

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
In late December 2019, the highly infectious new coronavirus disease 2019 (COVID-19) emerged in Wuhan, China, and rapidly spread around the world.1 In Korea, the first COVID-19 patient was reported in January 2020.2 In the early stage of the COVID-19 outbreak in Korea, most cases were concentrated in Daegu, which is 150 miles from the capital city of Seoul. However, as the number of cases and deaths increased, fear of infection spread throughout the country. During the COVID-19 pandemic, health care workers (HCWs) were exposed to a variety of new and unprecedented scenarios, and experienced a range of emotions in response to the critical situation. COVID-19 has caused high levels of perceived stress and has increased the mental health burden for HCWs.3 Exposure to work-related stress can lead to burnout in HCWs, which can subsequently reduce the quality of patient care.45 On March 2, 2020, South Korea established community treatment centers for the isolation and monitoring of patients with no or mild symptoms of COVID-19 during the pandemic. Medical and operating staff were dispatched to these centers, which faced a major shortage of medical resources because the demand far exceeded the supply.6
The COVID-19 outbreak has continued for more than 1 year, and researchers in several countries have studied its impact on HCWs. HCWs in a variety of fields have reported physical and mental health problems, including respiratory symptoms, fatigue, anxiety, depression, and distress during the COVID-19 pandemic.7 However, few studies have examined the views and experiences of multidisciplinary HCWs employed during this period. A comprehensive understanding of the experiences of multidisciplinary HCWs during the COVID-19 pandemic could improve healthcare systems around the world, especially in terms of their responses to future disasters. Thus, in the present study, we conducted an in-depth exploration of the experiences of multidisciplinary HCWs (including all workers who interacted with patients, including physicians, nurses, other medical practitioners and cleaning staff) in several centers during the COVID-19 outbreak in South Korea.
Go to : 
METHODS
Study design and participants
This study was conducted in three designated COVID-19 hospitals and one community treatment center in three major cities in South Korea (Seoul, Daegu, and Gwangju) from 18 November to 30 December 2020. We conducted semi-structured and face-to-face interviews with four focus groups to investigate the vocational issues encountered while working in a healthcare setting during the COVID-19 epidemic. Using purposeful sampling, we recruited eligible participants who directly or indirectly cared for patients during the COVID-19 epidemic. We included HCW directly caring for patients, such as physicians, nurses, and hospital managers, as well as laboratory technicians and maintenance workers potentially exposed to infectious materials. HCWs who declined to participate in the focus group interview were excluded. Because our aim was to examine the views and experiences of various HCWs, each group comprised participants with many different job titles from several wards (Table 1).
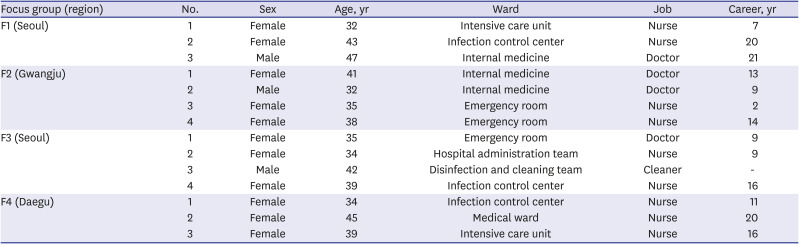
Table 1
Profile of interview participants
F1: Participants who directly cared for severe COVID-19 patients in a nationally designated hospital. F2: Participants who worked in screening test center for COVID-19 in a nationally designated hospital. F3: Participants who worked in community treatment center for asymptomatic and mild COVID-19 patients. F4: Participants who indirectly cared for COVID-19 patients in a nationally designated hospital.
COVID-19 = coronavirus disease 2019.
