

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
It is now more than one year since the first case of the coronavirus disease 2019 (COVID-19) was reported in the Republic of Korea, and as of February 1, 2021, there were 85,567 confirmed COVID-19 cases. Among the cases, 9,063 cases (10%) are children below 19 years,1 and no child fatality has been reported so far. This is similar to a global trend; many clinical studies have reported a low risk of infection and mild COVID-19 symptoms in children as compared to adults. According to a clinical analysis of 2,135 COVID-19 pediatric patients reported to the Chinese Center for Disease Control and Prevention (CDC), most children infected with the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from January 16 to February 8 in China showed mild or no symptoms. Of the 728 confirmed COVID-19 pediatric patients, 408 had mild or no symptoms, 298 cases were moderate, and only 18 cases were severe.2 In addition, in another study that included 31 COVID-19 pediatric patients in China, 17 cases were asymptomatic or mild, and 14 children had symptoms of pneumonia. There were no severe cases, and their symptoms usually improved within 3 days.3 Together, these findings indicate that children's clinical manifestations of SARS-CoV-2 may be less severe than that of adults.
A study by the CDC in the United States on SARS-CoV-2 in children reported that, as of April 2, 2020, out of 149,082 COVID-19 patients, 2,572 (22%) were children (< 18 years). Of the confirmed cases, 147 were hospitalized and only 15 children were admitted to the intensive care unit (ICU). Most cases of hospitalization were children < 1 year or with underlying diseases. 75% of the children had symptoms such as fever, cough, and shortness of breath, but they reported mild clinical manifestation.4
A study in Korea reported milder illness in children infected with SARS-CoV-2. The study included 91 COVID-19 confirmed pediatric patients aged under 19 years in Korea from February 18 to March 31, 2020. 30% of the patients had a mild fever and 39% of the patients had a high fever (38°C or higher). More than 60% of the patients had respiratory symptoms, and there were cases of anosmia and ageusia. Some patients had abdominal pain and diarrhea. In general, of the 91 patients, 65 tested positive for an RT-PCR test, among the 85% had mild symptoms, and no case developed to a severity level that required intensive care. This study showed that pediatric infections are less symptomatic and severe with a possibility of living a normal life unaware of SARS-CoV-2 infection.5
Based on the reports of low prevalence and severity of pediatric SARS-CoV-2 infections, the government has released new SARS-CoV-2 infection response and treatment guidelines for children. Following these guidelines, pediatric patients with no or mild symptoms can be treated at home under the care of their parents.6 This measure is meant to provide psychological stability along with treatment. In addition, some studies demonstrated that schools are not high-risk infection environments78 and that transmission to children was mostly household, with a low percentage of school transmissions (2.4%).9 Together, these findings could have inspired the Korean government to direct school reopening under strict infection prevention guidelines.10 However, there is still considerable concern on the impact of school reopening on community transmission of SARS-CoV-2.
In the present study, we aimed to evaluate the appropriateness of these directives and the severity of SARS-CoV-2 infections in children as compared to adults using sufficient national sample data. Therefore, we analyzed the impact of SARS-CoV-2 infection on children using SARS-CoV-2 national data, with the length of hospital stay (LOS), medical expenses, and ICU hospitalization as the variable outcomes. In addition, we aimed to provide informed suggestions on an efficient management plan for pediatric patients.
Go to : 
METHODS
Data collection and study participants
The purpose of this study was to determine the severity of SARS-CoV-2 infection in the pediatric population as compared to adults and to evaluate the appropriateness of the recent government directives, by analyzing the length of hospitalization, medical expenses, hospital, and intensive care unit admission rates. For this analysis, we used the NHIS-COVID DB of the National Health Insurance Service (NHIS). NHIS provides the NHIS-COVID DB to support research studies which are based on the evidence for the treatment and policy implementation of Coronavirus patients. This national data includes national qualifications, insurance premiums, medical exam results, and medical records from January 2015 to July 2020.11 In this study, we analyzed the records of 7,969 COVID-19 patients who were confirmed between January 01, 2020 and May 30, 2020 (Fig. 1). The length of hospitalization (number of days), medical expenses, hospitalization, and ICU admission rates were calculated. Medical expenses were calculated by converting KRW to USD based on the exchange rate on May 30, 2020.
