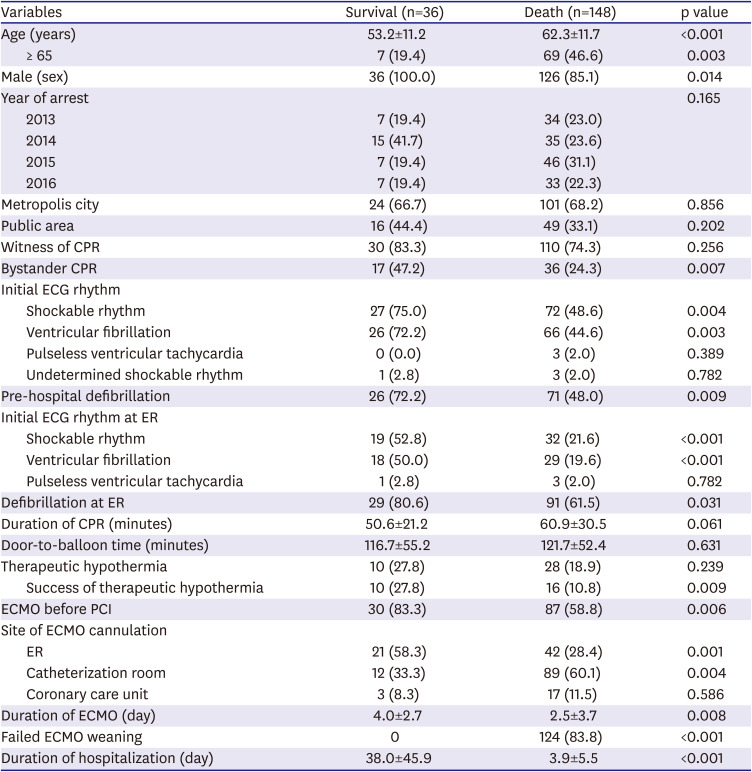
Table 2
Baseline characteristics and in-hospital care of study patients according to survival or death at 30 days
Values are expressed as mean±standard deviation or number (%).
CPR = cardiopulmonary resuscitation; ECG = electrocardiogram; ECMO = extracorporeal membrane oxygenation; ER = emergency room; PCI = percutaneous coronary intervention.
![]()
Clinical outcomes
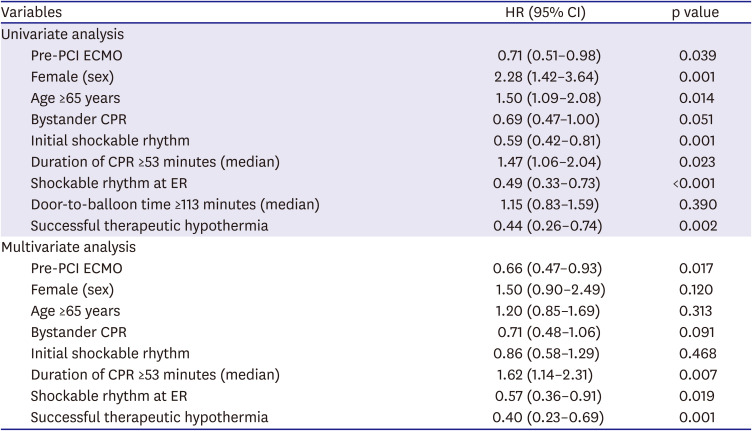
Figure 2A shows the incidence of study endpoints. In-hospital mortality was 78.8% (145 patients) in the entire study population and was significantly lower in the pre-PCI ECMO group (73.5% vs. 88.1%, p=0.020). Thirty-day mortality was also lower in the pre-PCI ECMO group compared to the post-PCI ECMO group (74.4% vs. 91.0%, p=0.006), and the result was similar on Kaplan-Meier survival analysis (Figure 2B, log-rank p=0.017). The proportion of patients with better neurologic function at discharge, defined as a Cerebral Performance Category score of 1 or 2, did not differ significantly between groups (54.8% vs. 37.5%, p=0.382). In multivariate Cox-regression analysis, pre-PCI ECMO significantly lowered 30-day mortality compared to post-PCI ECMO (Table 3, adjusted hazard ratio [HR], 0.66; 95% confidence interval [CI], 0.47–0.93; p=0.017).
