

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hepatitis C virus (HCV) is a major cause of chronic liver disease including liver cirrhosis (LC), hepatic decompensation, and hepatocellular carcinoma (HCC).12 Before the introduction of direct-acting antiviral (DAA) agents, the only treatment option was pegylated interferon (IFN) plus ribavirin (RBV).345 IFN-based treatments have been shown to produce a sustained virologic response 12 weeks (SVR12) after treatment completion in 70–80% of patients with chronic HCV genotype 2 infection.678 In Asian countries, SVR12 was found to be 95–100% in patients treated with sofosbuvir (SOF) plus RBV (SOF + RBV), which is higher than that estimated in Western countries.910 Treatment with glecaprevir/pibrentasvir (G/P) resulted in SVR12 > 95% when administered for 8 to 16 weeks in registered phase II and III trials.11121314 In addition, SVR12 is associated with reduced liver-related morbidity and mortality risks.1516
Current HCV treatment guidelines emphasize the need for a simplified treatment, such as the SOF plus velpatasvir (SOF + VEL) and G/P combinations.317 According to the American Association for the Study of Liver Diseases in 2019 and the European Association for the Study of the Liver in 2020, which establish the global standard treatment guidelines, SOF + VEL or G/P are the first recommended drug regimens for patients who have never received HCV therapy, regardless of genotype and the presence of compensated LC.317 SOF + RBV was the only IFN-free therapy in Korea for patients with genotype 2 infection prior to the Korean Society of Liver Association (KASL) in 2017 guideline update, but G/P therapy was subsequently added, and insurance coverage was secured in 2018.1819202122 The aim of our study was to investigate the effectiveness and safety of SOF + RBV and G/P regimens in Korean patients with HCV genotype 2 infection in real-world clinical practice.
Go to : 
METHODS
Patients
We retrospectively analyzed clinical data of adult patients (≥ 18 years old) with HCV genotype 2 infection treated with SOF + RBV from September 2015 to January 2019, and with G/P from January 2018 to February 2019 at seven university hospitals in the Korean southeast region. Patients with active HCC, or human immunodeficiency virus infection were excluded.
Treatment protocol
In the SOF + RBV treatment group, patients were administered SOF (SOVALDI®; Gilead Sciences, Foster City, CA, USA) 400 mg/day plus weight-adjusted RBV (VIRAMID®; IlsungPham., Seoul, Korea), and patients weighing < 75 kg and ≥ 75 kg were administered 1,000 mg/day and 1,200 mg/day, respectively. In patients with decompensated LC, RBV can be started at a dose of 600 mg daily, which can subsequently be adjusted depending on tolerance. RBV dose modifications were decided by the attending physician based on laboratory data and the contemporary KASL guidelines. Treatment lasted 12 weeks and 16 weeks for patients with chronic hepatitis and LC, respectively.
Patients in the G/P group were orally treated with a combination of 300 mg glecaprevir and 120 mg pibrentasvir (Mavyret®; Abbvie, North Chicago, IL, USA) once daily for 8 and 12 weeks for chronic hepatitis and LC, respectively.
LC was diagnosed based on histological or radiological evaluations. Compensated LC was restricted to Child-Turcotte-Pugh (CTP) class A.
Study assessments
The primary study outcome was to evaluate the proportion of patients who achieved sustained virologic response (SVR), which was defined as undetectable serum HCV RNA levels 12 weeks after end of treatment, as measured using polymerase chain reaction (PCR). HCV RNA was measured using a real-time PCR assay, and the lower limit of HCV RNA quantification was 15 IU/mL at all centers. Virologic response, defined as undetectable serum HCV RNA, was assessed during week 4 of treatment rapid virologic response (RVR), end of treatment (EOT) and week 12 SVR post-treatment. Failure to treat HCV infection included nonresponse, breakthrough, relapse, and medication discontinuation.