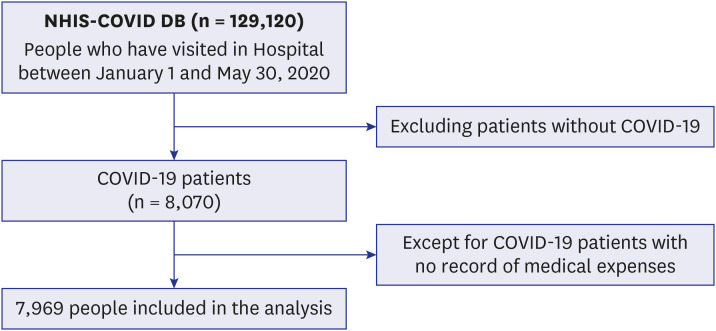 | Fig. 1Flow chart for people inclusion and exclusion criteria, and the final sample size.We have had NHIS-COVID DB for 129,120 patients who were enrolled in the National health insurance service and have been treated in Hospital between January 1 and May 30, 2020. Among them, 8,070 were COVID-19 patients, and we selected finally 7,969 COVID-19 patients except for those with no record of medical expenses.
COVID-19 = coronavirus disease 2019.
|
Statistical analysis
A t-test and ANOVA test were performed for a basic analysis of the difference in length of hospitalization days and medical expenses according to the characteristics of COVID-19 patients, and a chi-square test was used to compare the difference between hospitalization, intensive care unit admission rates, and characteristics of COVID-19 patients.
The following COVID-19 patient characteristics were considered; gender, age (0–9, 10–19, 20–29, 30–39, 40–49, 50–59, 60–69, 70–79, 80+), residence, health insurance premium, CCI score, and death. Health Insurance premium was used as a variable to reflect the economic status of the COVID-19 patients; in Korea, health insurance premiums are paid in accordance with income level. Medical aid is a low-income class, in which members do not pay health insurance premiums. In the present study, health insurance subscribers were classified into 1st quantile (lowest), 2nd quantile, 3rd quantile, 4th quantile, and 5th quantile (highest) according to the level of insurance premium. The CCI score was used to determine the severity of the underlying diseases. The updated weights suggested by Quan were assigned to calculate CCI Score.12 The length of hospital admission due to SARS-CoV-2 infection only, and hospital and ICU admission rates were used to determine the severity of COVID-19.
A multivariate linear regression analysis was carried out to examine the impact of COVID patients' characteristics on the LOS and medical expenses. The independent variables used in the linear regression model were gender, age, residence, health insurance premiums, and CCI scores, and the LOS and medical expenses were input into the model as dependent variables after log-transformation. Age groups were categorized as 0–9, 10–19, 20–49, 50–69, and 70+. As a result of Kolmogorov-Smirnov test, the LOS and medical expenses did not satisfy the normal distribution (P < 0.001). Thus, they were converted by taking the natural log. Multivariate logistic regression analysis was performed to identify the characteristics that affect the hospital and ICU admission rates of COVID-19 patients and to prove the low severity of SARS-CoV-2 infection in pediatric patients. Age (0–9, 10–19, 20–49, 50–69, 70+), residence, health insurance premiums, and CCI scores were set as independent variables and the dependent variables were hospital and ICU admission rates. SAS 9.4 was used for all statistical analysis and statistical significance was verified on the basis of P value < 0.05.
Ethics statement
This study conformed to the Korean guidelines on De-identification of Personal Data and was approved by the Kyung Hee University's Institutional Review Board (IRB No. KHSIRB-20-301(EA)) as a review exemption study. As the study used de-identified data, informed consent was waived by the board.
