

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cardiovascular disease (CVD) is the leading cause of death worldwide, accounting for nearly one-third of all deaths.1)2) The same holds true for Korea, where heart disease has been the leading cause of death for nearly a decade.3) Since a significant portion of CVD is preventable, the importance of adequate prevention strategies has long been emphasized.4) To implement such strategies and subsequently reduce the burden of CVD, magnitude and temporal trends in mortality, morbidity, and risk factors of CVD need to be clearly identified. In Korea, the Statistics Korea (formerly the National Statistical Office) has annually released anonymized data on the causes of death since 1983 based on the death registry.3) The temporal trend in CVD mortality has been repeatedly reported with this data.5)6)7) On the contrary, nationally representative data on CVD morbidity are extremely limited, making it difficult to accurately assess the incidence and prevalence of CVD in Korea. Although there have been several studies estimating the burden of CVD using the National Health Insurance claims data that cover the entire Korean population,8)9)10)11)12)13) most of the studies were confined to specific disease categories, such as myocardial infarction (MI),8)9) cerebrovascular diseases,10)11) or heart failure (HF).12)13) Moreover, substantial heterogeneity in study methods makes it inappropriate to compare their results directly. Regarding cardiovascular risk factors, fact sheets describing the prevalence and management status of hypertension, diabetes, dyslipidemia, obesity, and metabolic syndrome have been published by affiliated academic societies of Korea.14)15)16)17)18) Nonetheless, comprehensive data summarizing the overall status of CVD in Korea has not been reported yet. Thus, we analyzed the temporal trends in CVD mortality, hospitalization, and risk factors based on nationally representative datasets on behalf of the Korean Society of Cardiology.
METHODS
Ethical statement
The present study complied with the Declaration of Helsinki and was approved by the Institutional Review Board of Yonsei University Health System, Seoul, Korea (No. 4-2020-0207). Informed consent was waived since this is a retrospective study of de-identified administrative data.
Classification of circulatory system diseases
All diseases of circulatory system were categorized into heart diseases, cerebrovascular diseases, and other circulatory diseases. Heart diseases were further classified into subcategories, including ischemic heart diseases (IHD), HF, and hypertension. MI was considered a subcomponent of IHD. The overall classification scheme and corresponding International Classification of Diseases-10 (ICD-10) codes are presented in Table 1.
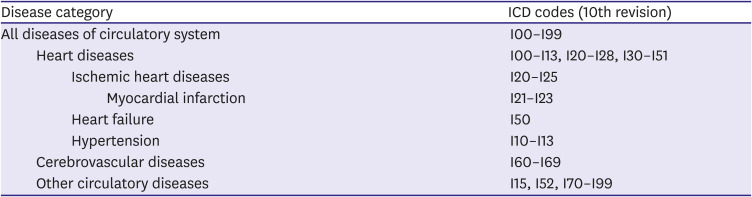
Table 1
Classification of cardiovascular diseases
![]()
Assessment of cardiovascular disease mortality
The Korean Statistical Information Service-Microdata Integrated Service (KOSIS-MDIS) covers the entire resident-registered population and a portion of unidentified individuals in Korea. Based on mortality data provided by the KOSIS-MDIS, we calculated the annual CVD mortality rate between 1983 and 2018. In addition, age-standardization was performed by the direct method to adjust for changing population structures over time. Specifically, the standardization was performed with the population structure of the resident-registered population in 2018 as a reference, separately by sex.
Assessment of cardiovascular disease hospitalizations
Using National Health Insurance Big Data (NHIBD), we evaluated the magnitude and temporal trends of CVD hospitalizations between 2002 and 2018 among adults aged ≥20 years covered by the National Health Insurance.19) For each year, we estimated the number of people hospitalized for CVDs. Then, CVD hospitalization rate was defined as the number of people hospitalized for CVD over the total number of insured people in that year. Age-standardized hospitalization rates were calculated with the direct method based on the population structure of insured people in 2018. As a diagnosis code for hospitalization can be recorded either as a primary diagnosis or other diagnoses, numbers of adults hospitalized for CVDs were estimated separately based on (1) primary diagnosis and (2) all diagnoses during hospitalization.
