

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Preoperative risk prediction scoring systems have been used to measure perioperative risk and identify high-risk patients in cardiac surgery. Currently, there are several preoperative risk evaluation systems for predicting the surgical risk of coronary artery bypass grafting (CABG). The Society of Thoracic Surgeons (STS) risk model and European System for Cardiac Operative Risk Evaluation II (EuroSCORE II) are widely used scoring systems.123
Although these risk prediction systems have been well validated for predicting mortality and morbidity,13 these systems calculate the operative risk of CABG regardless of whether using cardiopulmonary bypass (CPB) machines or aortic manipulations are performed. However, currently, many studies have reported the benefits of anaortic off-pump coronary artery bypass grafting (OPCAB) in terms of postoperative stroke and mortality compared to conventional CABG.45 This study aimed to evaluate the performance of preexisting preoperative risk prediction scoring systems, such as the STS risk model and EuroSCORE II for patients undergoing anaortic OPCAB.
METHODS
Patient characteristics and surgical procedure
From January 2010 to June 2017, 1,140 patients had planned to undergo isolated OPCAB preoperatively. Among them, 83 patients with concomitant cardiac or noncardiac procedures and 9 patients with aortic manipulation were excluded, and a total of 1,048 patients were enrolled in this study (Fig. 1). One thousand forty-three patients underwent anaortic OPCAB, and 5 patients who planned to undergo anaortic OPCAB were converted to on-pump CABG because of hemodynamic instability during anastomosis. The preoperative characteristics of the present study group are summarized in Table 1.
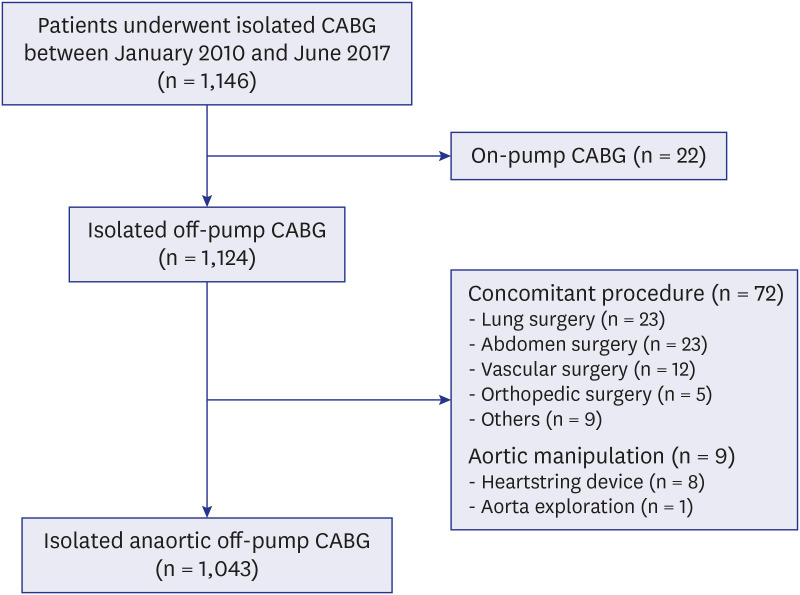
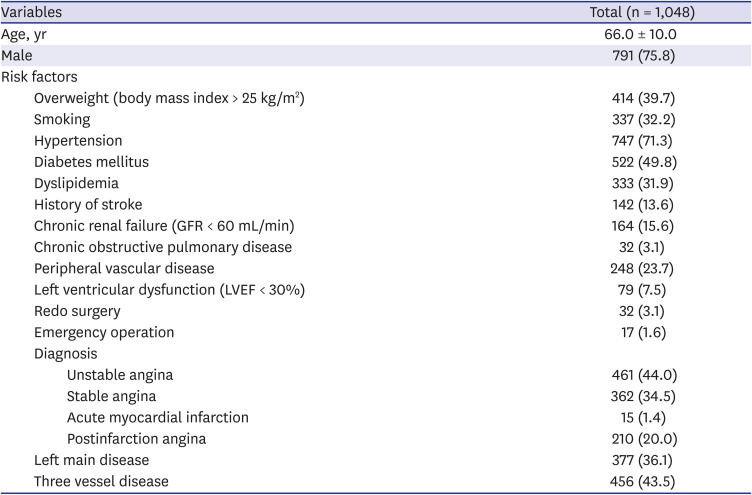
Table 1
Preoperative characteristics and risk factors of the study patients
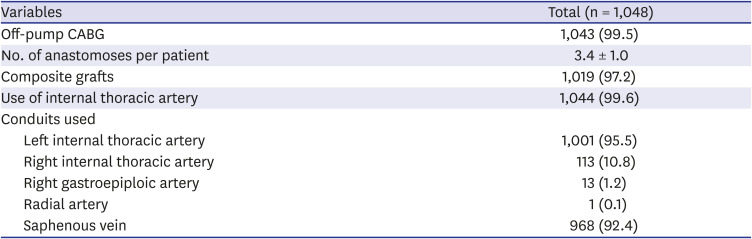
The basic surgical procedures and principles of OPCAB have been previously described.6 The internal thoracic artery (ITA) was used as an in situ graft to perform anaortic OPCAB in almost all of the patients (n = 1,044, 99.6%; left ITA, n = 1,001; and right ITA, n = 113), and the in situ right gastroepiploic artery was used in patients with single vessel disease of the right coronary artery (n = 2). composite graft technique was used for patients with multivessel disease (n = 1,014, 97.2%). The saphenous vein (SV) has been used as the preferred second conduit of choice to construct composite grafts since 2008 at our institution. The SV was harvested with a “minimal manipulation” technique before October 2013 and was harvested with a “no-touch” technique after October 2013. Transit-time flow measurement (TTFM; Medi-Stim AS, Oslo, Norway) and postoperative early angiographic evaluations were routinely performed. The operative characteristics of the present study group are summarized in Table 2.
Table 2
Operative and early clinical results
