

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF) is the most commonly diagnosed arrhythmia and is associated with an increased risk of adverse cardiovascular outcomes, including heart failure, stroke and death.1) Catheter ablation has shown to be effective in restoring sinus rhythm and advances in ablation technology allow cure rates of 60% to 70% for paroxysmal AF.2) These success rates are largely based on a cut-off of 30 seconds of documented atrial arrhythmia, which is not an optimal way to measure outcome. Patients experiencing very short recurrences of AF post-ablation may still do very well with a significant improvement in quality of life (QOL). A better measure may be AF burden, defined as the proportion of time that an individual is in AF during a monitoring period. In this review we aim to discuss the role of AF burden assessment in measuring outcomes and managing arrhythmia before and after AF ablation.
Go to : 
AF BURDEN AND POST-ABLATION MONITORING
The recurrences after PVI are usually reported based on patient's symptoms and/or intermittent rhythm monitoring (IRM) such as 24 or 48-hour Holter monitoring performed at 3–6 month intervals. However, these IRM measures are unreliable because of the limited window of examination, underestimating the true AF burden3)4)5) and overestimating the procedural success. In contrast, intracardiac continuous monitoring (ICM) may be a powerful tool for measuring true AF burden.6)7)
Charitos et al.,8) evaluated the sensitivity differences between IRM and ICM by analyzing the information obtained from 647 patients monitored with a subcutaneous implantable loop recorder or a pacemaker. In brief, they created different IRM models (24 hours and 7, 14, and 30 days) for every patient and they studied their sensitivities (defined as the proportion of patients correctly identified as having AF recurrence with the simulated IRM strategy to the true number of patients having AF recurrence identified from ICM). A 24-hour Holter strategy had a sensitivity of only 52% and even with 30-day Holter strategy for a total monitoring duration of 90 days had a sensitivity not exceeding 82%. Moreover, the sensitivity in detecting AF was driven by the both the AF burden and its dispersion over time, having more benefit in detecting AF patients with lower AF density.
Another study conducted by Kottkamp et al.,9) enrolled 100 patients with paroxysmal and persistent AF that underwent catheter ablation and compared a 24-hour Holter with 7-day Holter monitoring at 3, 6 and 12 months post-ablation. They found a freedom from AF in patients with paroxysmal AF was 83% vs. 55% (p=0.0002) at 6 months follow-up and 88% vs. 74% (p=0.14) at 12 months for the 24-hour ECG or 7-day ECG results, respectively. Similarly, the Discerning Symptomatic and Asymptomatic Episodes Pre and Post Radiofrequency Ablation of Atrial Fibrillation (DISCERN-AF) study10) used subcutaneous implanted cardiac monitors to evaluate the recurrence of AF after catheter ablation. Defined by symptomatic recurrence, the success rate of ablation was 58% but when success was defined as any AF/atrial flutter/atrial tachycardia detected on ICM, the success rate fell to 46%. The proportion of asymptomatic episodes also increased after ablation by a factor of 3–4 because post-ablation episodes were shorter, with lower heart rates. Twelve percent of patients had exclusively asymptomatic episodes.
Describing trial outcomes in terms of reduction in AF burden may be a better measure of clinical success post-ablation. In DISCERN AF, the freedom from a 30 second recurrence of arrhythmia was only 46% at 18 months. However, AF burden was reduced by 86% after ablation. More recently, the CIRCA-DOSE trial demonstrated a freedom of AF >30 seconds of about 50% using an ICM, but the AF burden was reduced by more than 99% after ablation.11)
The Heart Rhythm Society consensus document for catheter ablation of AF initially selected the 30 second recurrence cut-off based on the original definition of AF based on a minimum of 30 seconds from an ECG recording. They did not have any evidence to suggest picking any other endpoint. The selection of this endpoint, unfortunately, may have done a disservice to AF ablation since it sets a very high bar for defining success – almost complete elimination of any arrhythmia. A reduction in AF burden is likely a better assessment of success since clinically, many patients may still have a few short recurrences of AF but still feel much better. Before the consensus document can change, however, we need to understand what reduction in AF would be considered an appropriate outcome measure for clinical trials. This might be possible by understanding the relationship between AF reduction and patient QOL as well as AF burden and patient prognosis.
Go to :
QOL AND AF BURDEN
According to international guidelines, the primary indication for AF ablation remains the relief of symptoms caused by AF. The CAPTAF trial12) was designed to compare AF ablation and antiarrhythmic drugs using QOL as the primary endpoint and an ICM to assess AF burden. The investigators found that the QOL measured by the 36-Item Short Form Health Survey and the general health score improved significantly more in the ablation group. This QOL improvement correlated to a significant reduction in AF burden in the ablation group (78%) compared to the drug group (51%). However, the actual freedom from any AF recurrence >30 seconds in the ablation group was only 29.7%.