Assessment of cardiovascular risk factors
Using the Korea National Health and Nutrition Examination Survey (KNHANES) data, we assessed the current CVD risk factor distribution among adults aged ≥20 years who completed the KNHANES in 2018. The five major CVD risk factors included hypertension, diabetes, hypercholesterolemia, obesity, and current smoking (Table 2). We estimated the number of adults with each risk factor based on the weighted prevalence calculated from the KNHANES data. The number of adults with dyslipidemia was also assessed. Subsequently, we categorized the participants by the number of major risk factors (0, 1, 2, and ≥3) and examined its distribution by age and sex. All analyses of the KNHANES data accounted for the complex survey design adopted in the KNHANES to generate nationally representative estimates for the noninstitutionalized Korean population.20)
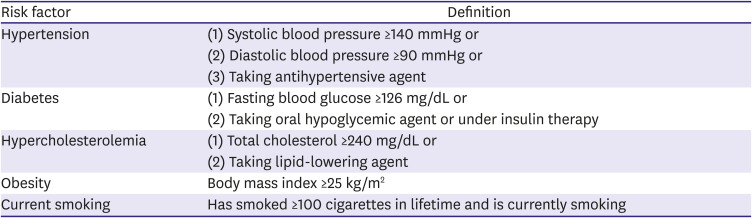
Table 2
Definition of cardiovascular risk factors
Additionally, dyslipidemia was defined as (1) low-density lipoprotein cholesterol ≥160 mg/dL or (2) triglyceride ≥200 mg/dL or (3) high-density lipoprotein cholesterol <40 mg/dL or (4) taking lipid-lowering agent.
![]()
RESULTS
Cardiovascular disease mortality
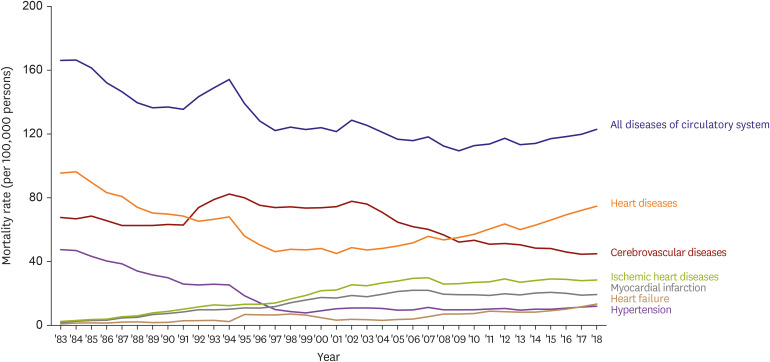
The mortality rate due to all diseases of circulatory system declined until 2010 and steadily increased afterward up to 123 per 100,000 persons in 2018 (Figure 1, Supplementary Table 1). Such shift is most likely due to population aging, as the age-standardized mortality rate has continued to decrease even after 2010 (Supplementary Figure 1). There was also a transient peak in circulatory system diseases mortality around 1994 when the ICD system was revised from 9th to 10th revision. In the last decade, mortality due to heart diseases, IHD, HF, and hypertension have increased. During the same period, mortality due to MI has been stagnant, whereas cerebrovascular diseases mortality has declined (Figure 1, Supplementary Table 1). Further details on the 36-year trend of mortality from diseases of circulatory system in Korea are presented elsewhere.21)
Hospitalization for cardiovascular diseases
Since 2002, the numbers of adults hospitalized for all diseases of circulatory system, heart diseases, and cerebrovascular diseases have consistently escalated based on both primary and all hospital diagnoses (Figure 2). Between 2002 and 2018, the number of people hospitalized increased 3.7 fold (from 169 thousand to 630 thousand) for all circulatory system diseases, 3.7 fold (from 91 thousand to 333 thousand) for heart diseases, and 3.5 fold (from 65 thousand to 227 thousand) for cerebrovascular diseases based on primary diagnosis (Figure 2A). Based on all hospital diagnoses, the number increased 4.5 fold (from 444 thousand to 1,994 thousand) for all circulatory system diseases, 4.1 fold (from 391 thousand to 1,600 thousand) for heart diseases, and 4.5 fold (from 105 thousand to 474 thousand) for cerebrovascular diseases (Figure 2B).

The hospitalization rate for all circulatory system diseases based on primary diagnosis also increased to 1,455 per 100,000 persons in 2018 (Figure 3A, Supplementary Table 2). The hospitalization rates for heart diseases and those for cerebrovascular diseases increased until 2016; after that, the heart diseases hospitalization rate continued to grow, while the cerebrovascular diseases hospitalization rate started to decline. Among heart diseases, the hospitalization rate due to HF exhibited the greatest increase (3.5-fold), followed by hypertension (2.7-fold), IHD (2.6-fold), and MI (1.9-fold) (Figure 3A, Supplementary Table 2).