Nonresponse was defined as an increase in serum HCV RNA levels despite an initial decrease during treatment. Breakthrough was defined as detectable HCV RNA after its initial disappearance during treatment. Relapse was defined as the observation of undetectable serum HCV RNA at the EOT, which becomes detectable between the EOT and 12 weeks after therapy completion. Adverse events (A/Es) were identified by reviewing medical records and additional data (onset time, severity, and duration) were confirmed through discussions with co-authors at each hospital. All methods of assessing treatment A/Es were in accordance with the Common Terminology Criteria for Adverse Events.
Statistical analyses
SVR rate was assessed in the full analysis set (FAS), which consisted of all patients who received at least one medication dose and the per-protocol set (PPS), which only included patients who completed the viremia evaluation at 12 weeks after the completion of the set period of treatment. Between group comparisons of categorized variables were conducted using the χ2 test or Fisher's exact test, and continuous variables were determined using Student's t-test or Mann-Whitney U test, as appropriate. The correlation between variables was analyzed using the Cox regression model and statistical significance was defined as P < 0.05.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Dong-A University Hospital and the requirement for informed consent was waived (IRB number: DAUHIRB-19-087). Our study was approved by the institutional review board of each participating hospital.
Go to :
RESULTS
Patient baseline characteristics
A total of 1,096 patients were treated with SOF + RBV or G/P. Of these, 953 were treated with SOF + RBV, of which 59 (47 failed follow-up due to unknown causes and 12 discontinued the drug owing to A/E) did not complete treatment, and 894 patients completed the treatment. Among these, 33 patients in SOF + RBV group and 14 patients in the G/P group did not undergo the SVR12 test (Fig. 1).
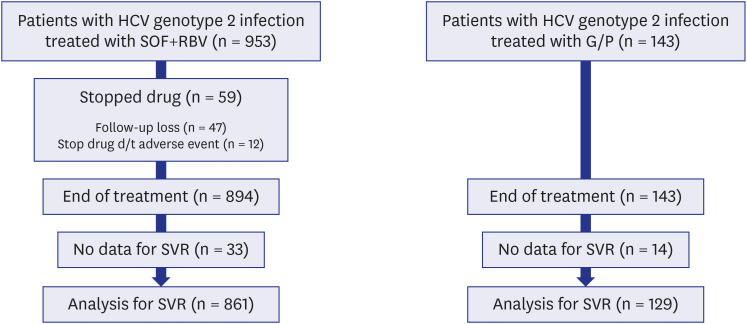
Table 1 shows the baseline characteristics of the patients; those in the SOF + RBV group had a mean age of 61 years and 545 (57.2%) were female. Furthermore, 285 (30%) patients had LC, 253 (26.5%) had CTP class A, 28 had decompensated LC with CTP class B, and 4 had decompensated LC with CTP class C. In addition, 224 (23.5%) patients had fatty liver (FL) and 49 (5.1%) had a prior history of HCC. The mean baseline HCV RNA level was 2.6 × 106 IU/mL and two patients (0.2%) had an estimated glomerular filtration rate (eGFR) < 30.
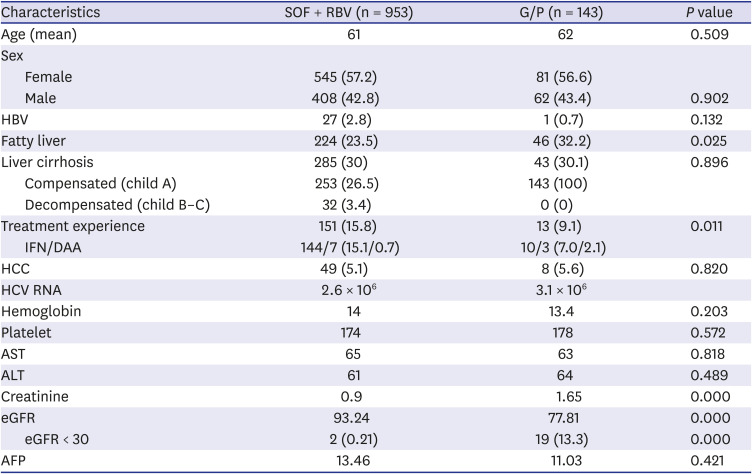
Table 1
Baseline characteristics of patients according to antiviral regimen
Values are presented as number (%).