Calculation of the risk prediction scores
The EuroSCORE II was calculated for each patient with dedicated online software to predict operative mortality.7 The EuroSCORE II was calculated retrospectively before January 2016 and prospectively after January 2016. The STS score was calculated using dedicated online software for each patient to predict operative mortality and postoperative outcomes, including renal failure, permanent stroke, prolonged ventilation, deep sternal infection, reoperation, morbidity or mortality, short length of stay and long length of stay; these scores were calculated retrospectively because the STS score was recently revised to STS Adult Cardiac Surgery Database version 2.9 in 2018.8
All definitions of operative death and postoperative complications were followed by the STS risk model outcomes except for short and long length of stay.7 A short length of stay was defined as a hospital stay of less than 13 days, and a long length of stay was defined as a hospital stay of more than 16 days, referring to the data from Korea's Health Insurance review and assessment service. The performance of the STS risk model and EuroSCORE II were evaluated for calibration of 9 variables (mortality, renal failure, permanent stroke, prolonged ventilation, deep sternal wound infection, reoperation, morbidity or mortality, short length of stay, long length of stay) and calculation of discrimination power. Because STS risk model version 2.9 was developed for patients who underwent cardiac surgery between July 2011 and June 2014, subgroup analyses were performed for calibration of the STS risk model for patients who underwent CABG after July 2011 (n = 834).
Statistical analysis
Statistical analyses were performed using IBM SPSS statistical software (version 25.0, IBM Inc., Armonk, NY, USA) and SAS software (version 9.4, SAS Institute, Cary, NC, USA). The risk-adjusted event ratio was used to evaluate the calibration power of the STS risk model and EuroSCORE II. The risk-adjusted event ratio was defined as observed events divided by expected events (O/E ratio). An O/E ratio > 1.0 means that the model underpredicts the event, while an O/E ratio < 1.0 means that the model overpredicts the events. If the 95% confidence interval (CI) of the O/E ratio excludes the value of ‘1.0,’ it was considered statistically significant.9 The CI was calculated by the Byar approximation method. In addition to O/E ratio, the Hosmer-Lemeshow test and calibration plot were used to evaluate the calibration power of risk modes. The Hosmer-Lemeshow test was used to assess whether the observed event rate matched the expected event rate for the quartiles of the predicted value.10 The calibration was also assessed by plotting the predicted probability of operative mortality and postoperative complications against the actual probability with 95% CIs for the quartiles of the predicted value. The expected probability is shown on the x-axis, and the actual probability is shown on the y-axis.