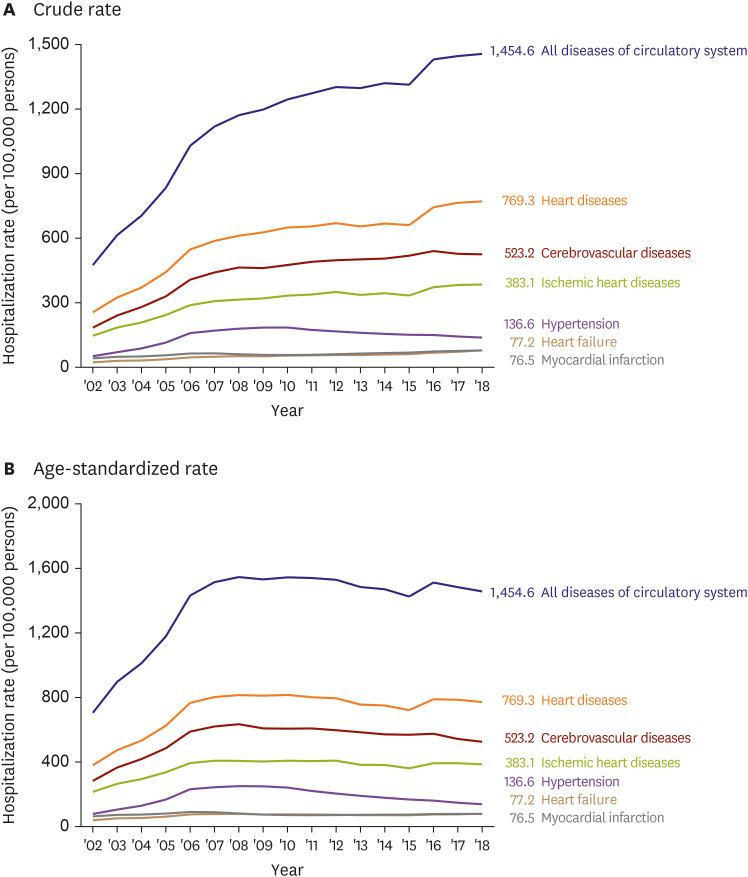
Again, such trends could be attributed in part to population aging in Korea. The age-standardized hospitalization rates for all circulatory system diseases and their components had continually risen until 2009. (Figure 3B, Supplementary Table 3) Since then, the hospitalization rates for all circulatory system diseases, heart diseases, and cerebrovascular diseases have slowly declined. At the same time, the hospitalization rate for hypertension also decreased steadily, while the rate for HF declined until 2015 and increased thereafter. The hospitalization rate for IHD remained stagnant until 2012 then fluctuated. On the contrary, the hospitalization rate for MI decreased until 2011 then increased afterward (Figure 3B, Supplementary Table 3).
Cardiovascular risk factors
In 2018, approximately 12.1 million adults had hypertension, 4.3 million had diabetes, 8.7 million had hypercholesterolemia, 14.9 million were obese, and 8.8 million were currently smoking (Figure 4). The proportion of people with ≥2 risk factors rapidly increased with older age, ranging from 14.7% in the age group of 20-29 years to 58.4% in the age group of ≥70 years. Moreover, 27.8% of people aged ≥70 years had 3 or more cardiovascular risk factors (Figure 5A). This age-related trend was apparent in both sexes. Whereas men had a greater number of risk factors until age 70, the number surpassed among women at age >70 years (Figure 5B and C).


DISCUSSION
CVD mortality has increased during the last decade in Korea. Such increment was mainly driven by heart diseases, while mortality due to cerebrovascular diseases has declined over the past 2 decades. Hospitalization for CVD has also continually increased, with every CVD category showing a 2-3-fold increase between 2002 and 2018. Age-standardization revealed that the aforementioned increases in mortality and hospitalization were attributable, at least in part, to the population aging in Korea. As to cardiovascular risk factors, a high proportion of Korean adults were carrying more than one risk factor, and the number of risk factors escalated with older age.
Considering the rapid population aging in Korea, the continued increase in CVD hospitalization and mortality appears inevitable. Moreover, the age-dependent distributions of cardiovascular risk factors imply an even greater burden predicted in the future. Thus, concerted and sustained efforts are crucial among healthcare professionals, policymakers, and the general population themselves to achieve early prevention and subsequently reduce the burden of CVD in Korea.
 XML Download
XML Download