![]()
Four psychiatrists discussed the interview structure and completed a practice interview. The interview focused on the views and experiences of HCWs providing care and assistance to COVID-19 patients. The final semi-structured interview included the following main questions: “What kinds of difficulties did you experience when providing COVID-19-related medical care?,” “How did you feel when working during the COVID-19 epidemic?,” “What changed in your life during the COVID-19 epidemic?,” “What are the main psychological and physical problems that you have encountered?,” and “What were your responsibilities and obligations during the COVID-19 epidemic?.” The HCWs who agreed to participate in the study were asked to sign an informed consent form. The interviews lasted for approximately 60 minutes.
Data collection
We obtained demographic and work-related information from the study participants before the interviews. The lead researcher (a psychiatrist) conducted a semi-structured face-to-face interview with each participant in a convenient and confidential location. The lead researcher maintained a neutral attitude when collecting the data and established a good relationship with each participant via active listening and clarification of any issues, guiding the discussion according to the interview outline by asking the research questions, encouraging the participants to discuss their experiences and ideas, and asking follow-up questions to further develop any emergent themes. The interviews were tape-recorded, or recorded verbatim, with the permission of the participants.
Data analyses
We employed the consensual qualitative research (CQR) approach to analyze the data and capture the unique experiences of healthcare professionals providing COVID-19-related medical care.8 CQR is an inductive method of describing phenomena. CQR is useful for investigating the in-depth experiences of individuals.8 According to CQR guidelines, research team members should reach a consensus regarding all analysis decisions. The research team in this study had four members. Before collecting the data, all team members participated in a discussion, in which they shared their expectations and biases. The aim of this exercise was to reduce subjectivity in the data collection and analyses. Each team member reviewed the data independently and generated a list of domains (themes).
The research team reached a consensus on the domain list through discussion, independently coded the transcripts, and then reviewed the transcripts coded by the other team members. The domain list was continuously revised until a consensus was reached. The themes of the interviews were extracted and summarized clearly and concisely.
The research team then identified subthemes in each domain by reading the transcripts several times. The domains and subthemes were coded by multiple research team members. The CQR analysis process continued until a consensus was reached regarding the domains, subthemes, and core ideas. An auditor reviewed the results to ensure that the raw data were categorized accurately, and that the core ideas appropriately reflected the data.9 The research team assimilated the auditor's feedback.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of the National Medical Center (IRB No. NMC-2010-081). All subjects provided informed consent upon study enrollment.
Go to :
RESULTS
Our main focus was on the experiences of HCWs providing COVID-19-related medical care. The data analysis yielded four domains: work-related struggles, personal life-related struggles, psychological stress, and health-related struggles. Table 2 presents the main domains and subthemes.
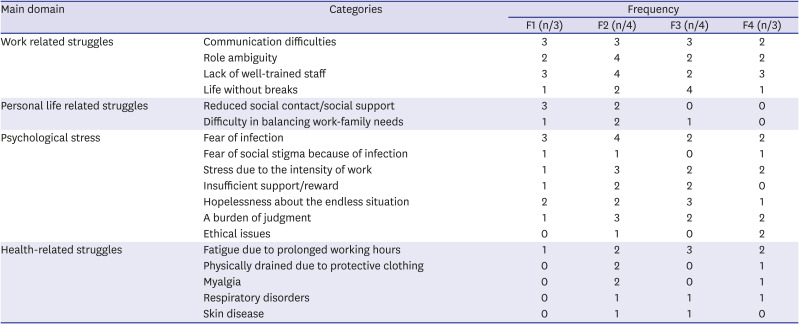
Table 2
The main domains and sub-categories extracted from the data analyses
![]()
Domain 1: work-related struggles
This domain refers to the difficulties that HCWs experienced in providing COVID-19-related medical care, such as conflicts with patients and guardians, the media, and government officials. Four subthemes emerged: “communication difficulties,” “role ambiguity,” “lack of trained manpower,” and “life without a break.”