The CABANA trial13) could not prove a benefit of catheter ablation over antiarrhythmic drugs in the composite endpoint of mortality, stroke, serious bleeding, or sudden death. However, there was a significant improvement in QOL in the catheter ablation group which also correlated to a significant reduction in AF recurrence with ablation compared to drugs (adjusted hazard ratio [HR], 0.52; 95% confidence interval [CI], 0.45–0.60; p<0 .001). But like the CAPTAF trial, the freedom from any AF recurrence >30 seconds in the ablation arm was only about 50% after 3 years.
Clearly, both CAPTAF and CABANA show that many patients will experience an improvement in QOL after catheter ablation without total elimination of the arrhythmia. It could be argued that ablation causes a so-called placebo effect (“patient expectancy bias”) given the invasiveness of the procedure compared to drugs. Some have argued that ablation should be compared to a sham procedure group to remove the expectancy bias. But studies to date do provide a strong link between procedural success and improved QOL. The question is how much reduction in AF burden is required to improve patient QOL? There have been very few studies examining this direct relationship.
In a sub-analysis of the Substrate versus Trigger Ablation for Reduction in AF (STAR AF) I trial, there was a significant improvement in physical health (24%) and mental health (19%) component scores from baseline to 12 months after ablation (p<0.05 for both) for all of the ablation strategies, even though there were differences in procedural outcome.14) However, in a multivariable analysis, AF recurrence did independently predict aggregate QOL score. Furthermore, the study showed that QOL measurements improved in patients with lower AF burdens and did not decrease until the highest quartile of AF burden correlating to a median of 27.2 hours per month (Figure 1).
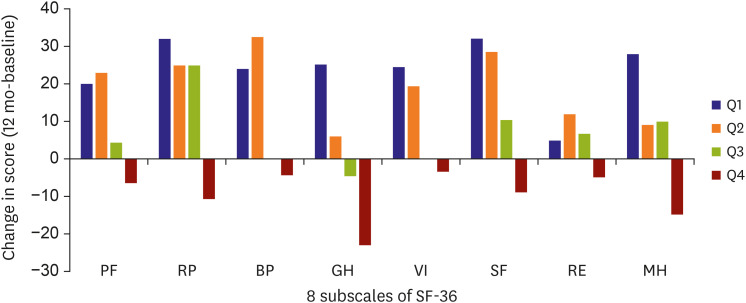 | Figure 1Figure from Mantovan et al.14) Change in 8 subscale values in the 36-Item Short Form Health Survey (SF-36) from baseline to 12 months after ablation for patients with recurrence of AF. Arrhythmia burden was split into quartiles. The quartiles were: 30 seconds to 30.8 minutes (Q1), 30.9 minutes to 1.3 hours (Q2), 1.4 hours to 4.7 hours (Q3), and 4.8 to 720 hours (Q4). For Q1 and Q2, there were significant improvements in the magnitude of change for each of the 8 subscales from baseline to 12 months. For patients in Q3, there was either significant improvement (p<0.03 for RP, SF, RE, and MH) or no significant change (PF, BP, GH, VI). For patients in Q4 there was a significant decrease in all subscales.AF = atrial fibrillation; BP = body pain; GH = general health; MH = mental health; PF = physical functioning; RE = role emotional; RP = role physical; SF = social functioning; VI = vitality.
|
Terricabras et al conducted a sub-study of the STAR AF II trial.15)16) The trial enrolled 589 patients and analyzed the AF burden reduction and the QOL improvement in three different ablation strategy groups; 1) PVI, 2) PVI plus complex fractionated electrograms or 3) PVI plus linear lesions. The QOL assessment was analyzed using the SF-36 and the EuroQol Health-Related Quality of Life 5-Dimension-3-Level (5Q-5D-3L) questionnaires at 12 and 18 months after ablation. AF burden was calculated from weekly trans-telephonic monitor transmissions and patient symptoms. Freedom from AF episodes >30 seconds was only 49% but the AF burden reduction was 92%. All three ablation arms experienced significant improvement in QOL. However, greater reductions in AF burden were associated with greater QOL improvement. Greater than 70% reduction in AF burden was associated with an improved QOL while less than 70% reduction in AF burden did not show the same degree of improvement (Figure 2).