Go to :
RESULTS
COVID-19 patient characteristics
To compare the average LOS and medical expenses with the COVID-19 patients' characteristics, and to confirm the statistical significance, t-test, and analysis of variance (ANOVA test) were performed (Table 1). Based on our results, the LOS for female patients (27.4 ± 19.3 days) was longer than that of male patients (26.7 ± 19.1 days), and there was a statistically significant difference between means (P = 0.006). In addition, medical expenses were higher among women (6,043 ± 9,761 USD) than in men (5,201 ± 6,043 USD) (P < 0.001). An analysis of the LOS (P < 0.001) and medical expenses (P < 0.001) by age, which are the main results of this study, showed that mean of LOS was the shortest in patients aged 10–19 (22.4 ± 12.9 days), and the longest in patients aged 80 years and above (34.2 ± 25.7 days). The medical expenses for patients aged 0–9 (4,640 ± 7,086 USD) and 10–19 (4,232 ± 3,689 USD) years were lower than for the other age groups and it increased with age in patients over ≥ 20 years. Among the areas of residence, Seoul had the longest LOS (43.7 ± 34.6 days) and highest medical expenses (10,580 ± 12,238 USD), which were significantly different from those of the other areas (P < 0.001). There was a difference between the average of LOS and medical expenses by health insurance premium level (P < 0.001), and the LOS was the longest among the patients in the 1st quartile (30.6 ± 25.1 days), while the medical expenses were the highest among patients with medical benefits (7,754 ± 8,656 USD). The patients who had a CCI score of 3+ showed the longest LOS (33.8 ± 27.2 days) and highest medical expenses (7,123 ± 9,391 USD) (P < 0.001). There was no significant difference in LOS according to the death of COVID-19 patients (P = 0.483), but there was a difference in medical expenses (P < 0.001). The average medical expense for the death cases was 4,930 ± 7,374 USD, which was higher than that of the survivors (6,441 ± 8,911 USD).
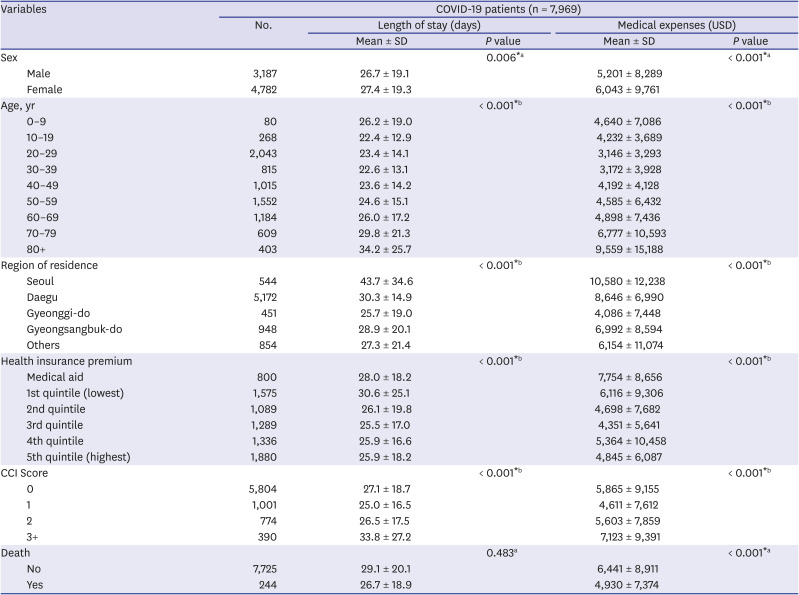
Table 1
Mean length of stay and medical expenses by characteristics of COVID-19 patients
COVID-19 = coronavirus disease 2019, SD = standard deviation, CCI = Charlson comorbidity index.
*P < 0.05, aP value for t-test, bP value for ANOVA test.