Communication difficulties
Communication difficulties refers to conflicts among medical staff, and between medical staff and patients, the media, and governmental officials. When an organization has an ambiguous division of work and lacks a well-established system, many conflicts can occur between its members. The vertical communication in the medical community has become problematic. In some cases, patients or their families strongly complained about the COVID-19 examination fee or quarantine process. Communication difficulties may also occur in the context of the administrative process, such as when media representatives report confidential information or the same data are requested in different formats by various official departments. Excerpts from the interviews follow:
“It was not easy to respond to people complaining about paying for the test in a nationally designated testing site. In some cases, we were forced to discard samples taken from people who left without paying for their test.” [F2_3]
“We did not hide COVID-19-related information, but we felt stressed when people falsely blamed hospitals and became angry about non-transparency and the slow release of information.” [F1_2]
“I directed my questions to the infection control center, which is the hospital's COVID-19 ‘control tower’, when I had any questions about COVID-19. However, the infection control center did not respond to my inquiries right away. This was stressful because patients wanted immediate feedback from me.” [F2_3]
“My request to the department's overall supervisor was not accepted, and I was notified that I should follow the supervisor's decision.” [F1_1]
Role ambiguity
Regardless of the job type and work environment, the medical staff reported that the division of COVID-19-related work was ambiguous and needed to be improved. When there is an increase in the workload and number of complaints, employees are more likely to be asked to take over projects that were previously the responsibility of another employee. Moreover, the same individuals were repeatedly dispatched from their departments to handle COVID-19-related work, which may not have been ideal. The need for a fairer system for recruiting and deploying personnel was cited by all of the focus groups. Finally, the HCWs reported that they took on additional COVID-19-related work even if their existing workload had not been reduced:
“We had to prepare for emergencies because the COVID-19 situation was prolonged. However, there was a problem with the division of work among the staff. Medical staff in the infection control center had too many tasks, and the patients had a wide variety of physical conditions, making it difficult to complete all of the tasks efficiently. However, staff in other departments thought that all of the COVID-19-related work was the responsibility of the infection control center.” [F1_2]
“Complaints about COVID-19 were directed to the infection control center by all of the staff, patients, and patients' guardians. However, it was difficult for me to respond to all of the complaints and questions.” [F4_1]
“I asked myself why I should handle all of these things by myself when there were so many other medical staff besides me. I already had many things to perform before the COVID-19 pandemic, but I was completely overwhelmed after the COVID-19 outbreak.” [F2_1]
Lack of well-trained staff
A shortage of trained staff occurred because of the prolonged health crisis, so many temporary HCWs were recruited. Even with this measure, all of the focus groups identified a lack of trained HCWs as one of their stressors. This led to a heavy workload, because considerable time and energy is needed to train new employees. Furthermore, newly recruited employees often quit after experiencing a heavy workload, leading to a vicious circle in which staff were constantly educating new employees:
“As the COVID-19 situation became more prolonged, all of the nurses except me had been dispatched from other departments. Thus, many nurses in my department had limited work experience. Most of the patients who came to testing clinics or emergency rooms were cared for by nurses who had only been working in those departments for a month or two. It was stressful to train the nurses who had been sent from other departments.” [F2_4]
“Critically ill patients need to receive care from specialized nurses. However, the number of nurses who are specialized in the care of critically ill patients is small. The workloads of nurses in the intensive care unit (ICU) were not reduced, because nurses in other departments were dispatched to the ICU. However, these nurses lacked the skills needed to care for critically ill patients. Thus, while the number of nurses in the ICU increased, few of those could effectively help me.” [F1_1]
“It was incredibly challenging to perform complicated (skilled) procedures, such as cardio-pulmonary resuscitation, because 60% of staff were novices.” [F4_3]
Life without a break
All groups reported a lack of breaks at work, and no distinction between being on and off work:
“I had received over 10 calls while at home, some of them even at dawn, and I felt like I was working all day. I had to come out to work in the early morning, and even on an off-duty day when a patient had a critical medical problem. So, I felt like I was working all year.” [F4_1]
“I got many calls from unknown numbers 24 hours a day. The hospital staff, employees in the Centers for Disease Control and Prevention, and those at the manager level above the lead nurse kept contacting me on both weekdays and weekends. I felt like I was a call-center employee, because I had to answer the phone at any time.” [F3_4]
Domain 2: personal life-related struggles
The “personal life-related struggles” domain refers to the difficulties that arose in the personal lives of the medical staff in charge of COVID-19-related work. This domain comprises two subthemes: reduced social contact/social support, and difficulty in balancing work–family needs because of increased work intensity and worrying about the possibility of infecting others.