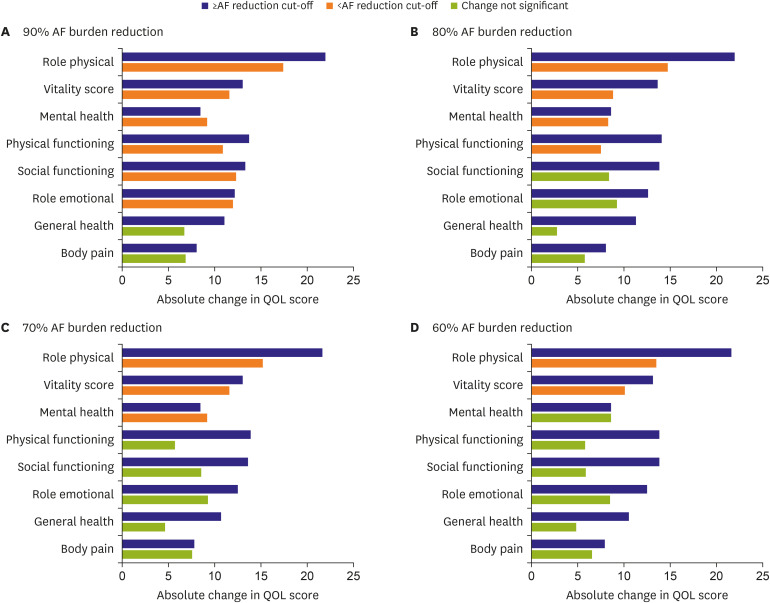 | Figure 2Figure from Terricabras et al.16) Patients with less than 90% AF burden reduction, experienced an improvement in QOL in 6 of the 8 subscales. Patients with less than 80% AF burden reduction, had an improvement in 4 of 8. For patients with less than 70% AF burden reduction, 3 of 8 scales and for patients with less than 60% AF burden reduction, 2 of 8 scales showed a statistically significant positive change.AF = atrial fibrillation.
|
Finally, an analysis from another clinical trial by Essebag et al.17) demonstrated that patients with a decrease in AF of >19 h/month had a significantly greater improvement in QOL and an AF burden <24 h/month at 12-months post-ablation was also independently associated with significant increase in QOL. Thus, it seems clear that if the purpose of ablation is to improve symptoms, the primary end-point shouldn't be freedom from AF episodes as a categorical variable (yes/no) and AF burden gives us a better understanding of actual patient response. The ongoing long-term monitoring for persistent AF and correlation with QOL utilizing ICMs should also provide further data on the correlation of AF burden and QOL. Selected trials that correlate QOL and AF burden are listed in Table 1.

Table 1
AF burden and QOL
| Study | Study design | Sample size | Follow-up (years) | Monitoring | Outcome |
|---|---|---|---|---|---|
| CAPTAF12) | Randomized | 155 | 1 | ICM | Greater increase in QOL among ablation group |
| CABANA13) | Randomized | 2,200 | 4 | IRM (Holter monitoring) | Higher AF burden reduction and improvement of QOL among ablation group |
| STAR AF II substudy15) | Randomized | 589 | 1.5 | IRM (Holter) | Greater reduction in AF is associated with greater improvement in QOL |
| CAPCOST16) | Prospective observational | 230 | 1 | IRM (Holter) | Lower postablation AF burden experienced better improvement in QOL |
AF = atrial fibrillation; ICM = intracardiac continuous monitoring; IRM = intermittent rhythm monitoring; QOL = quality of life.
![]()
Go to :
AF BURDEN AND PROGNOSIS
To justify changing a 30 second clinical trial endpoint to one based on AF burden, understanding the relationship between AF burden and patient prognosis is also important. Piccini et al.,18) performed a case-crossover analysis of the AF burden of 3,131 patients with a cardiac implantable device (pacemaker or defibrillator) who died and had continuous monitoring data from 1 year to 4 weeks preceding death. They found that the presence of more than 6 hours of AF per week was associated with an increased odds of death (odds ratio [OR], 2.30; 95% CI, 2.09–2.53; p<0.001) as well as a week-to-week progression in AF burden greater than 24 h (OR, 12.95; 95% CI, 8.72–19.22; p<0.001).
