

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Infective endocarditis (IE), though a rare disease with a yearly incidence of 3–10 per 100000 among general population, is a highly morbid medical condition that can lead to fatal or disabling consequences.1) Despite improvements in diagnostic strategy, antimicrobial treatments and surgical interventions, the mortality of IE has not improved over the last 3 decades.2)3) Meanwhile, as a consequence of growing number of patients undergoing prosthetic heart valve replacement, the incidence of prosthetic valve endocarditis (PVE) has increased in recent years. PVE is typically known as a more deadly complication compared with native valve endocarditis (NVE) due to its challenging nature to handle severe adhesion surrounding the heart, and to more severe and broader lesions requiring extensive procedures.1)4) Although several studies have described and evaluated the surgical outcomes PVE relative to NVE, its prognostic values on early and late outcomes with regards to mortality, reinfections as well as other important valve-related outcomes have not been well-characterized through studies with contemporary, reasonably-sized cohorts. With these regards, in the aim of contributing to the body of evidence in the field of surgical IE, we sought to comprehensively analyze clinical patterns and surgical outcomes of PVE compared with NVE.
Go to : 
METHODS
Ethical statement
The study protocol was approved by the Institutional Review Board of Asan Medical Center (2020-0271). The requirement for informed consent from individual patients was waived due to the retrospective design of the present study.
Study population
We retrieved consecutive 269 patients who underwent cardiac surgery because of IE between November 2013 and March 2019 from the institutional cardiac surgery database of Asan Medical Center, Seoul, Korea. The disease was considered active if the patients were currently being treated with anti-microbial agents against endocarditis based on the definition provided by the Society of Thoracic Surgeons (STS).5) Surgical treatment was considered in patients with following signs referred to the current practice guidelines; heart failure, severe valve dysfunction, periannular involvement or paravalvular abscess, large mobile vegetation (>10 mm) with embolism or high risk of embolic event, persistent sepsis despite adequate antibiotics therapy and IE caused by Staphylococcus aureus, fungal or highly resistant microorganism.6)7) Of 269 patients, 56 had PVE and remainder (n=213) had NVE. For patients undergoing surgery because of infective endocarditis, valve substitute was generally selected as for any other valve surgeries based on the current practice guidelines.6)7) However, bioprosthetic valve was occasionally considered in younger patients who had high operative risk, particularly, including chronic kidney and liver disease to avoid anticoagulation therapy.
Data collection
Clinical follow-up information on individual patients was obtained through March 2020 from institutional electronic medical databases and chart reviews. Infectious etiology was collected by microbiologic laboratory results, and preoperative blood cultures, intraoperative cultures or 16S rDNA analysis of valvular tissue were reviews to confirm the causative pathogens. Detailed lesions of the affected valves were recorded based on echocardiographic reports, intraoperative findings and pathologic examinations of valvular tissue. Data regarding vital status and date of death were collected from institutional electronic, and were further validated by health claims databases for National Health Insurance Service, which is mandatory universal health insurance program providing comprehensive medical care coverage to all residents of the Republic of Korea.8)9)
Outcome measures
The primary outcomes of interests were all-cause mortality and valve-related adverse events, including valve reinfection, stroke, valve reoperation and permanent pacemaker (PPM) implantation referencing the Society of Thoracic Surgery Guidelines.5) Early mortality was defined as deaths within 30 days of surgery. Recurrent IE was further categorized as early and late recurrence based on a cutoff of 180 days from the surgery.10)11) For further measure, perioperative complications (e.g., low cardiac output syndrome [LCOS] requiring mechanical circulatory support, early stroke, newly initiated dialysis and bleeding demanding surgical intervention) were also evaluated.