The area under the ROC curve (AUC) was used to evaluate the discrimination power of the STS risk model and EuroSCORE II. The discriminative power is thought to be excellent when AUC ≥ 0.80, very good when 0.75 ≤ AUC < 0.8, and acceptable when 0.7 < AUC < 0.75. The DeLong's test was performed to compare the discrimination power for mortality between the EuroSCORE II and STS risk models.
Data are expressed as the mean ± standard deviation, or as proportions. A P value less than 0.05 was considered statistically significant, and 0.05 ≤ P value < 0.1 was considered marginally significant.
RESULTS
Performance of the EuroSCORE II
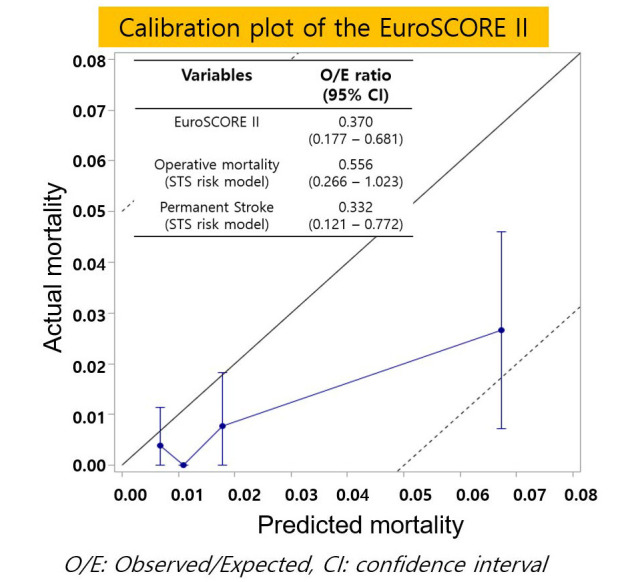
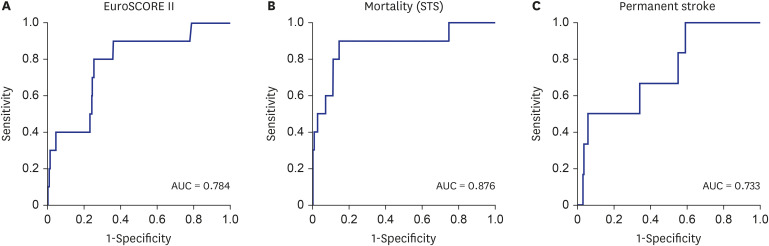
Operative mortality occurred in 10 patients (0.95%). The causes of operative mortality were septic shock (n = 4), low cardiac output syndrome (n = 3), acute respiratory distress syndrome (n = 2) and limb ischemia (n =1). The predicted mortality calculated from EuroSCORE II was 2.58 ± 4.15%. The O/E ratio of EuroSCORE II was 0.370, and EuroSCORE II significantly overpredicted the operative mortality for patients who underwent anaortic OPCAB (CI, 0.177–0.681; Table 3). In the Hosmer-Lemeshow test, there was a significant difference between the predicted mortality calculated by EuroSCORE II (P = 0.003) and actual mortality. The calibration plot showed that the predicted mortality calculated from EuroSCORE II was higher than the actual mortality in all groups (Fig. 2A). EuroSCORE II showed good discrimination power with an AUC of 0.784 (Fig. 3A).