Decreased social support
The HCWs reported that, as they increasingly dealt with patients who were positive for COVID-19, they reduced their social activities because they were worried about being infected. They also chose to isolate themselves because of other people's prejudices against people who were in close contact with positive cases. Therefore, they reported reduced perceived social support:
“I chose to isolate myself from my family. I think it has been like that for over 6 months. I currently live alone and physical distance myself from my friends and family.” [F1_1]
“I have experienced other people's avoidant behaviors. In particular, a woman who lives next door to me pressed against the wall to keep her distance from me when we took the elevator together. We used to have small chats before the COVID-19 pandemic began.” [F1_3]
Struggles in maintaining a balance between work and family
The HCWs reported that excessive workloads greatly reduced the amount of time and energy that could be devoted to family or personal life. Expectations and needs regarding the caretaking role at home also increased, because children and students were partaking in online classes from home:
“I didn't want to do anything at home, and I just collapsed when I got back from the hospital because I was so exhausted. I have an elementary school child in a lower grade level, and my child is in a virtual class. I needed to help with my child's homework assignments. However, I felt that I couldn't take good care of my child because I was so exhausted.” [F2_4]
“I couldn't take care of my child during the early adjustment period in elementary school. It was frustrating because I couldn't take care of my child before he entered middle school. With the COVID-19 pandemic, my child has had more free time. However, I became busier because it is a national emergency. Thus, I needed to cooperate with our government's efforts to fight against COVID-19. It is a challenging situation because my child misses my care.” [F1_2]
Domain 3: psychological stress
The psychological stress domain refers to healthcare providers' concerns in terms of safety, occupational, economic, and social issues. This domain includes the following subthemes: “fear of infection,” “fear of social stigma regarding infection,” “stress due to the intensity of work,” “insufficient support/reward,” “burden of judgment,” and “hopelessness about the endless situation.”
Fear of infection
The medical staff who dealt with confirmed cases of COVID-19 expressed anxiety about infection, regardless of where they worked. They perceived a high risk of infection and were worried about the potential effect on their patients and families if they acquired the virus:
“The ICU mainly performs high-risk procedures, and the staff in the ICU are regularly exposed to patients' body fluids. Thus, I have a great fear of infection. I once cared for a patient who complained of dizziness, and the patient then tested positive for COVID-19. Thus, I had to self-quarantine for 2 weeks. While I was on my way home, I was informed that I had been in contact with a confirmed COVID-19 patient. Thus, I was worried that my family would become infected with COVID-19 as a result of contact with me.” [F4_3]
“I was very fearful about getting infected when I changed my work clothes. It is probably easier to become infected by picking up staff members' clothes than to get infected by direct contact with a confirmed COVID-19 patient. I was afraid to pick up the clothes that the staff took off.” [F3_3]
Fear of the social stigma of infection
In Korea, the travel routes of confirmed cases are publicly disclosed. The surveyed healthcare providers feared that they would be misunderstood or criticized after disclosing their travel routes. Given its uniqueness, this fear was considered different from the fear of actual infection:
“I drove early in the morning to buy a house in another province. If I become infected and spread the virus to this area, I will be socially ostracized. Even though I had to go there to buy my house, I was very worried. If I test positive for COVID-19, the government will track my movements, and my movements will be released to the general public. If this happens, people are likely to blame me for traveling to another province.” [F2_2]
Stress due to the intensity of work
Officials at screening clinics and life treatment centers, as well as members of focus group 2, who had to respond to COVID-19 but had no experience of responding to Middle East respiratory syndrome (MERS), reported higher stress than those in focus group 1, who had experience of responding to the MERS outbreak:
“I had experience responding to the MERS outbreak a few years ago, but I was worried that I would face new challenges during the COVID-19 outbreak. I was afraid that my work intensity would increase a lot and that I would not have my normal personal life for several months.” [F1_2]
“I had a lot of anger. It seemed like everyone was trying to do what they wanted to do while not taking on challenging tasks. Manpower should be assigned according to workload, but this did not happen. So I got angry; I may have an anger disorder.” [F2_1]
