

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
After several pneumonia patients were reported to be positive for the severe acute respiratory syndrome coronavirus 2 in December 2019, it rapidly spread all over the world. Until now, more than 120 million patients have been confirmed to have contracted the coronavirus disease 2019 (COVID-19), and approximately 3.0 million patients have succumbed to this disease.1 This novel coronavirus is different from other members of the Coronaviridae family. The virus responsible for COVID-19 could show high viral load without symptoms in the disease's early phase.23 Therefore, control of the disease is very difficult due to its clinical characteristics. Several studies have reported that COVID-19 infection could induce symptoms associated with upper and lower respiratory infection such as cough, rhinorrhea, sputum, and dyspnea and general symptoms of fever and fatigue. Moreover, it has also been reported to cause mild to severe acute respiratory distress syndrome and even death has been reported.45 Although olfactory dysfunction (OD) was not considered an important symptom in the early days of the COVID-19 outbreak, recently published studies have suggested that OD must be considered an important symptom in the early stages of COVID-19 disease. Borsetto et al.6 reported that the overall prevalence of OD was 47%, as reflected from the findings of a systematic review of patients which mentioned about OD. This symptom preceded other symptoms in 20% of patients and was a concomitant manifestation in 28% of patients.6 Also, the American Academy of Otolaryngology-Head and Neck surgery included OD as a screening tool for the detection of COVID-19 infection.7 We also recently published an article about OD, which was evaluated as an objective test (Cross-Cultural Smell Identification Test [CC-SIT]; Sensonics International, Haddon Heights, NJ, USA) in COVID-19 patients who were isolated in a quarantine facility (Gyeonggi International Living and Treatment Support Center). We observed that 24.2% of patients complained of OD with a mean CC-SIT score of 8 ± 2.8
Several studies have reported on the pattern of recovery of OD which showed considerable variability. Chiesa-Estomba et al.9 reported that among the 751 patients, 367 (49%) patients reported complete recovery, and 107 (14%) patients reported partial recovery of olfaction after a mean follow-up of 47 ± 7 days. Additionally, Chary et al.10 reported that 64% of patients reported complete recovery and 33% reported incomplete recovery. To date, no treatment has been clearly established for OD associated with COVID-19 infection. Olfactory training is a validated treatment modality in patients with OD, as suggested by Hummel et al.11 Moreover, Damm et al.12 reported that olfactory training is a successful therapy regimen in patients with post-infectious OD (PIOD). PIOD occasionally occurs after upper airway viral infection, in which olfactory impairment persists even after the resolution of other respiratory symptoms. In our previous report, COVID-19 infection-associated OD was regarded as a quantitative disorder (reduced or absence of olfaction) with sensory neural cause, such as PIOD.8 Therefore, we consider that olfactory training is also effective in COVID-19 associated OD.
To assess the clinical characteristics of OD in COVID-19 patients, we compared the subjective and objective olfactory function using questionnaires and CC-SIT as per the experience of the patients during COVID-19 infection. Moreover, we assessed the effect of olfactory training in patients with OD who were confirmed by CC-SIT objectively.
METHODS
Study design, study population, and data collection
This prospective cohort study included 53 adult patients who were diagnosed with COVID-19 by reverse transcriptase-polymerase chain reaction from respiratory samples. The diagnosis was confirmed, and the recovery period was between April 2020 and September 2020. Patients who had experienced OD before confirmation of COVID-19 diagnosis were excluded from the present study. Nasal endoscopic examination and olfactory evaluation were performed by a single rhinologist at our tertiary hospital's outpatient clinic. When the patients visited the clinic, we interviewed the participants about general and rhinological symptoms, and history of underlying disease. The study participants were asked to fill out questionnaires about their current state of olfactory function. Thereafter, we performed an objective olfactory function test using CC-SIT.12 If the CC-SIT score indicated that the participant had OD, we recommended the olfactory training for two months and performed the follow-up test to evaluate olfactory function improvement. All study participants did not take any oral or topical steroids before and during study periods.