![]()
A Chi-square test was performed to compare the rates of hospital and ICU admissions with the characteristics of the COVID-19 patients and to determine statistical significance (Table 2). 79.1% of the patients were hospitalized and approximately 12.8% of patients were admitted to the ICU (P < 0.001). Hospitalization rates and intensive care unit rates were higher in male patients 82.6% and 16.1%, respectively, than in female patients. In the hospitalization and ICU admission by age, the higher the age, the higher the hospitalization rate. However, while the hospital admission rates for patients aged 0–9 years (90.0%) were higher than patients aged 60–69 years (87.2%), the ICU rates for patients aged 0–9 years (12.5%) were similar to ICU rates in patients aged 50–59 (12.6%). The hospital admission rate of COVID-19 patients was highest in Seoul (98.3%), while the ICU admission rate was higher in the other areas (29.2%). Hospital admission rates by health insurance premium level were the highest for patients with medical benefits (84.9%), and these rates increased as the health insurance premium level increased. The ICU admission rates showed a similar trend to hospital admission rates. The higher the CCI score, the higher the hospital and ICU admission rates, and the hospital (99.6%) and ICU (48.8%) admission rates of the patients dying from COVID-19 were higher than those of the survivors (P < 0.001).
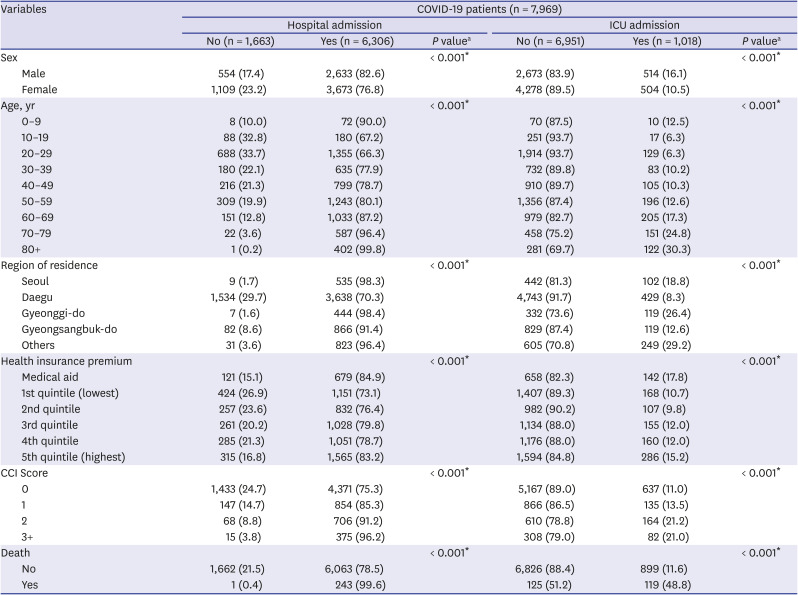
Table 2
Rate of hospital and ICU admission by characteristics of COVID-19 patients
ICU = intensive care unit, COVID-19 = coronavirus disease 2019, OR = odds ratio, CI = confidence interval, CCI = Charlson comorbidity index.
*P < 0.05, aP value for χ2 test.
![]()
Linear regression analysis for the length of stay and medical expenses in COVID-19 patients
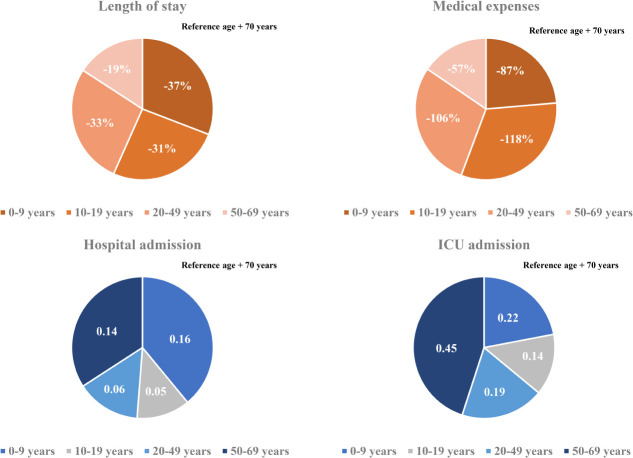
Multivariate linear regression analysis was employed to analyze the relationship between LOS of COVID-19 patients, medical expenses, and social factors (Table 3). To satisfy the linearity of the regression model, a regression model was established by log conversion of the number of LOS and medical expenses. Based on the analysis results, there was a correlation between all the other variables except for health insurance premiums and the LOS, and all independent variables in the case of medical expenses. The LOS of female patients was 4% shorter than that of male patients (P = 0.004), and medical expenses were 18% lower in female patients than male (P < 0.001). With regard to LOS and medical expenses by age, the LOS for patients aged 0–9 was the shortest, and the medical expenses for patients aged 10–19 were the lowest. Compared to patients over 70 years old, patients aged 0–9 had a 37% shorter LOS (P < 0.001) and spent 87% less on medical expenses (P < 0.001). The LOS for patients aged 10–19 was 31% shorter (P < 0.001), and they had lower medical expenses (118%).