Table 3
Calibration of the STS risk model and EuroSCORE II for all patients
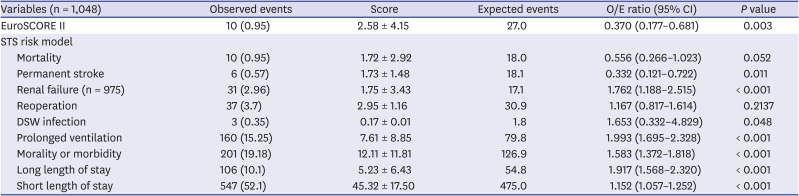
Fig. 2
Calibration plot of the (A) EuroSCORE II, (B) mortality calculated by the STS risk model and (C) permanent stroke calculated by the STS risk model.
EuroSCORE = European System for Cardiac Operative Risk Evaluation, STS = Society of Thoracic Surgeons.
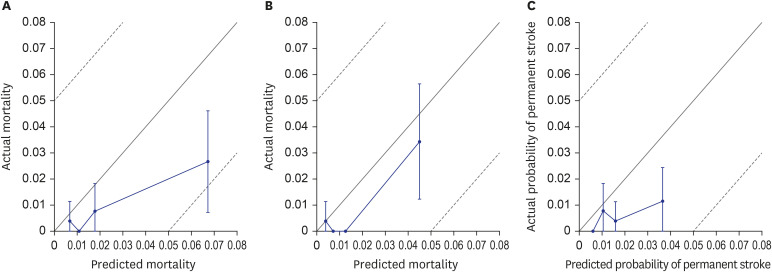
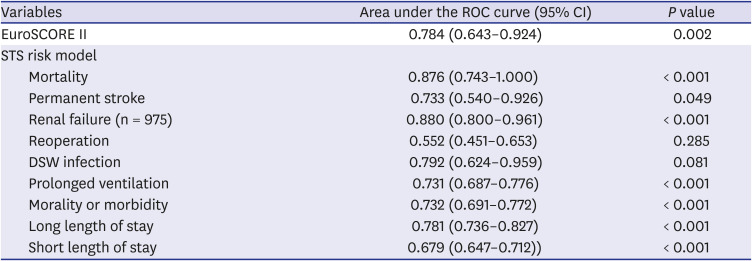
Fig. 3
ROC curves of (A) EuroSCORE II, (B) mortality and (C) permanent stroke calculated by the STS risk model.
ROC = receiver operating characteristic, EuroSCORE = European System for Cardiac Operative Risk Evaluation, STS = Society of Thoracic Surgeons, AUC = area under the receiver operating characteristic curve.
Performance of the STS risk model
The predicted mortality calculated from the STS risk model was 1.72 ± 2.92%. The O/E ratio of operative mortality in the STS risk model was 0.556, and the STS risk model overpredicted the operative mortality with margianlly significance in the Hosmer-Lemeshow test (CI, 0.266–1.023; P = 0.052; Table 3). The calibration plot showed that the predicted mortality calculated by the STS risk model was higher than the actual mortality in the top three quartiles (Fig. 2B). In terms of discrimination power for operative mortality, the STS risk model showed excellent results, with an AUC of 0.876 (Fig. 3B). The STS risk model showed a significantly higher discrimination power for mortliaty than the EuroSCORE II risk model (P = 0.007). In subgroup analyses for patients who underwent anaortic OPCAB after July 2011, the STS risk model overpredicted operative mortality with statisticaly significance based on the O/E ratio, and with marginially significance based on Hosmer-Lemeshow test (CI, 0.193–0.992; P = 0.055; Table 4).