“I thought a hospital was not the right place to work, and I felt I had to quit my job at my hospital when I started working on the COVID-19-related assignments.” [F2_3]
“I had so much work to do, and I was always busy working until midnight. I had to complete my assignments by early the next morning because of administrative needs. I didn't think such paperwork was necessary at that time.” [F3_2]
Insufficient support and reward
The surveyed healthcare providers also complained that they often received unfair treatment or inadequate emotional and financial support, despite their sacrifices and efforts as frontline workers. In some cases, nurses were upset because they had to take on chores outside of their job description (e.g., cleaning up garbage). Likewise, administrative workers felt it was unfair that they did not receive additional emergency wages like doctors and nurses. The medical doctors reported that they considered their additional wages to be lower than expected, and that the method for calculating compensation was insufficient:
“I saw a lot of donations to the medical staff. Food donations came to the screening clinic. However, when the medical staff ate they threw trash on the floor. I was upset while cleaning up the trash, although I am in a low-level position.” [F3_3]
“I was suddenly dispatched to the treatment center, and I took only a day off after working from 7 pm to 1 am for 41 days. However, the salary I received for this work was simply set at the rate for less than 8 hours per day, and I felt that this was not sufficient considering the risk associated with the work.” [F3_3]
The burden of making professional decisions
Doctors reported that they felt greatly burdened by having to make many critical decisions during the pandemic. When they had to make a judgment about something outside their area of expertise, they felt especially hesitant about whether they had made the right choice:
“I got phone calls asking for my opinion about X-rays, even at dawn. I was told that other departments couldn't cooperate right away. I didn't want to do it early in the morning, but I had no other choice. I had to take all responsibility for my professional opinion. Other staff said that a patient had COVID-19 symptoms, and the staff asked me to decide whether or not the person needed additional tests. That was not easy to do.” [F2_1]
“I had to complete a lot of tasks within a short period of time. This was a burden because other departments were also waiting for my decisions.” [F3_2]
“It was difficult for me to decide on the screening tests because it was not my area of expertise. It was not easy because I was told to continue working in an area where I was not specialized. I received some compensation for this, but I was not sure if it was an appropriate practice.” [F2_1]
Hopelessness about the endless situation
The results for this domain were similar to those for the stress caused by the intensity of work. The only difference was that the healthcare providers reported experiencing feelings of anger and exhaustion because of the need to endure the current health crisis without knowing how long it would last:
“I can perform my regular duty, as it is within my capabilities. However, things got worse, and exceeded my comfort zone and capabilities. The situation did not seem to get any better. Thus, it was challenging for me.” [F2_1]
“I was easily upset simply by meeting patients when I had much hard work to do. I was thinking, “How long should I keep doing this, because it seems to have no end?” There were times when I got angry for no reason because I had given up my entire personal life for endless assignments.” [F2_4]
Domain 4: health-related struggles
The health-related struggles domain pertained to changes in the health status of medical staff while performing COVID-19-related work. Five subthemes were derived: fatigue because of prolonged working hours (“I feel too tired to do anything when I go home”), physical depletion because of protective clothing (“wearing protective clothing requires considerable physical energy”), myalgia, respiratory disorders, and skin diseases. Some participants also reported joint pain and panic (“feelings of falling after not having a break for 3 hours”):
“I was able to take a break in a break room at my hospital. However, I experienced skin problems because I had worn protective equipment and a mask for 7–8 hours straight. I had to wear my gloves in duplicate, so my hands couldn't breathe. So I sweated and bled. I went to a dermatologist. I applied dermatology ointment under my gloves, and took them off for a while when no patients were present. My hands were itchy at bedtime, and I was scratching my hands without knowing it.” [F2_3]
Go to :
DISCUSSION
To the best of our knowledge, this study is the first to focus on the experiences of hospital staff during the COVID-19 outbreak in South Korea, and to use qualitative methods to investigate these experiences and vocational issues. Our aim was to obtain the views on a range of topics of medical professionals who worked during the COVID-19 pandemic.