Statistical analyses
Continuous variables, expressed as mean±standard deviation, were compared using Mann-Whitney U test and Student's t test, as appropriate. Categorical variables were presented as frequencies and percentages and compared using χ2 or Fisher exact tests. Time trends in proportions of PVE among surgical patients with IE were tested by χ2 test for linear trend after the breaking down the surgical period into quartiles. Kaplan-Meier plots were used to construct the conditional probabilities for survival and freedom from adverse events, and the log-rank test was adopted to compare differences in the estimates between the 2 groups. Potential risk factors for overall mortality were assessed using Cox proportional-hazard (PH) model. In this model, the PH assumption was examined using scaled Schoenfeld residuals and no relevant violations were observed in all tested models. After univariable Cox PH analyses, variables with p value less than 0.2 were included into the multivariable PH models. Afterward, stepwise backward elimination technique was used to retain only variables with p<0.1 in the final multivariable model. Results are presented as hazard ratio (HR) for overall mortality with corresponding 95% confidence interval (CI) and p value. In addition, we assumed that the comparative risk of mortality may differ between PVE and NVE across early and late phases. Therefore, we conducted a landmark survival analysis to test this hypothesis. All reported p values were 2-sided, and p values less than 0.05 were considered statistically significant. Analyses were performed using R statistical software, version 3.4.0 (R Foundation, Vienna, Austria; http://www.R-project.org/).
Go to :
RESULTS
Baseline and operative profiles
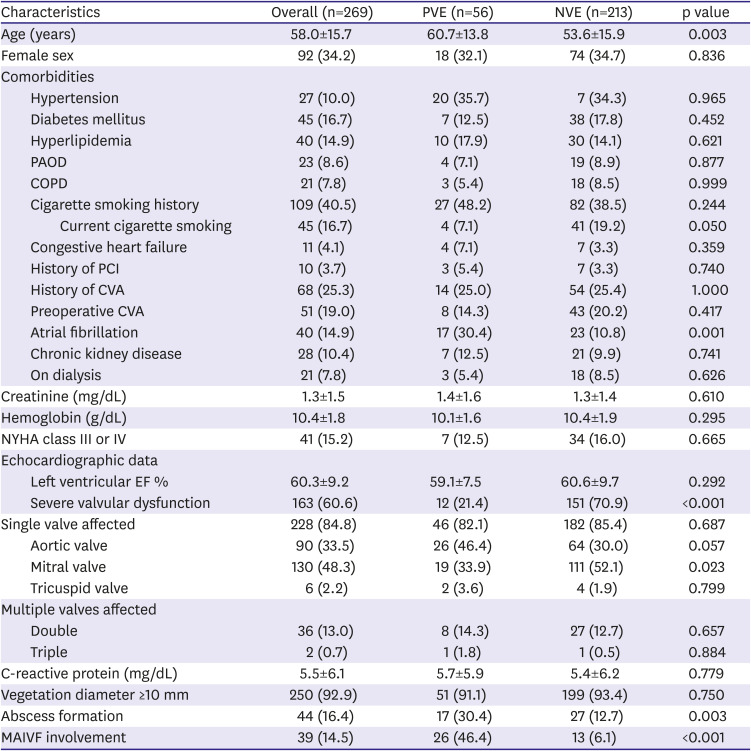
The proportion of PVE among the entire surgical IE has gradually increased from 15.4% (11/71) to 29.5% (18/61) through the study period (p=0.055) (Figure 1). The baseline profiles of patients with PVE and NVE are summarized in Table 1. PVE patients were older, and more commonly had mitral aortic intervalvular fibrosa (MAIVF) involvement and abscess formation compared to NVE patients. There were 51 (19.0%) patients who experienced preoperative embolic event including cerebrovascular accident and visceral embolism; 8 (14.4%) and 43(20.2%) in PVE and NVE group, respectively (p=0.417). The mitral valve was the most frequently affected site in overall cohort (n=130, 48.3%) with its higher proportion in NVE (n=111, 52.1%) than in PVE (n=19, 33.9%). Inversely, PVE patients more often had IE involvement in the aortic valve (n=25, 44.6%). The distribution of infected valves is demonstrated in Table 1.