In 2018, Wong et al.,19) analyzed data from the Asymptomatic Atrial Fibrillation and Stroke Evaluation in Pacemaker Patients and the Atrial Fibrillation Reduction Atrial Pacing Trial (ASSERT) and evaluated the predictors of subclinical AF (SCAF) progression defined as the development of clinical AF or >24 hours of SCAF and its relationship with hospitalization for heart failure.20) A total of 415 patients with a pacemaker and SCAF episodes between 6 minutes and 24 hours were evaluated. During the follow-up, 15.7% of patients experienced progression to SCAF >24 hours or to clinical AF and this progression was associated with a four-fold increased risk of heart failure hospitalization (HR, 4.10; 95% CI, 1.65–10.2; p=0.002). In another study, evaluating SCAF, Gonzalez et al.21) showed that in pacemaker patients, the presence of atrial high-rate episodes (AHREs) as little as 5 minutes or more was associated with a significant increase in cardiovascular mortality (HR, 2.80; 95% CI, 1.24–6.31) and stroke mortality (HR, 9.65; 95% CI, 1.56–59.9).
Finally, in a meta-analysis of AF type, non-paroxysmal AF was associated with a higher mortality than paroxysmal AF even after correction for competing variables (HR, 1.22; 95% CI, 1.09–1.37).22) Based on this data, it would appear that understanding AF burden would be more closely related to patient prognosis than an arbitrary cut-off of 30 seconds.
Go to :
AF BURDEN AND RISK OF STROKE
The major risk associated with AF is a 2 to 3-fold increase in the risk of ischemic stroke. Strokes caused by AF tend to be larger and are also associated with increased mortality.23) Oral anticoagulation (OAC) is effective in mitigating this risk. Catheter ablation has not been shown to decrease the risk of stroke. The HRS Consensus Document on Catheter Ablation of AF suggest that after a successful ablation, the decision to continue OAC should be determined by the stroke risk of the patient and not on the apparent success of the procedure.24) This is not an unreasonable recommendation since DISCERN AF showed that asymptomatic AF episodes continue post-ablation and while these may not affect patient QOL, they still remain a risk for thromboembolic (TE) events.25)26) The question is whether AF burden can be sufficiently reduced to allow discontinuation of OAC post-successful ablation.
Early studies suggest that even minimal burdens of AF are associated with a significant risk of TE events. The ASSERT trial demonstrated that in patients with a pacemaker, as little as 6 minutes of AHRE increased the risk of TE by 2.5 times compared to patients with no AHRE over a follow-up of 2.5 years.20) Similar results were found in an analysis of the Mode Selection Trial in Sinus-Node Dysfunction (MOST) trial,27) where the risk of stroke was increased by a factor of 2.5 in patients who had at least one episode of AHRE. The TRENDS trial (A Prospective Study of the Clinical Significance of Atrial Arrhythmias Detected by Implanted Device Diagnostics) analyzed 2,486 patients with new implanted CIED who had at least one stroke risk factor and no previous history of long-standing persistent AF.28) They found that the TE risk was quantitatively linked to AT/AF burden where AT/AF burden ≥5.5 hours on any day in the most recent 30 days was associated with doubling the risk of TE compared with the zero AF burden (HR, 2.20; 95% CI, 0.96–5.05; p=0.06). Data from both the ASSERT and TRENDS studies also suggest that the occurrence of stroke is not temporally related to episodes of AF, suggesting that even brief episodes of AF may be a marker for stroke risk and that the absence of AF is not protective. All of this data combined would suggest that reduction of AF burden to even small levels would not prevent a risk of stroke and therefore allow for discontinuation of OAC.
On the other hand, more recent evidence demonstrates a stronger link between AF burden and the risk of stroke. A sub-analysis of the ASSERT trial,29) for example, showed that the risk of TE stroke only increased in patients with AHRE lasting more than 24 hours (HR, 3.24; 95% CI, 1.51–6.95; p=0.003) compared to patients without AHRE. But when AHRE burden was <24h, the TE risk seemed to be similar to patients without AHRE. This is consistent with other data suggesting that the TE risk in SCAF appears to be lower than in clinical AF.30)31) A pooled analysis of five prospective observational studies involving patients with previously implanted pacemakers or defibrillators (10.016 patients) showed that while stroke risk increased with higher AF burden, the increase was not as high as suggested by the ASSERT and TRENDS studies.32) For one hour increase in the daily maximum of AF burden, the relative risk for stroke increased by only 3%; a daily maximum of 6 hours of AF increased stroke risk by only 17% and only with 12 h of AF did the risk increase by 37%. And while ASSERT and TRENDS suggested no relationship between the occurrence of AF and stroke, the strokes included in those analyses were not adjudicated to be TE-related events. Many of the strokes were likely lacunar or carotid in origin which would not be related to AF. Other studies have suggested a much stronger link between occurrence of AF and stroke.33)
A study by Kaplan et al.34) reinforces the idea that AF burden is related to stroke and that brief AF recurrences may not warrant OAC. The authors of this study extracted data from administrative health databases on 21,768 patients with implanted devices and a history of AF. They observed an interaction between AF burden and CHA2DS2-VASc that could shift the stroke risk above or below the threshold required for anticoagulation. In patients with an AF burden between 6 minutes and 23.5 hours, a CHA2DS2-VASc score of more than 3 is required to justify OAC, while a duration of AF 24 hours or more would justify OAC at a CHA2DS2-VASc score of 2. Selected studies that correlate AF burden and risk of stroke in patients with CIED are listed in Table 2.