SOF = sofosbuvir, RBV = ribavirin, G/P = glecaprevir/pibrentasvir, HBV = hepatitis B virus, IFN = interferon, DAA = direct-acting antiviral,
HCC = hepatocellular carcinoma, HCV = hepatitis C virus, AST = aspartate transaminase, ALT = alanine transaminase, eGFR = estimated
glomerular filtration rate, AFP = alpha-fetoprotein.
![]()
Patients in the G/P group had a mean age of 62 years, 81 (56.6%) were female, and 43 out of 143 (30%) patients had compensated LC. In addition, 46 (32.2%) patients had FL and 8 (5.6%) had a prior history of HCC. The mean baseline HCV RNA level was 3.1 × 106 IU/mL and 19 (13.3%) patients had an eGFR < 30. Comparing the baseline characteristics of the two groups (Table 1), more patients had FL and low eGFR in the G/P group than in the SOF + RBV group.
Treatment response
Table 2 shows the virologic response of the SOF + RBV and G/P groups. The FAS analysis of the SOF + RBV group showed the SVR to be 89% (848/953), whereas in the PPS analysis it was 98.3% (846/861). The corresponding values in the G/P group were 89.5% (128/143) and 99.2% (128/129), respectively. The PPS analysis showed that the SVR was excellent with the SOF+RBV and G/P regimens.
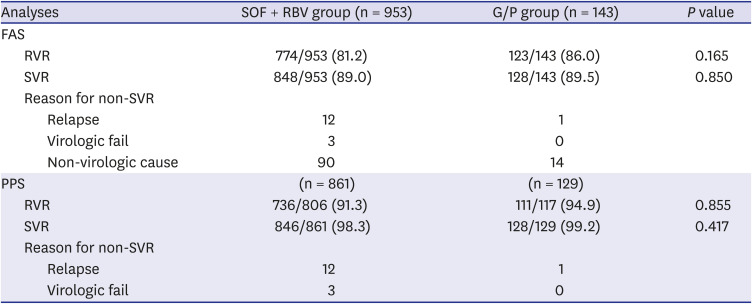
Table 2
Virologic response according to antiviral regimen
SOF = sofosbuvir, RBV = ribavirin, G/P = glecaprevir/pibrentasvir, FAS = full analysis set, PPS = per-protocol set, RVR = rapid virologic response, SVR = sustained virologic response.
![]()
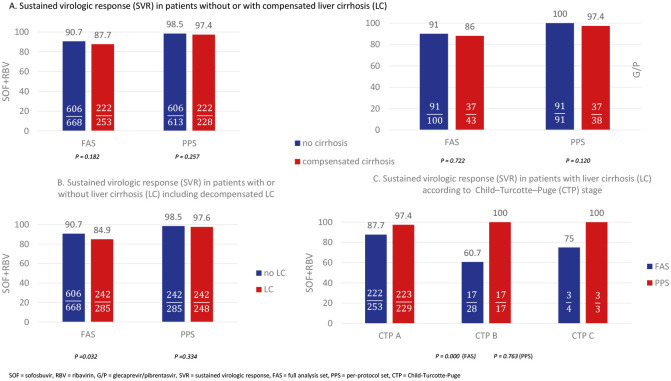
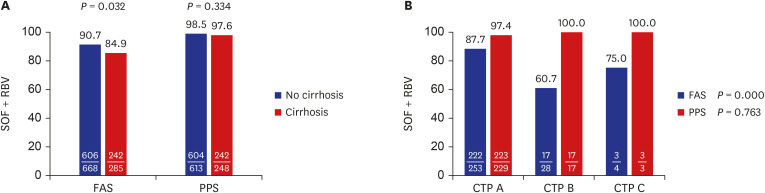
No patients had decompensated LC in the G/P group, while 32 patients with decompensated LC were included in the SOF + RBV group. PPS analysis of the SVR according to the patients with LC in the SOF+RBV group (Fig. 2A) revealed no difference, while the FAS analysis of the same showed a significant difference (90.7% vs. 84.9%, P = 0.032). The FAS analysis of SVR according to the CTP stage showed a statistically significant difference (Fig. 2B).