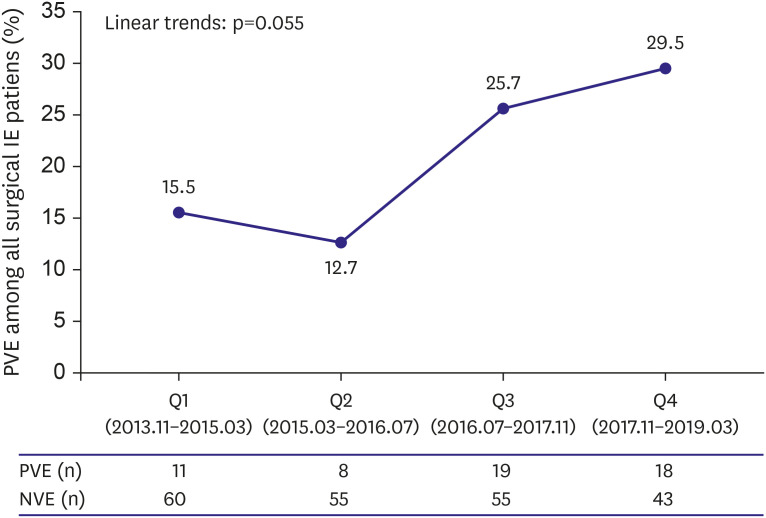 | Figure 1Quartile trends in proportion of prosthetic valve endocarditis among surgical patients with infective endocarditis over time.NVE = native valve endocarditis; PVE = prosthetic valve endocarditis.
|
Table 1
Baseline characteristics
Values are number (%) or mean ± standard deviation, unless otherwise indicated.
COPD = chronic obstructive pulmonary disease; CVA = cerebral vascular accident; EF = ejection fraction; MAIVF = mitral aortic intervalvular fibrosa; NVE = native valve endocarditis; PAOD = peripheral arterial occlusive disease; PCI = percutaneous coronary intervention; PVE = prosthetic valve endocarditis.
![]()
Indication of surgery and operative profiles are detailed in Tables 2 and 3, respectively. Of 269 patients, 81 (30.1%) patients underwent emergent surgery and 2 (0.7%) demanded preoperative mechanical circulatory support with extracorporeal membrane oxygenation because of cardiogenic shock. Valves were replaced with bioprosthetic and mechanical valve in 88 (32.7%) and 123 (45.7%) patients, respectively. A significantly higher proportion of PVE patients necessitated MAIVF repair compared to NVE patients. Cardiopulmonary bypass (235.1±105.3 vs. 133.3±51.0 minutes; p<0.001) and aortic cross clamping times (145.2±66.6 vs. 92.9±14.4 minutes; p<0.001) were significantly longer in PVE patients as compared with NVE patients.

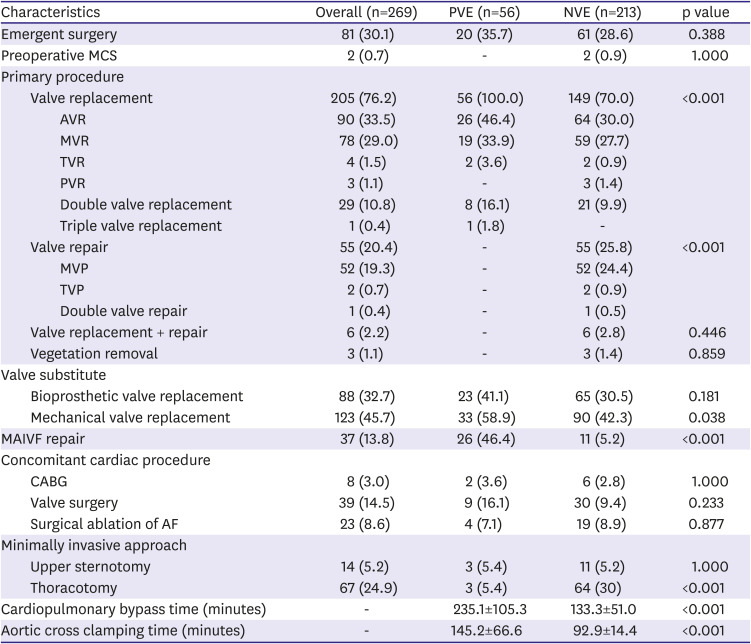
Table 2
Indication of surgery
Values are number (%) or mean±standard deviation, unless otherwise indicated.