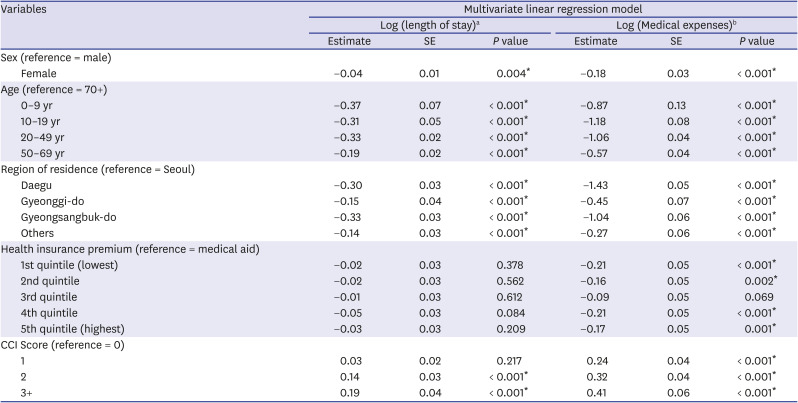
Table 3
Results of the multivariate linear regression analysis for log of “length of stay” and “medical expenses”
SE = standard error, CCI = Charlson comorbidity index.
*P < 0.05, aMultivariate linear regression model with a natural log of “length of stay” as dependent variable; bMultivariate linear regression model with a natural log of “medical expenses” as dependent variable.
![]()
Based on the analysis of the LOS and medical expenses by residential areas, the LOS and medical expenses in other regions were lower than in Seoul. In particular, in Gyeongsangbuk-do, LOS was the shortest, while the medical expenses for Daegu were 143% lower than that of Seoul, as well as the other regions (P < 0.001). It was found that health insurance patients had longer LOS than medical aid patients, showing a statistically significant difference. Medical aid patients were charged more for medical expenses than health insurance patients. Statistical difference was confirmed in these groups except the 3rd quintile group.
As for the CCI score, as the score increased, the length of hospitalization and medical expenses increased. Patients with a CCI score of 3 or higher had 19% longer LOS than patients with a CCI Score of zero (P < 0.001). There was a statistical difference between medical expenses and CCI Score, and patients with a CCI score of 3 + spent 41% more on medical expenses than patients without severe underlying diseases (P < 0.001).
Logistic regression analysis for hospital and ICU admission in COVID-19 patients
Multivariate logistic regression analysis was performed to evaluate the impact of social factors on the severity of COVID-19 patients (Table 4). Two logistic regression models were created with hospital and ICU admission as outcome variables, and the analysis showed the association between hospital or ICU admission and the most independent variables in the logistic regression model. First of all, the risk of hospitalization (odds ratio [OR], 0.74; 95% confidence interval [CI], 0.65–0.84) and ICU admission (OR, 0.62; 95% CI, 0.54–0.72) in female patients was lower than in male patients. Younger age groups were at a lower risk of hospitalization and ICU admission than patients over 70 years of age. The odds ratio for hospital admission for patients aged 10–19 years was 0.05 times and for admission to the ICU was 0.14 times lower compared to patients aged 70 years and over. Patients aged 10–19 showed the lowest severity. By region, the risk of hospitalization was the highest in Seoul, while the ICU admission rate was higher in patients who resided in Gyeonggi-do (OR, 1.40; 95% CI, 1.02–1.91) and other regions (OR, 1.71; 95% CI, 1.30–2.25). Analysis of the health insurance premium level of COVID-19 patients showed that hospital and ICU admission was higher in patients with medical benefits. The higher the CCI score, the higher the risk of hospital admission, and it was statistically significant. However, statistical significance was only observed in patients with a CCI score of 2 (OR, 1.50; 95% CI, 1.21–1.86) when admitted to the ICU. Analysis of risk factors affecting admission to the intensive care unit was only done on the younger age group (0–19 years). A logistic regression model was established by considering gender, age, residential area, Health insurance premium quintile, and disability as explanatory variables, of which no variables were statistically significant (Table 5).