Table 4
Calibration of the STS risk score for subgroups
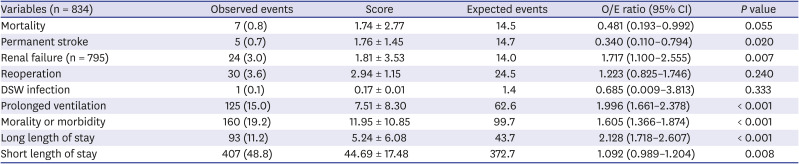
Permanent stroke occurred in 6 patients (0.57%), 5 of whom had embolic stroke, and one had a hemorrhagic stroke. No patients experienced atrial fibrillation before the stroke. The predicted permanent stroke occurrence rate calculated by the STS risk model was 1.73 ± 1.48%. The O/E ratio was 0.332, and the STS risk model significantly overpredicted the permanent stroke occurrence rate (CI, 0.121–0.722; Table 3). There was a significant difference between the predicted occurrence rate of stroke and the actual stroke occurrence rate in the Hosmer-Lemeshow test (P = 0.011). The calibration plot showed that the predicted probability of permanent stroke was higher than the actual probability in all groups (Fig. 2C). The discrimination power of the STS risk model for permanent stroke was acceptable, with an AUC of 0.733 (Fig. 3C). Subgroup analyses also showed that the STS risk model significantly overpredicted permanent stroke based on the O/E ratio and Hosmer-Lemeshow test (CI, 0.149–0.889; P = 0.020; Table 4).
The calibrations of other outcomes are summarized in Table 3. Based on the O/E ratio and Hosmer-Lemeshow test, the predicted occurrence rates of renal failure, prolonged ventilation, mortality or morbidity, long length of stay, and short length of stay calculated by the STS risk model significantly underpredicted the actual occurrence rate.
The discrimination power of the STS risk model for other outcomes are summarized in Table 5 and Supplementary Fig. 1. The STS risk model showed excellent discrimination power for renal failure and good discrimination power for deep sternal wound infection and long length of stay. Additionally, the STS risk model showed acceptable discrimination power for prolonged ventilation and mortality or morbidity. However, the STS risk model showed relatively low discrimination power for reoperation and short length of stay.
Table 5
Discrimination power of STS risk model and EuroSCORE II (n = 1,048)
DISCUSSION
This study reported two main findings. First, preexisting risk prediction scoring systems, the EuroSCORE II and the STS risk model, overpredict the mortality for patients undergoing anaortic OPCAB. Second, the STS risk model overpredicts the occurrence rate of permanent stroke for patients undergoing anaortic OPCAB.
Currently, the EuroSCORE II and STS risk models are widely used risk prediction scoring systems. EuroSCORE II predicts operative mortality after all cardiac surgeries, and the STS risk model predicts 9 early clinical outcomes, including mortality and permanent stroke, after six common cardiac procedures. These two systems showed good calibration and discrimination in the validation data.13 However, these risk prediction scoring systems have not been considered to calculate scores for aortic manipulation or used for CPB. Therefore, we evaluated whether the preexisting risk prediction scoring systems can appropriately predict the perioperative risk for patients undergoing anaortic OPCAB.
In this study, the EuroSCORE II and STS risk model (for subgroups) overpredicted the operative mortality for patients undergoing anaortic OPCAB. Although the advantage of OPCAB for mortality remains controversial,1112 our study showed the possibility that anaortic OPCAB has an advantage in terms of early mortality compared to conventional CABG. These results might be due to anaortic OPCAB being performed by a highly experienced surgeon, reduced occurrence of permanent stroke, and intrinsic features of not using CPB.
Although the EuroSCORE II and STS risk model overpredicted the operative mortality for patients undergoing anaortic OPCAB, the STS risk model (1.67%) calculated a predicted mortality that was closer to the actual mortality (0.95%) than the EuroSCORE II (2.51%). In addition, the STS risk model showed the better discrimination power for mortality. There are two possible factors that could affect this result. First, the two systems have different model designs. The STS score was developed using patients who only underwent isolated CABG, but the EuroSCORE II was developed using patients who underwent all kinds of cardiac surgery, and the operation type was considered a risk factor. The STS risk model calculated the predicted values based on 65 risk factors, but EuroSCORE II calculated the value based on 18 risk factors. Second, the latest STS risk model was developed for patients who underwent cardiac surgery between July 2011 and June 2014, and EuroSCORE II was developed for patients who underwent cardiac surgery in 2010. These differences may have allowed the STS risk model to calculate a more accurate prediction for operative mortality.