NVE = native valve endocarditis; PVE = prosthetic valve endocarditis.
![]()
Table 3
Operative profile
Values are number (%) or mean±standard deviation, unless otherwise indicated.
AF = atrial fibrillation; AVR = aortic valve replacement; CABG = coronary artery bypass graft; MAIVF = mitral aortic intervalvular fibrosa; MCS = mechanical circulatory support; MVP = mitral valve prolapse; MVR = mitral valve replacement; PVR = pulmonary valve replacement; TVP = tricuspid valve prolapse; TVR = tricuspid valve replacement.
![]()
Causative pathogens
The most prevalent pathogen in overall cohort was the viridans group Streptococci, which was isolated in 87 (32.3%) patients. The coagulase negative Staphylococci and viridans group Streptococci was the most common pathogen for patients with PVE (n=15, 26.8%) and NVE (n=78, 36.6%), respectively. Both methicillin-sensitive (5.4% vs. 7.5%; p=0.790) and resistant (5.4% vs. 5.2%; p=1.000) Staphylococcus aureus infection as well as fungal infection (5.4% vs. 1.9%; p=0.325) rates were similar between the groups (Table 4).
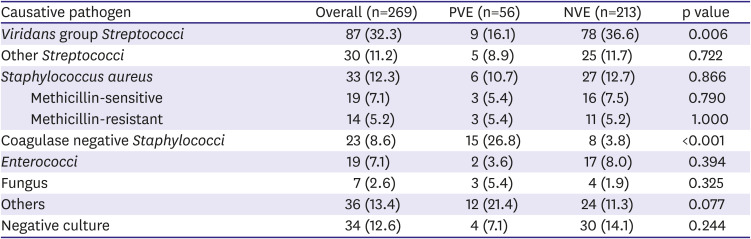
Table 4
Microbiological data
Values are number (%) or mean±standard deviation, unless otherwise indicated.
PVE = prosthetic valve endocarditis; NVE = native valve endocarditis.
![]()
Clinical outcomes
Details of perioperative and long-term adverse clinical outcomes, and their comparative risks are depicted in Table 5. The early mortality rates were 14.3% and 6.1% in PVE and NVE patients, respectively (p=0.049). With regard to perioperative complications, an early stroke rate was comparable between the groups (12.5% vs. 8.5%; p=0.356), but the incidence rates of other early major morbidities including LCOS demanding mechanical support (12.5% vs. 3.8%; p=0.017), newly initiated dialysis (19.6% vs. 6.6%; p=0.004), reoperation for bleeding (14.3% vs. 3.3%; p=0.003) and early PPM implantation (12.5% vs. 1.4%; p=0.001) rates were significantly higher in the PVE group than the NVE group. PVE patients had longer intensive care unit stay (3.0 days [interquartile range; IQR, 2.0–7.3 days] vs. 2.0 days [IQR, 1.0–3.0 days]; p=0.031) and hospital stay (35.5 days [IQR, 22.8–78.0 days] vs. 28.0 days [IQR, 15.0–37.0 days]; p=0.004) compared with NVE patients.