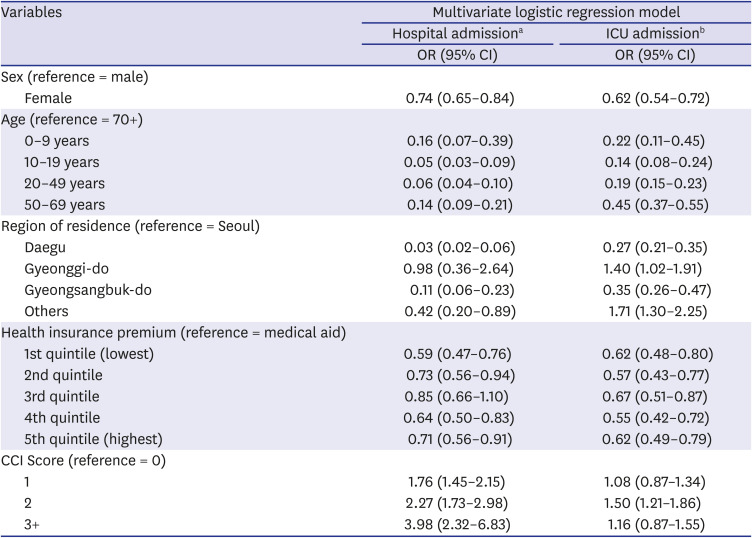
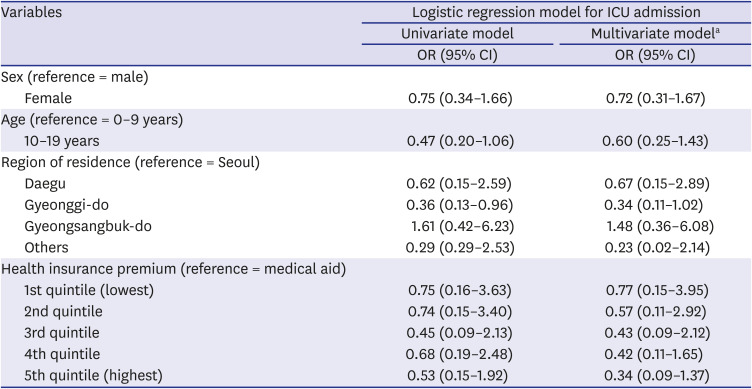
Table 4
Results of the multivariate logistic regression analysis for hospital and ICU admission
ICU = intensive care unit, OR = odds ratio, CI = confidence interval, CCI = Charlson comorbidity index.
aMultivariate logistic regression model with “hospital admission” as a dependent variable; bMultivariate logistic regression model with “intensive care unit admission” as a dependent variable.
![]()
Table 5
Results for the multivariate logistic regression analysis for ICU admission in aged 0–19 years
aMultivariate logistic regression model with “intensive care unit admission” as a dependent variable. Disability was also corrected as an explanatory variable in this model.
ICU = intensive care unit, OR = odds ratio, CI = confidence interval.