Anaortic OPCAB has theoretical benefits regarding the occurrence of stroke because this technique can prevent damage caused by CPB and aortic manipulation, such as emboli caused by gaseous or fat particles or atherosclerotic embolization.1314 Some previous studies showed a decrease in the risk of stroke after OPCAB,1516 and recently, a meta-analysis by Zhao and colleagues4 showed that anaortic OPCAB could decrease the risk for postoperative stroke, especially in high-risk patients. In this study, the STS risk model significantly overpredicted the occurrence rate of permanent stroke with an O/E ratio of 0.337. This result suggests that anaortic OPCAB could have a protective effect on permanent stroke compared to conventional CABG.
Although the present study suggested that anaortic OPCAB may have advantages in operative mortality and permanent stroke, previous studies demonstrated controversial results.111217181920 Comparable early results had been shown irrespective of applying cardiopulmonary bypass machine from previous large-scale multicenter studies.11121718 In addition, similar or favorable 5-year outcomes after on-pump CABG compared with off-pump CABG were recently reported from the CORONARY and ROOBY trial.1920 However, those previous studies have limitations regarding surgical expertise of attending surgeon,121718 and have not reported the extent of aortic manipulation and the proportion of an aortic OPCAB.11121718 In this regard, well designed randomized study comparing the conventional CABG and anaortic OPCAB should be performed.
Unexpectedly, the STS risk model underpredicted the occurrence rate of acute renal failure, prolonged ventilation, and mortality or morbidity. There are some possible explanations for these results. First, our institutional factor could affect the clinical results. Our postoperative protocols included performing early angiography for most of our patients, which might lead to a higher incidence of acute renal failure than the predicted value. Relatively long operation time might be taken as a teaching hospital and could lead a higher incidence of prolonged ventilation. Also, our postoperative strategy of extubation during the next daytime might also affect the prolongation of intubation. Second, the STS risk model for predicting prolonged ventilation is likely inaccurate for Asians. When the latest STS risk model was developed, only 2.8% of patients (12,076/439,092) were Asian people.3 The Asians included in the model development may not represent the Asians living in Asia since they lived in different lifestyles. Third, the intrinsic features of anaortic OPCAB including volume loading to stabilize the vital signs during posterior vessel revascularization might affect the clinical outcomes. Further studies should be performed to demonstrate the relation between the anaortic OPCAB and acute renal failure or prolonged ventilation.
In terms of hospital stay, the criteria to discriminate short and long stays were different from the definitions of the STS risk model because of the different health insurance systems between the USA and South Korea. The value of 16 days, which is the criterion for long stays, corresponded to the top 75%, and 13 days, which is the criterion for short stays corresponded to the bottom 25%. According to a previous study performed using STS NCD in 2002, 52.5% (260,908/496,797) of patients had a short stay, and 5.2% (26,008/496,797) of patients had a long stay.21 This means that our criteria using quartiles (bottom 25% and top 75%) for short and long stays may be too low. If the criteria were set similarly to the values of the previous study, the occurrence of short stays would increase, and the occurrence of long stays would decrease. The present study has several limitations. First, the present study was a retrospective observational study from a single institution and it had an institutional factor. And most of the surgeries were performed by a highly experienced surgeon for anaortic OPCAB. Therefore, this could limit the generalization of these results to all surgeons and hospitals. A multicenter study involving many surgeons performing both on-pump and off-pump CABG will be required to evaluate the performance of the preexisting risk models for anaortic OPCAB.
Second, the number of events was too small to evaluate the calibration of the models, especially for deep sternal wound infection, using the Hosmer-Lemeshow test. Therefore, the risk-adjusted ratio was mainly used for the calibration of the models, and there were some differences between the risk-adjusted ratios and Hosmer-Lemeshow tests.
In conclusion, the preexisting risk prediction scoring systems for CABG, the STS risk model and EuroSCORE II, overpredicted the risk of mortality and stroke rate for anaortic OPCAB. These findings suggest the possibility that anaortic OPCAB can lower the operative mortality and occurrence of postoperative stroke than conventional CABG.
 XML Download
XML Download