Clinical factors associated with SVR12
Prognostic factors affecting SVR12 in both groups were analyzed in the PPS (Table 3). Baseline aspartate transaminase (AST), alanine transaminase (ALT), eGFR, HCV RNA, presence of HBV infection, FL, LC, and previous treatment did not affect the SVR12, whereas male sex (P = 0.032) and history of HCC (P = 0.013) were significantly associated with SVR12 in the multivariate analysis.
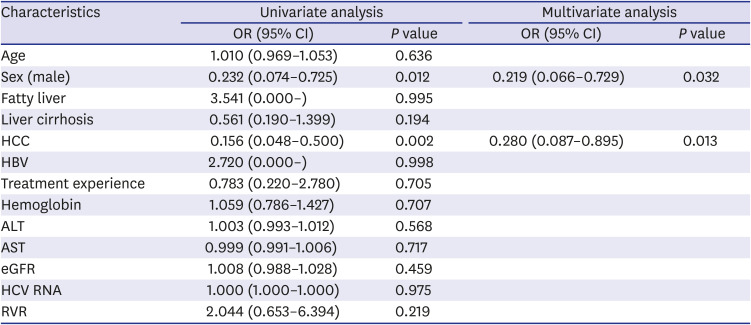
Table 3
Predictive factor analysis for sustained virologic response
OR = odds ratio, CI = confidence interval, HCC = hepatocellular carcinoma, HBV = hepatitis B virus, ALT = alanine transaminase, AST = aspartate transaminase, eGFR = estimated glomerular filtration rate, HCV = hepatitis C virus, RVR = rapid virologic response.
![]()
Of 861 patients, the 806 analyzed for RVR consisted of 736 (91.3%) and 70 (8.7%) who did and did not achieve RVR, respectively. SVR12 rates in patients who did and did not achieve RVR were 98.5% (725/736) and 98.6% (69/70), respectively (P = 0.965). RVR was not a significant factor for SVR12.
Characteristics of patients who did not complete SOF + RBV treatment
Table 4 shows the baseline characteristics of 59 (6.2%) patients who started but did not complete the SOF + RBV treatment. The multivariate analysis showed that low hemoglobin (Hb), high ALT, and decompensated LC affected the treatment completion.
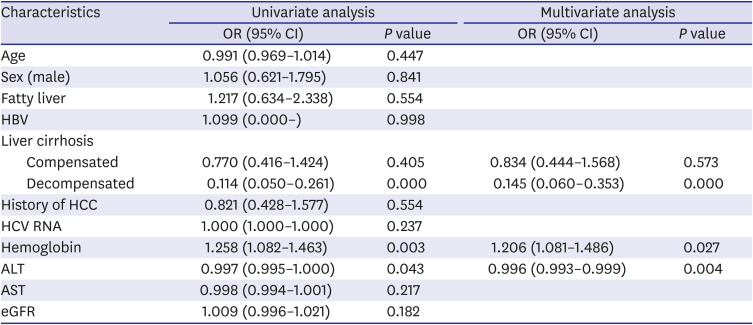
Table 4
Predictive factor analysis of patients who did not complete the sofosbuvir plus ribavirin treatment
OR = odds ratio, CI = confidence interval, HBV = hepatitis B virus, HCC = hepatocellular carcinoma, HCV = hepatitis C virus, ALT = alanine transaminase, AST = aspartate transaminase, eGFR = estimated glomerular filtration rate.