![]()
Go to :
DISCUSSION
In this study, we included 7,969 Korean COVID-19 patients between January 1, 2020 and May 30, 2020. We aimed to determine the severity of SARS-CoV-2 infection in pediatric population compared to adults by analyzing LOS, medical expenses, hospitalization, and ICU admission. The average hospitalization days for children aged 0–9 was 26.2 days and 22.4 days for patients aged 10–19, which was about 8 days and 11.8 days shorter, respectively, than those aged 80 or older (34.2 days). Even when other variables were corrected, children aged 0–19 were found to have a shorter hospitalization period than those of older age groups. The medical expense analysis by age showed that the average medical expense for children was approximately 4,900 USD lower than that of patients aged over 80 years. The linear regression analysis also showed that children 0–9 years of age spent 87%, and those aged 10–19 spent 118% less on medical expenses than those aged 70 years and above, even after correction of other variables. The probability of hospitalization was the lowest at 10–19 years old (67.2%), which was 95% lower compared to patients aged 70 years or older, and also, their ICU admission rate was the lowest at 6.3%. On the other hand, the likelihood of hospitalization and ICU admission was the highest among children aged 0–9 years and generally patients under 50 years of age.
Our study findings were similar to those of a United States study that compared the LOS between children and adults with SARS-CoV-2 infection. This study analyzed patients who were hospitalized due to SARS-CoV-2 infection from 13 March to 17 May 2020 and compared clinical outcomes of patients aged < 24 years (n = 65) and adult patients (> 24 years, n = 60). According to the results, patients under the age of 24 stayed in the hospital for an average of 6.37 days, while the average of LOS in patients aged < 24 years was 14.77 days. Among the patients under 24 years, the average hospitalization period was 4.84 days for patients with mild symptoms, and of patients who were on a ventilator or died, the average hospital stay was 4.5 times longer (21 days) than the other patients in the same age group. In patients under 21 years of age with Multisystem Inflammatory Syndrome (MIS), the average hospitalization period was 8.10 days, which was about 2 times higher than that of patients with mild symptoms.13 Considering the results, younger patients had shorter hospital stays than adults.
In the present study, it was confirmed that the medical expenses were the lowest among patients aged 10–19 years old and highest among patients 80 years or older. A study in China has also suggested that younger patients spend less on medical expenses. The average cost of medical expenses for patients aged 0–34, including children, was the lowest (2,752 USD), while the average cost for those aged 70 and above was approximately five times higher than that of the younger age group (11,668 USD). This study assumed that most of the older people already had an underlying disease, and the presence of diseases may have influenced the high medical expenses.14 However, in our study, even after correcting for severe underlying diseases through CCI score, the medical expense for the elderly was still high. This could be attributed to age-related immune system changes, which may be relevant not only to the age-related illnesses but also susceptibility to infectious diseases.15
Our results also showed that the higher the age, the higher the probability of admission, and patients aged 10–19 years had the lowest admission rates. According to the recent study on the Financial Burden of Hospitalization of Children with COVID-19 in Korea, medical cost increased with age, but similar to our results, it was measured lower in children aged 11–15 years compared to 6–10 years. In addition, in terms of medication use, it was also less prescribed in patients aged 11–15 years. These results suggest that the severity of coronavirus is low in the teenage group.16 In another study that evaluated the severity of SARS-CoV-2 infection in patients admitted in hospital and ICU in the United States, Hospital and ICU admissions rates also showed a trend of increasing with age, but the hospital admission rate for patients aged 0–19, was 2.5%, this was the lowest compared to other age groups, and there were no ICU admission cases.17
Overall, the severity of SARS-CoV-2 infection in patients under the age of 19 years was lower than in adults, and among the younger patients, in particular, 0–9 years old are more likely to develop serious symptoms than those aged 10–19 years. Similar to our findings, some studies already in China showed that infants can develop severe illness when infected with the SARS-CoV-2. Researchers analyzed the confirmed and suspected COVID-19 pediatric patients aged 0–15 years reported from January 16 to February 8, 2020. They revealed that the proportion of COVID-19 patients with severe and critical illness among infants was highest in patients < 1 year (10.7%), 7.3% in 1–5 years, and 4.2% for the patients aged 6–10 years. Based on our results, the lower the age, the higher the probability of poor prognosis.2 In addition, a cohort study of 25 confirmed COVID-19 pediatric patients in Hubei, China, showed that two severely ill patients were infants under the age of 1 year who had symptoms of secondary bacterial pneumonia. This study conjectured that bacterial pneumonia, which is prevalent in infancy, may be the cause of the poor prognosis.18 Currently, in Korea, self-treatment measures have been proposed for pediatric patients with a low risk of complications among children aged 0–12 years, and from March 2021, children under the age of 8 years will be attending school every day under COVID-19 response measures. However, based on this and previous studies, the severity of SARS-CoV-2 infection was lowest at the age of 10–19 years, the age for children who are less likely to develop more severe symptoms should be adjusted in the mitigation measures.