Evaluation of subjective and objective olfactory function
Subjective olfactory function was evaluated using the 11-point Likert scale (0–10), and the Korean version of the Questionnaire of Olfactory Disorders (QOD).14 Among QOD questionnaire subdomains, we used the QOD-visual analog scale (QOD-VAS) and the short version of QOD-negative statements (sQOD-NS). The Korean version of the QOD-VAS comprises five questions with an 11-point scale (0–10), and a higher score indicates poor subjective olfactory function. On the other hand, the Korean version of sQOD-NS consists of seven questions with a 4-point scale (0–3) and a higher score indicates better subjective olfactory function. The CC-SIT comprises 12 multicultural odorants items (banana, chocolate, cinnamon, gasoline, lemon, onion, paint thinner, pineapple, rose, soap, smoke, and turpentine) based on items from the University of Pennsylvania Smell Identification Test.13 The patients underwent the “scratch-and-sniff” protocol that involved 12 microencapsulated odorants strips with enveloped pencil and forced-choice of one answer among the four choices. Although, Doty et al.13 suggested normative data according to age and sex, we used our country criteria according to previously published data, anosmia as 0–4, hyposmia as 5–10 and normosmia as 11–12.1415
Olfactory training using odorants
Olfactory training is a treatment for patients with OD that was first suggested by Hummel et al.11 using eucalyptus, clove, lemon, and rose. In Korea, Kim et al.16 suggested the four familiar odorant regimens as pine, cinnamon, lemon, and peppermint. They reported successful results on olfactory function improvement in PIOD patients using these odorants. Thus, we also used the same regimen. The patients had to sniff each odorant for 10 seconds with a rest period 30 seconds to prevent olfactory fatigue twice a day (morning and evening) for 2 months.16
Statistical analysis
Statistical analysis was performed using the Statistical Package for the Social Science version 21 (IBM Corporation, Armonk, NY, USA). To compare the participant's demographics, the subjective and objective olfactory function between patients' group according to the experience of olfactory impairment, categorical variables were compared using the χ2 test and continuous variables were compared using the Mann-Whitney U test. We also performed an independent t-test and Fisher's exact test to assess the subjective and objective olfactory function changes after olfactory training.
RESULTS
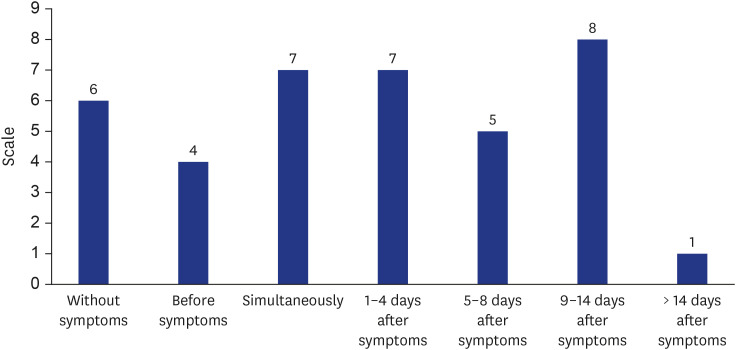
Among the 53 study subjects, 35 were female. A total of 38 subjects reported the experience of OD during COVID-19 infected periods. The mean ± standard deviation age of the study participants was 36.51 ± 13.59 years. The mean number of days after diagnosis of COVID-19 was 89.06 ± 40.89 days, and in the 38 subjects who experienced OD, the mean follow-up period after the initiation of OD was 88.50 ± 39.44 days. The demographics of the study participants are described in Table 1. When we assessed the timeline for the manifestation of general or rhinologic symptoms to the onset of OD, six patients developed OD without other general or rhinologic symptoms. Besides, four patients developed OD before the onset of other symptoms, while seven patients developed OD simultaneously. Also, 21 patients developed OD after development of other symptoms (Fig. 1).