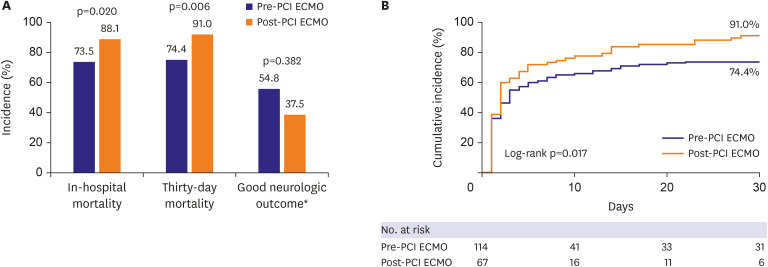 | Figure 2Incidences of study endpoints (A), and Kaplan-Meier estimates of cumulative probabilities of 30-day death for patients according to ECMO timing (B).ECMO = extracorporeal membrane oxygenation; PCI = percutaneous coronary intervention.
*Defined as scoring 1 or 2 on the cerebral performance category score.
|
Table 3
Predictors of death at 30-days
CI = confidence interval; CPR = cardiopulmonary resuscitation; ECMO = extracorporeal membrane oxygenation; ER = emergency room; HR = hazard ratio; PCI = percutaneous coronary intervention.
![]()
Predictors of 30-day mortality
To investigate the independent predictors of 30-day mortality, Cox's proportional hazards regression analysis was performed (Table 3). Continuous variables, such as the duration of CPR and door-to-balloon time, were converted to dichotomous variables using the median value. Shockable rhythm at the ER (HR, 0.57; 95% CI, 0.36–0.91; p=0.019) and successful therapeutic hypothermia (HR, 0.40; 95% CI, 0.23–0.69; p=0.001) were also associated with improved 30-day survival. However, prolonged CPR significantly predicted 30-day death (HR, 1.62; 95% CI, 1.14–2.31; p=0.007).
Go to :
DISCUSSION
In the present study, we compared 30-day mortality between ECMO before PCI and ECMO after PCI in patients with AMI complicated by profound cardiogenic shock after resuscitated cardiac arrest, using data from a nationwide prospective OHCA registry. The principal findings were as follows: 1) in-hospital and 30-day mortality were unacceptably high despite successful PCI in patients with AMI complicated by cardiogenic shock after resuscitated cardiac arrest; 2) early ECMO before PCI significantly reduced both in-hospital and 30-day mortality compared to ECMO after PCI; and 3) there was a tendency toward more favourable neurologic outcomes at discharge in patients who received ECMO before PCI than those who received ECMO after PCI.