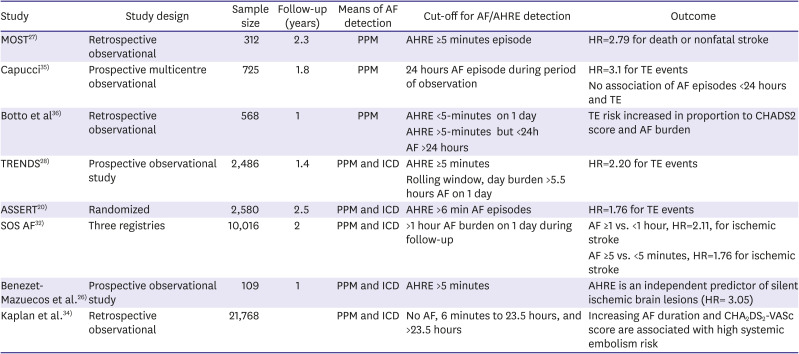
Table 2
Studies of AF burden and risk of stroke in patients with CIED
| Study | Study design | Sample size | Follow-up (years) | Means of AF detection | Cut-off for AF/AHRE detection | Outcome |
|---|---|---|---|---|---|---|
| MOST27) | Retrospective observational | 312 | 2.3 | PPM | AHRE ≥5 minutes episode | HR=2.79 for death or nonfatal stroke |
| Capucci35) | Prospective multicentre observational | 725 | 1.8 | PPM | 24 hours AF episode during period of observation | HR=3.1 for TE events |
| No association of AF episodes <24 hours and TE | ||||||
| Botto et al36) | Retrospective observational | 568 | 1 | PPM | AHRE <5-minutes on 1 day | TE risk increased in proportion to CHADS2 score and AF burden |
| AHRE >5-minutes but <24h | ||||||
| AF >24 hours | ||||||
| TRENDS28) | Prospective observational study | 2,486 | 1.4 | PPM and ICD | AHRE ≥5 minutes | HR=2.20 for TE events |
| Rolling window, day burden >5.5 hours AF on 1 day | ||||||
| ASSERT20) | Randomized | 2,580 | 2.5 | PPM and ICD | AHRE >6 min AF episodes | HR=1.76 for TE events |
| SOS AF32) | Three registries | 10,016 | 2 | PPM and ICD | >1 hour AF burden on 1 day during follow-up | AF ≥1 vs. <1 hour, HR=2.11, for ischemic stroke |
| AF ≥5 vs. <5 minutes, HR=1.76 for ischemic stroke | ||||||
| Benezet-Mazuecos et al.26) | Prospective observational study | 109 | 1 | PPM and ICD | AHRE >5 minutes | AHRE is an independent predictor of silent ischemic brain lesions (HR= 3.05) |
| Kaplan et al.34) | Retrospective observational | 21,768 | PPM and ICD | No AF, 6 minutes to 23.5 hours, and >23.5 hours | Increasing AF duration and CHA2DS2-VASc score are associated with high systemic embolism risk |
AF = atrial fibrillation; AHRE = atrial high-rate episode; CIEDs = cardiac implantable electronic devices; HR = hazard ratio; ICD = implantable cardioverter-defibrillator; OR = odds ratio; PPM = permanent pacemaker; TE = thromboembolic.
![]()
Go to :
CONCLUSIONS
In this article, we have shown how AF burden may be a superior methods by which to assess outcome after AF ablation. Reduction of AF burden may be a more accurate reflection of procedural success than a time to event analysis basing success on a single recurrence >30 seconds. Furthermore, AF burden correlates better to changes in QOL as opposed to dichotomous definitions of success. And finally, AF burden may be a better predictor of prognosis and stroke risk than a single measure of AF. For this reason, we believe that future guidelines will eventually adopt AF burden as the best outcome measure for effectiveness of catheter ablation.
Go to :
 XML Download
XML Download