Table 1
Demographics of study subjects
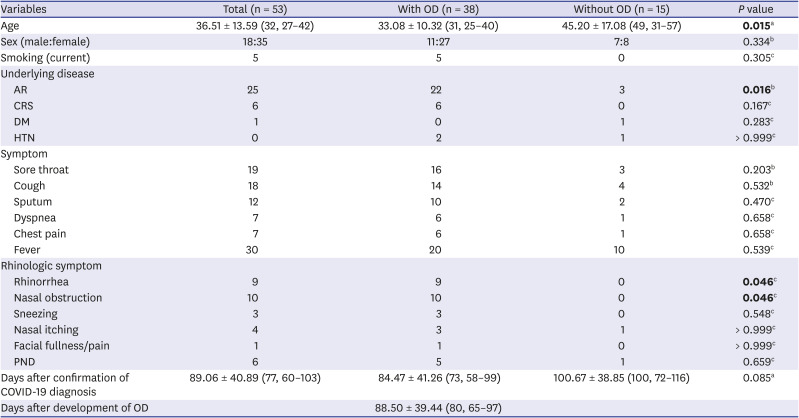
Values are presented as mean ± standard deviation or median (interquartile range).
Bold values indicate statistically significant.
OD = olfactory dysfunction, AR = allergic rhinitis, CRS = chronic rhinosinusitis, DM = diabetes mellitus, HTN = hypertension, PND = post nasal drip, COVID-19 = coronavirus disease 2019.
aMann-Whitney U test; bχ2 test; cFisher's exact test.
Subjective and objective olfactory function
As mentioned above, 38 subjects reported that they experienced subjective OD (with OD group), and 15 subjects did not (without OD group). Among the 38 subjects in the OD group, 92.1% (35/38) patients stated that their olfactory function improved, and 52.6% (20/38) patients were regarded as normosmia according to the CC-SIT score. When we compared the olfactory function status between these two groups, we found that the subjective olfactory function was significantly impaired in the with OD group even after three months of OD onset. Moreover, the number of patients with subjective hyposmia was also significantly higher in the with OD group than in another group. However, according to CC-SIT score and the number of patients with objective hyposmia (CC-SIT ≤ 10), the objective olfactory function was not significantly different between the two groups (Table 2). Additionally, we also found that six patients were diagnosed as hyposmic status objectively even though they had not experienced any OD.
Table 2
Comparison of subjective and objective olfactory function between patients group with and without OD after COVID-19 diagnosis
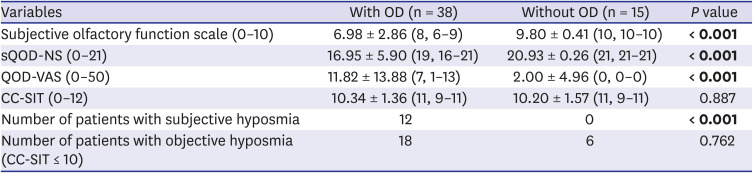
Values are presented as mean ± standard deviation or median (interquartile range).
Bold values indicate statistically significant.
Mann-Whitney U test and χ2 test.
OD = olfactory dysfunction, COVID-19 = coronavirus disease 2019, sQOD-NS = short version of Questionnaire of Olfactory Disorders-negative statements, QOD-VAS = Questionnaire of Olfactory Disorders-visual analog scale, CC-SIT = Cross-Cultural Smell Identification Test.