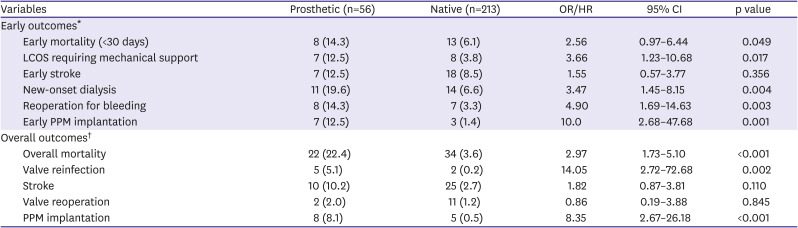
Table 5
Comparative outcomes of prosthetic versus native groups
*Early outcomes are given as OR and long-term outcomes are given as HR derived from univariable logistic regression and Cox-proportional hazard model, respectively. †Overall outcomes are presented as number of patients (number/100 patients-year).
CI = confidence interval; HR = hazard ratio; LCOS = low cardiac output syndrome; OR = odds ratio; PPM = permanent pacemaker.
![]()
During follow-up (28.2 months [IQR, 11.5–45.8 months]; overall 648.8 patient-years), PVE group showed significantly higher risk of overall mortality (HR, 2.97; 95% CI, 1.73–5.10; p<0.001), valve reinfection (HR, 16.14; 95% CI, 3.24–80.35; p<0.001) and PPM implantation than NVE group (HR, 8.35; 95% CI, 2.67–26.18; p<0.001). With regard to survival, PVE group showed significantly higher risk of perioperative (odds ratio [OR], 2.56; 95% CI, 0.97–6.44; p=0.049) and overall mortality (HR, 2.97; 95% CI, 1.73–5.10; p<0.001). The landmark survival analysis revealed that mortality risk in PVE group was considerably higher within 1 year after IE surgery (HR, 3.09; 95% CI, 1.65–5.78; p<0.001) and such trend continued even after 1 year of time (HR, 2.76; 95% CI, 0.96–7.99; p=0.061). Recurrence of IE was documented in 7 patients, occurring 5 (5.1%/patient-years) in PVE group and 2 (0.2%/patient-years) in NVE group. Of 7 patients with valve reinfection, 3 had non-viridans group Streptococcal infection at their initial endocarditis event. The mean time after surgery to valve reinfection was 23.9 months (IQR, 7.6–23.9 months) in the PVE group and 33.9 months (IQR, 25.6–42.2 months) in the NVE group. Early recurrent IE occurred in only 1 patient with PVE at 5 months after index IE surgery. Late recurrence developed in 6 including 4 in PVE group and 2 in NVE group. In addition to 10 patients who had implanted PPM during hospitalization, 3 patients necessitated PPM implantation during a follow-up period (1 in the PVE group and 2 in the NVE group). Overall, PPM implantation was implanted in 13 patients in study cohort—8 (8.1%/patient-years) in the PVE group and 5 (0.5%/patient-years) in the NVE. The most common reason for PPM implantation was complete atrioventricular block (8/13, 61.5%) with its rates among all PPM cases of 62.5% (5/8) in the PVE group and 60.0% (3/5) in the NVE group.
Kaplan-Meier curves showed a significantly decreased overall survival (OS), and freedom from valve reinfection and PPM implantation in the PVE compared with NVE; however, there were no significant differences in freedom from stoke and valve reoperation between PVE and NVE group (Figure 2). One-year and 3-year OS rates were 69.6±6.1% and 61.3±6.7% in PVE patients, respectively; and 89.2±2.1% and 85.4±2.5% in NVE patients (p<0.001), respectively (Figure 2A). The freedom from IE recurrence at 3-year was 80.9±7.4% and 99.3±0.7% in the PVE and NVE group, respectively.