As far as we know, there are no randomized controlled trials regarding the benefit of early ECMO therapy before PCI in patients with AMI complicated by cardiogenic shock.15)16)17)18) Recently, one retrospective study compared short-term survival between ECMO before PCI and ECMO after PCI in 46 STEMI patients, and showed that ECMO before PCI improved the chance of survival in patients with STEMI with complicated refractory cardiogenic shock.24) However, there was limited evidence of the benefit of early ECMO therapy in patients with AMI after resuscitated cardiac arrest. Despite a lack of randomized controlled trials, a large meta-analysis showed the usefulness of early ECMO therapy for increasing survival and favourable neurologic outcomes in patients after resuscitated cardiac arrest.18) CPR presentation in the AMI setting is associated with high short-term mortality in cases of AMI with cardiogenic shock treated by ECMO25); however, no study has entirely enrolled AMI patients after resuscitated OHCA. Retrospective data from 253 patients who underwent ECMO indicated that a composite endpoint of in-hospital mortality, left ventricular assist device implantation, and heart transplantation was significantly lower in ECMO before PCI than in ECMO after revascularization (32.0% vs. 49.5%; odds ratio, 0.48; 95% CI, 0.24–0.98; p=0.045).26) In the current study, all patients were survivors after OHCA in the Korean nationwide registry contrary to above-mentioned study. Although the population recruited to this study included survivors after OHCA, in-hospital and 30-day mortality were unacceptably high, which could be due to the prolonged duration of CPR in the study population compared to other studies.17) Consequently, the early ECMO before PCI can be useful in both AMI patients complicated by shock with or without CPR. The nationwide OHCA registry used herein did not have detailed information about procedural data and initial diagnosis, such as STEMI or NSTEMI. However, patients enrolled in the current study had thrombolysis in myocardial infarction flow grade 3 after PCI, which is associated with improved mortality after ECMO.27) Furthermore, NSTEMI patients complicated by cardiogenic shock seem to have similar or worse clinical outcomes compared to STEMI patients with shock.28) Therefore, the initial diagnosis may not have impacted clinical outcomes. Early ECMO may improve the chance of favourable neurologic outcomes18); however, there was no significant difference in the frequency of good neurologic outcomes at discharge. Because of the high in-hospital mortality in the current study, the sample size was not sufficient (the total number of survivors was 39) to assess the effect of early ECMO on neurologic outcomes. Nevertheless, there was a higher tendency toward favourable neurologic outcomes at discharge in patients who received ECMO before PCI than those who received ECMO after PCI (54.8% vs. 37.5%). However, the reduced mortality with similar neurologic outcomes suggests the potential for generating survivors with poor outcomes.
Cannulation site between early and late ECMO group was significantly different in our study. Early ECMO group more received ECMO at ER (50.4% vs. 6.0%), and late group more received it at catheterization room (45.3% vs. 71.6%) or coronary care unit (4.3% vs. 22.4%). However, the detailed baseline or angiographic characteristics, and the data about reason for late ECMO insertion after successful PCI were not available in the current registry. Although there was no definite reason for late ECMO in the current study, there was a possibility that many patients in late group received ECMO due to CPR or profound cardiogenic shock even after successful PCI. This difference rather strengthens our conclusion that early ECMO before PCI can be useful compared to ECMO after PCI in AMI patients with profound cardiogenic shock after ROSC.
In the current study, successful therapeutic hypothermia and shockable rhythm were preventive factors of 30-day mortality. Patients with poor neurologic outcomes may be prone to severe infections, such as pneumonia, urinary tract infection or pressure sore infection, which could lead to septic shock or multi-organ failure. Shockable rhythm was also related to favourable clinical outcomes in patients treated with ECMO for refractory cardiogenic shock post-cardiac arrest.29)
The current study had several limitations. First, it used a non-randomised, observational design despite being based on a large, prospective, nationwide OHCA registry. Although we performed multivariate analysis, other variables not included in our registry may have influenced the study outcomes. Second, baseline characteristics, comorbidities and laboratory findings associated with clinical outcomes, such as serum lactate and prothrombin activity, were not considered. Third, the nationwide data we used did not include echocardiographic or renal replacement therapy data, nor detailed data of ECMO, such as pump flow. Fourth, data on in-hospital complications, such as limb ischemia, bleeding, stroke, and sepsis, which could impact mortality, were not available. Finally, the rate of ECMO implantation in the ER was high in the current study. Because all study population in the current study underwent CPR on arrival, and there might be a high probability of ECMO implantation in ER. Because non-fluoroscopy guided ECMO implantation was associated with higher complication rate, such as insertion site bleeding or catheter mal-apposition,30) this high rate of ECMO insertion at ER could impact clinical outcomes.
In conclusion, ECMO support before revascularisation was associated with improved short-term survival compared to ECMO after revascularisation in patients with AMI complicated by profound cardiogenic shock after resuscitated cardiac arrest. In the absence of randomised controlled trials, this study provides valuable information on the optimal management of these high-risk patients.
Go to :
 XML Download
XML Download