Effects of olfactory training
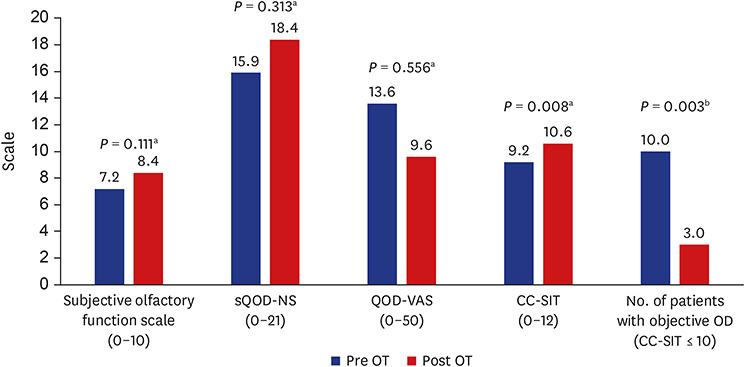
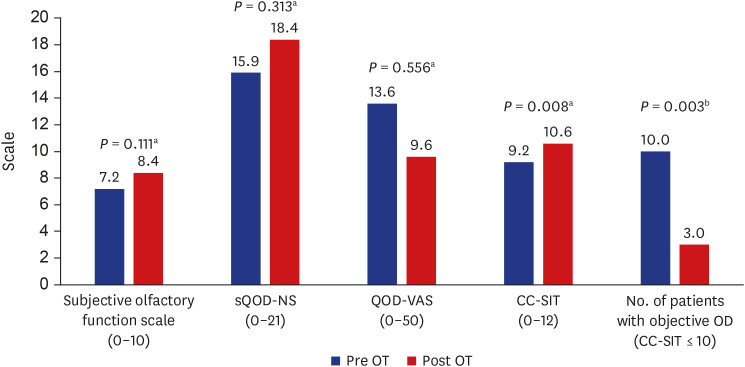
Olfactory training was introduced among 24 patients. However, only 10 patients revisited the outpatient clinic after the 2-months duration of olfactory training. Therefore, we could perform the assessment only in these 10 patients. In our study subjects with olfactory training, seven out of 10 patients recovered to normal olfactory function. The mean CC-SIT score was significantly increased after 2 months of olfactory training (9.20 ± 0.79 to 10.60 ± 1.26, P = 0.008). However, subjective olfactory function according to the 11-point Likert scale, sQOD-NS, QOD-VAS only showed an improved tendency without statistical significance after 2 months of olfactory training (Fig. 2).
Fig. 2
Changes of subjective and objective olfactory function after 2 months of olfactory training.
sQOD-NS = short version of Questionnaire of Olfactory Disorders-negative statements, QOD-VAS = Questionnaire of Olfactory Disorders-visual analog scale, CC-SIT = Cross-Cultural Smell Identification Test, OD = olfactory dysfunction, OT = olfactory training.
aIndependent t-test; bFisher's exact test.
DISCUSSION
In the present study, we found that subjective olfactory function was significantly impaired in patients who experienced olfactory impairment during COVID-19 infection even after 3 months of symptom onset. However, an objectively measured olfactory function was not significantly different in the presence or absence of a history of OD in the context of COVID-19 infection. To date, several studies have evaluated the clinical features and pathophysiology of COVID-19 infection-associated OD. Mastrangelo et al.17 reported that COVID-19 infection-associated OD occurred without nasal congestion or discharge. These clinical features suggest that OD might be caused by sensorineural damage. Moreover, they suggested that phagocytes infection and vascular damage in olfactory bulb, and infection and death of supporting cells due to COVID-19 lead to inflammatory cytokine release and causes neuronal dysfunction.17 Lv et al.18 performed the telephone survey in 196 patients and reported that impaired olfaction in the COVID-19 patients was restored in 89.7% of the patients within 3 months of their discharge from hospital. Brandão Neto et al.19 also performed a telephone survey using 11-point category rating scale in 655 patients who recovered from COVID-19 infection. This study also reported that the total and partial olfaction recovery rate was 53.8% and 44.7%, respectively.19 Besides, Cho et al.7 performed the prospective cohort study in 83 COVID-19 patients and 60 controls using the 11-point Likert scale to evaluate of olfactory function. They reported a complete recovery of olfaction in 71.8% of COVID-19 patients within 10 days of symptom onset.7 Moreover, Kosugi et al.20 and Chary et al.10 also reported the short-term recovery rate of olfaction as 86.8% and 97% using subjective questionnaires. In our study subjects, about 92.1% (35/38) of patients reported that their olfaction improved, and 68.4% (26/38) reported that their olfaction totally recovered based on subjective evaluation. These results were similar to the above mentioned earlier studies. However, we found that objective olfaction using validated CC-SIT was normalized in only about 52.6% (20/38) of the patients with OD group. Also, six of the patients who stated that they had no experience of OD were identified as hyposmic state. Considering the reasons for the inconsistency between subjective and objective olfactory outcomes, we presumed that if patients experienced OD, they would be extremely concerned about OD and constantly worried about it. Therefore, the patients with OD group showed negative results for the sQOD-NS and QOD-VAS questionnaires than patients without OD group. Based on these results we suggest that, although subjective olfaction is important, there might be an error when the improvement in olfactory function is gauged by using only subjective parameters.