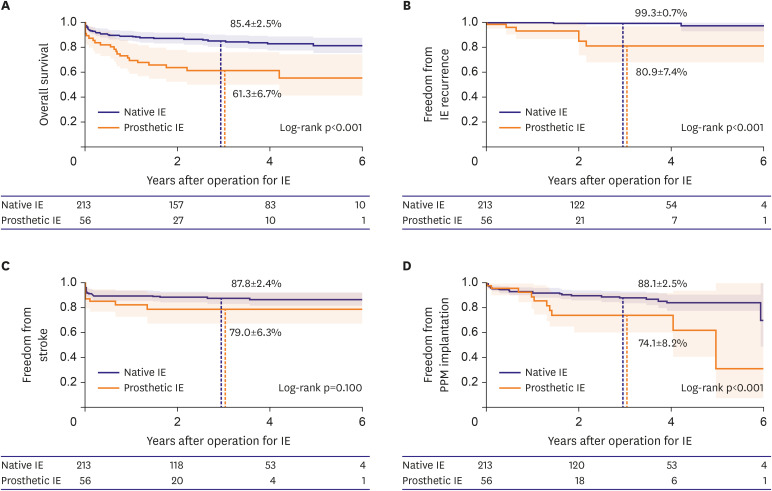 | Figure 2Kaplan-Meier curves for the clinical outcomes. (A) Kaplan-Meier curve for the survival rates. (B) Kaplan-Meier curve for freedom from IE recurrence rates. (C) Kaplan-Meier curve for freedom from stroke rates. (D) Kaplan-Meier curve for freedom from PPM plantation.IE = infective endocarditis; PPM = permanent pacemaker.
|
Factors associated with mortality and IE recurrence
The results of univariable and multivariable Cox PH analyses to determine risk factors for overall mortality are summarized in Table 6. Final multivariable model revealed that PVE (HR, 2.67; 95% CI, 14.0–5.07; p=0.003), age (HR, 1.04; 95% CI, 1.01–1.07; p=0.009), chronic kidney disease (HR, 2.93; 95% CI, 1.58–5.44; p=0.001), multi-valve involvement (HR, 2.13; 95% CI, 1.14–3.98; p=0.01), and causative pathogens of Staphylococcus aureus (HR, 3.26; 95% CI, 1.68–6.33; p<0.001) or fungus (HR,3.13; 95% CI,1.25–7.86; p=0.015) were independent and significant risk factors for overall mortality
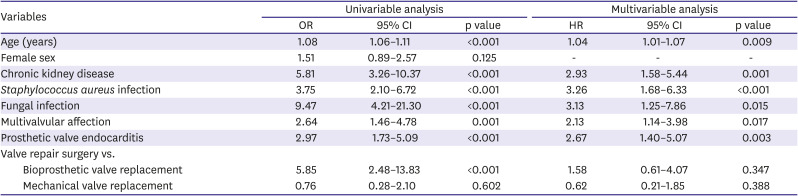
Table 6
Risk factors for mortality in patients with infective endocarditis
Early outcomes are given as OR; long-term outcomes are given as HR.
CI = confidence interval; HR = hazard ratio; OR = odds ratio.
![]()
With regard to IE recurrence, comprehensive risk factor analyses were unavailable because of a limited number of events (n=7). Univariable Cox PH model, however, showed that following variables were significantly associated factors of recurrence of IE: PVE (HR, 14.05; 95% CI, 2.72–72.68; p=0.002), MAIVF involvement (HR, 17.92; 95% CI, 3.35–95.81; p=0.001), and causative pathogen of Staphylococcus aureus (HR, 10.83; 95% CI, 1.63–72.23; p=0.014) and fungus (HR, 19.87; 95% CI, 1.59–248.05; p=0.020).
Go to :
DISCUSSION
In the present study analysis, the patients with PVE were characterized as being older and presenting with more extensive infectious lesions compared to NVE patients consistent with previous studies.4)10)12) PVE was associated with significantly higher perioperative risk and it was also associated with substantial risk of late mortality.
In concordance with previous studies, patients undergoing surgery for PVE showed significantly higher risk of early mortality than patients with NVE.13)14)15) Although an early mortality rate of PVE group in the present study was relatively lower (14.3%) than reported rates ranging from 19% to 50%, it was still significantly poorer than that of NVE (6.1%).4)10)12) Kaplan-Meier analysis showed notably inferior OS of PVE group compared with NVE group through the follow-up period, and the impaired survival outcomes seemed not confined to early period but rather extended to late period as demonstrated by the landmark survival analysis. This unique finding of this study that PVE impacts on late outcomes may be explained by a multitude of factors such as greater baseline risk (i.e., older age, higher AF prevalence) and more virulent causative pathogens (more Staphylococci infection) as compared with NVE, but also higher incidences of major non-fatal complications associated with more challenging and extensive PVE surgery might have affected late survival adversely.