The COVID-19 pandemic has transformed the healthcare system, and HCWs have been confronted by serious challenges in the workplace.1011 In terms of communication, HCWs were affected by communication difficulties between patients and infection control centers. For instance, complaints from patients about unexpectedly high bills or expensive prescriptions were inadequately handled and associated with staff shortages.12 The participants in the present study reported that more equitable task distribution was necessary to protect HCWs from stress when operating outside of their own field of expertise. Furthermore, HCWs reported feeling overwhelmed by rapid modifications to policies and guidelines,1314 which create confusion and distress for workers.7 Our study showed that communication difficulties and a lack of adequate guidelines were associated with role ambiguity and work overload. Role ambiguity refers to the lack of clarity about duties and responsibilities needed to fulfill one's role.15 Many studies have identified role ambiguity as a source of job dissatisfaction and psychological withdrawal from the work group.1617 During times of crisis and evolving care needs, it is important to establish effective information and communication platforms with standardized guidelines to support HCWs. In this study, because of the sudden outbreak of COVID-19, temporary HCWs from other departments (rather than well-trained staff) were required to participate in COVID-19-related work. Although these staff received pre-job training before starting their duties, their skills were obtained during brief training programs; this may have reduced their work efficiency and quality. During this outbreak, early training and confidence in professional skills have increased staff willingness to actively participate in anti-epidemic work.18 Continuous medical training regarding how to deal with public-health emergencies is needed.19 Furthermore, sustainable health care systems with staff skilled in infection management and advanced human resources planning would be beneficial. Consistent with our findings, most HCWs in previous studies indicated that the way that their work was organized during the COVID-19 epidemic did not allow them to get enough rest, leaving them feeling exhausted.20 As pointed out by other authors,2122 medical centers need to provide breaks to meet basic needs and allow the venting of emotions.
The continuing COVID-19 crisis has changed the lives of HCWs considerably. The participants in the present study reported that they experienced difficulty in balancing work with caring for their families. Our findings were consistent with previous studies23 showing that HCWs voluntarily restricted their social activities, leading to feelings of social isolation. Social isolation, i.e., having few social relationships, is a risk factor for the development of loneliness (the subjective feeling of being isolated).24 Social isolation and loneliness have been identified as major risk factors for stress, depression, and anxiety.2526 Psychological interventions and strategies are needed to increase social support, as are coping skills to improve the emotional state of HCWs during the COVID-19 pandemic.
Regarding fear of infection, consistent with prior reports, the HCWs in our study feared becoming infected with COVID-19,2728 and thus increasing the risk of contagion within their families. The susceptibility to, and mortality associated with, infectious diseases can intensify anxiety and fear among HCWs, potentially affecting their health and work efficacy during an epidemic.29 As in our study, this feeling was especially evident among HCWs in ICUs30 who had to manage the risk of contagion31 and had witnessed COVID-19 patients dying,32 which led to an intense fear of infection. The cleaning staff in our study also reported a fear of infection while at work. Cleaning staff who were not equipped with the appropriate protective equipment may have had more fear of infection during the disinfection and cleaning of contaminated objects and clothing.33 The inadequate protection of HCWs in all health care settings raises professional and ethical issues about the extent of their duties.34 Organizational managers should provide infection-control protocols and sufficient protective equipment for all HCWs, including medical staff.