Our study confirmed that children are less likely to develop severe COVID-19 symptoms; children aged 10–19 years especially, showed a rapid recovery rate and low severity. These results showed a pattern similar to studies conducted in other countries,19 although there were different COVID-19 hospitalization and discharge measures. This could be attributed to age-related body changes, and some studies suggested that the changes influence the body's response through the following mechanisms: First, the SARS-CoV-2 S protein adheres to the angiotensin-converting enzyme (ACE) 2 and penetrates into the human body. But, because this enzyme may be less developed at a younger age, children are protected from coronavirus infection.2021 Second, in the body SARS-CoV-2 is split into two by TMPRSS2, a protein on the surface of human cells. These cracked proteins interact with the cell surface, and RNA is brought into the cell to proliferate. Therefore, the severity of SARS-CoV-2 infection is related to the activity of TMPRSS2 in the body; the expression of this protein increases significantly as the body ages, consequently, the severity of SARS-CoV-2 in the elderly. On the contrary, children have very low levels of TMPRSS2 expression, so they may be relatively protected against severe forms of COVID-19.22 Lastly, children's immune systems response to the SARS-CoV-2 infection is different from that of adults. In the human body, there are many T cells that respond to viruses and regulate immunity. In severe cases of coronavirus, T cells decrease, resulting in decreased antiviral ability. However, there are more T cells in the children's body than in adults; the T cells suppress inflammatory reactions preventing them from developing into severe symptoms. In addition, there are many regulatory T cells, such as interleukin-10 (IL-10) in the lung tissue of children; IL-10, which inhibits inflammatory factors such as the harmful cytokine interleukin 6 (IL-6), may protect the children from SARS-CoV-2 infection.23
This study has a few limitations. First, since the residential treatment centers have been operating since March 2020, patients with mild symptoms, who were diagnosed with COVID-19 before March, were defined as hospitalized patients. Therefore, it is possible that the number of severe cases was inaccurate. In addition, there may have been errors in determining the severity because patients' clinical information by age was not contained after coronavirus infection. Nevertheless, this study attempted to increase the sensitivity of the analysis results by using four outcome variables in order to compensate for the lack of clinical information.
This study demonstrates low severity of SARS-CoV-2 infection in younger patients (0–19 years) by analyzing the LOS, medical expenses, hospital, and intensive care unit admission rates as outcome variables. Since the possibility of developing severe SARS-CoV-2 infection symptoms at the age of 10–19 was the lowest, mitigation strategies should be implemented not only to children aged 0–12 years but to middle and high school students. However, in children, COVID-19 is asymptomatic, and therefore they can be silent spreaders. Therefore, mitigation strategies must include thorough management and quarantine rules. Examples are some European countries, such as Belgium, which have fully reopened schools along with exhaustive preventive measures.24 However, children with underlying diseases need to be protected from high-risk infection environments. This study additionally tried to determine the severity of SARS-CoV-2 infection in children according to their social characteristics, but the results showed no statistically significant difference. However, earlier reports suggested that children's social factors may affect the severity of SARS-CoV-2 infection.25 For further clarification, additional studies with larger samples are required. This will help to select groups vulnerable to SARS-CoV-2 infection among children and provide priority support for them.
Go to :
 XML Download
XML Download