Whether the type of valve substitute has any significant clinical impacts in IE is still an issue of open debates.16)17)18)19)20)21) Results from a large multicenter study by Toyoda and colleagues22) suggested that choice between bioprosthetic and mechanical prostheses did not affect long-term mortality or risk of recurrent infection in surgical IE, and these findings are in agreement with those of the present study. These results may provide a further supporting evidence for current practice guidelines that patient-guided approaches should be used in the choice of prosthetic types even in IE as for any other valve surgeries.7)22)23) As the life expectancy is the most important indicator of this decision, estimated survival outcomes should be kept into consideration with priority. Of note, the long-term survival is very limited in PVE with a median survival time of around 5 years (Figure 2A), and by this reason, most of PVE patients may be better fitted to bioprosthetic valve replacement as its durability is expected go beyond their life expectancy except for healthy/young individuals.
The risk of conduction disturbances and consequent PPM implantation is another important issue in PVE. Inherent risk of cardiac conduction injuries that valvular surgery poses in addition to the extension of IE to conduction systems are the main drivers of developing atrioventricular block (AVB) demanding PPM implantation in surgical IE patients.24)25)26) Previous studies demonstrated that aortic valve (AV) involvement, valvular abscess, prior valvular surgery and Staphylococcus aureus infection were strong predictors of postoperative PPM implantation, and valve replacement compared to valve repair surgery was another risk factor.24)25)27) In the present study, PVE was characterized by more common AV and MAIVF involvement, Staphylococci infection and abscess formation as compared with NVE. In addition, valve repair is not available option in PVE. Finally, risk of injuries to conduction system is a probably negligible issue than leaving infectious material in the heart in IE surgery. Therefore, all of these inherent conditions given in PVE seem inevitably increase the risk of PPM insertion postoperatively.
Recurrence of IE is another significant and potentially devastating complication after IE surgery. There is a paucity of data demonstrating significant predictors of IE recurrence. A meta-analysis including 8,978 patients and a population-based cohort study demonstrated that valve repair surgery is associated with lower rate of recurrent endocarditis than valve replacement, and this result implies that PVE fundamentally has a higher chance to have recurrent IE than NVE.28)29) Furthermore, as intravenous leads of PPM may contribute as a source of IE, the higher rate of PPM implantation demonstrated in PVE further increases the risk of recurrent infection. Univariable analyses revealed Staphylococcus aureus or fungal infection and MAIVF involvement as significant and independent risk factors along with PVE; however, the number of events was not enough to offer more robust statistical examinations. Therefore, the issue of reinfection after PVE surgery needs further studies in larger cohorts ideally with longer follow-up information to obtain greater understanding of this futile complication. Such studies are expected to allow identification of clues to prevent this complication.
The present study poses several limitations to be acknowledged. First, this study has inherent limitation of retrospective design of the research. Second, our study population might be affected by referral bias. This is a single-, high-volume quaternary referral center study, therefore, the study results may not generalizable to other settings. Third, the study cohort is influenced by surgical selection bias. Since this study include only patients who underwent surgical treatment of IE but not those who received medical treatment only, the results of the study have limited applicability to overall medical and surgical PVE.
In conclusion, the proportion of PVE among surgical IE patients has increased gradually over time. PVE surgery carries significantly higher perioperative risks of mortality and major complications as compared with NVE, and such greater risks extended beyond the early postoperative phase. This information should be factored into decision making for optimal management in PVE, and should also be provided to patients' side for adequate informed consents.
Go to :
 XML Download
XML Download