Another psychological stressor experienced by HCWs is social stigma. Since HCWs come into contact with groups susceptible to infection, they may have been stigmatized during the COVID-19 pandemic. Particularly, HCWs were more likely to believe that people spoke negatively or gossiped about them,35 leading to higher rates of stress and burnout.3637 In our study, one participant feared that he would be criticized more harshly than the general public after disclosing his travel route during the pandemic. There is also evidence that social stigma prevented HCWs with various responsibilities from responding appropriately.38 Hence, psychological support should be available for HCWs during the various stages of isolation and treatment.39
In terms of the intensity of work, our data indicate that some HCWs experienced overwhelming work demands due to an imbalance between workload and human resources, and to additional administrative tasks. Moreover, one participant described experiencing feelings of anger on recognizing this work overload. Negative emotions related to overwork have been reported not only in Daegu, which is had the largest outbreak in the early period of the COVID-19 pandemic among all cities in South Korea, but also in other regions. In our study, stress due to the intensity of work was reported by HCWs not only in designated COVID-19 hospitals, but also in community treatment centers for patients with mild COVID-19. Our findings suggest that during pandemics, the employment conditions for HCWs should be framed within the context of the job-demand resources model. This could reduce burnout and increase job engagement via resources such as performance feedback in the face of high work demands, as well as help prevent exhaustion, burnout, and other mental health issues.40 Despite work overload during the pandemic crisis, HCWs reported feeling that they were insufficiently and unfairly compensated for their efforts. Psychosocial risk factors in the work environment are magnified by a lack of rewards.41 Rewards that acknowledge the accomplishments of HCWs can mitigate fatigue42 and provide motivation to deliver better patient care.43 Moreover, an unfair distribution of responsibilities was found to decrease job satisfaction and diminish the willingness to work hard.44 HCWs employed during the COVID-19 pandemic should be rewarded to reflect their personal sacrifices.
Our findings showed that various types of HCWs were assigned to new roles and required to make decisions that were beyond the scope of their previous duties. This burden of judgment made some HCWs feel powerless and guilty due to an inability to improve patient outcomes.45 Thus, skilled and well-trained colleagues and supervisors, together with new HCWs, should perform tasks in line with their professional responsibilities.
Our findings suggested that HCWs were susceptible to various health problems during the COVID-19 pandemic. Consistent with previous studies, the physical symptoms reported in this study included respiratory symptoms, myalgia, fatigue, and skin damage.446 Several risk factors for these physical problems were identified, including long work hours, unnecessary hand-washing, and improper infection control.7 Concerning skin damage, consistent with previous studies,4748 our findings showed that the increase in frequency of hand sanitation, and long periods in which personal protective equipment (PPE) were worn during the COVID-19 pandemic, damaged the skin on the hands of HCWs. PPE-induced dermatoses occur mainly because of occlusion and hyper-hydration of the skin by PPE due to epidermal barrier dysfunction,49 leading to the development of contact dermatitis. Coworkers and dermatologists should be aware of the potential for skin lesions in HCWs. Furthermore, emollients, creams, and moisturizers should be provided to HCWs as precautionary measures.49
This study had several limitations. First, since our work was qualitative and exploratory, causality was not established. Second, the sample was disparate, including physicians, service nurses, practitioners, and cleaners. However, we did not aim to compare experiences among different types of HCWs in COVID-19 wards. Third, self-reported measures (interviews) were used, which could have led to over-reporting of certain experiences. Despite these limitations, our multicenter, multidisciplinary study provides a useful record of HCW experiences during the COVID-19 pandemic.
In conclusion, our data indicate that HCWs experienced distress in their personal and professional lives due to working during the COVID-19 pandemic. Furthermore, all types of Korean HCWs had a heightened risk of mental and physical health problems after the pandemic, regardless of their workplace and region. The possible effects of these difficult experiences on HCWs should not be underestimated. Health care organizations should integrate HCWs support into their responses to the pandemic: comprehensive support systems to relieve negative health effects and improve the wellbeing of HCWs should be provided. In addition, long-term policies and strategies are needed to enable health care systems to better respond to long-lasting pandemic situations.
Go to :
 XML Download
XML Download