Recently, Le Bon et al.21 reported the clinical outcome of olfactory training in 18 dysosmic patients after COVID-19 infection. They reported that a 10-week course of olfactory training had improved their olfactory function score.21 In our study, we found that the subjective olfactory function showed an improved tendency after olfactory training without any statistical significance. Furthermore, the objective olfactory function was significantly improved, and 70% of patients were normalized after olfactory training. In the present study, the mean duration of olfactory impairment in patients who underwent olfactory training was approximately 3 months. Kim et al.22 reported that better treatment outcomes were achieved in PIOD patients who started olfactory training less than 1 month after olfactory loss. Therefore, we concluded that immediate olfactory training might show better results in COVID-19 infection-associated OD.
Our study has several limitations. First, we performed CC-SIT to confirm objective olfactory function. Although CC-SIT is a validated study, it can only evaluate the identification of olfactory function. Therefore, the patients with subjective OD might have decreased threshold or discrimination of olfactory function, and these aspects could affect the results of this study. The most validated objective olfactory function test is to assess the threshold, discrimination and identification (TDI) of olfaction. Moreover, CC-SIT consists of only 12 questions. So, it is difficult to distinguish between malingering and anosmia because the expected minimum score for random answers is 3 and the criteria for anosmia is 4. Therefore, if we evaluated the objective olfaction using TDI score, we could suggest more valuable data than the present study. However, when we initiated this study, the Food and Drug Administration of South Korea withdrew the olfactory test's approval using TDI. Thus, it was impossible to use it for objective evaluation of olfactory function. Also, Konstantinidis et al.23 reported that olfactory function mainly increased olfactory identification score with olfactory training in PIOD patients. Therefore, we regarded that olfactory improvement using only identification tests could also show meaningful clinical results. Second, only 41.7% (10/24) of patients with olfactory training visited our outpatient clinic to assess olfactory improvement, and the number of study subjects was relatively small. Thus, it might have caused selection bias. Third, in our demographics of study subjects, initial nasal symptom and history of nasal disease was significantly different between with OD and without OD group. Therefore, it might have affected the results of this study. Lastly, we did not perform a randomized controlled study to assess the effect of olfactory training. Therefore, we thought that well-designed study with a sufficient sample size is required, and we plan to conduct such a follow-up study in the future.
In the present study, we found that subjective olfactory function significantly decreased in COVID-19 patients who had experienced OD within 3 months of the disease course. However, the objective olfactory function was not significantly different in COVID-19 patients, even when these patients had an OD history. Therefore, olfactory function assessment using subjective questionnaires only might not reflect the real status of olfactory function in COVID-19 patients.
The two-month duration of olfactory training significantly improved olfactory function, and 70% of patients became normal after treatment. Therefore, olfactory training is an effective treatment modality for COVID-19 infection-associated OD.
 XML Download
XML Download