![]()
Characteristics of patients who relapsed during G/P treatment
Only one patient treated with G/P for 12 weeks experienced a relapse. This was a 74-year-old man with HCV genotype 2a + 2c infection who had not been previously treated for HCV infection. The patient had compensated LC and eGFR < 15, but not HBV or FL. Treatment response was evaluated as responsive in RVR and ETR, but as relapse in SVR12.
Safety and tolerability
A/Es were reported in 569 (59.7%) and 37 (25.9%) patients in the SOF + RBV and G/P groups, respectively (Table 5). The most common A/E in the SOF + RBV-treated patients was anemia (517 patients, 54.2%), followed by hyperbilirubinemia (167 patients, 17.5%) and fatigue (125 patients, 13.1%). Elevated ALT, pruritus, rash, headache, and gastrointestinal disorder were reported in < 10% of patients. Four patients died, including two of liver failure due to LC progression and two of pneumonia. Death caused by pneumonia was considered unrelated to treatment with the antiviral medications. The most common A/E in G/P-treated patients was gastrointestinal disorder (13 patients, 9.1%), followed by fatigue (8 patients, 5.6%). Other A/Es were reported in < 5% of patients. Elevated bilirubin levels and the prevalence of anemia and fatigue were significantly higher in the SOF + RBV group than in the G/P group.
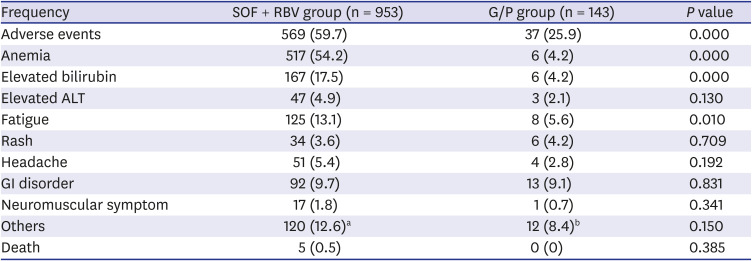
Table 5
Adverse effects according to treatment group
Values are presented as number (%).
SOF = sofosbuvir, RBV = ribavirin, G/P = glecaprevir/pibrentasvir, ALT = alanine transaminase, GI = gastrointestinal.
aSomnolence, cough, weight loss, panic disorder, hair loss, decreased renal function, fever, thirst, ascites, edema, weakness, dyspnea, herpes zoster, urticaria, left middle cerebral artery infarction, facial edema, hepatic encephalopathy, hypothyroidism, anorexia, dizziness, hot flush, chest discomfort, malignant lymphoma, dyspnea on exertion; bDuodenal ulcer bleeding, cough, presyncope, somnolence, weakness, elevated blood pressure, edema, dizziness.
![]()
Go to :
DISCUSSION
Following the development of pangenotypic DAA, low A/Es and close to 100% SVR12 have been reported in the treatment of HCV infection. HCV genotype 2 is the second largest HCV genotype in Korea, SOF + VEL and G/P regimens are recommended worldwide for this genotype.17 In Korea, SOF + RBV or SOF/ledipasvir and G/P are the drugs that are covered by insurance for the treatment of HCV genotype 2 infection, whereas for decompensated LC, SOF + RBV is the only drug regimen covered by insurance. Our study aimed to analyze not only the effectiveness and safety of the SOF + RBV and G/P regimens in real-world practice, but also the treatment completion rate and causes of treatment failure.
We adopted FAS rather than intention-to-treat (ITT) analyses, which are commonly performed in other studies. In our study, the SVR12 of the SOF + RBV group was 89% and 98.3% in the FAS and PPS analyses, respectively. In comparison, the SVR12 of the ITT and PP sets in a real-world multicenter Japanese study were 96.8% and 97.6%, respectively,23 and it was 100% in the PP set of a phase III study from Taiwan.10 In our study, the PPS results showed no significant differences compared to real-world studies conducted in other countries; however, the SVR12 was significantly lower in the FAS. This discrepancy was likely attributable to the different patient criteria included in the analysis.
In our study and in the Japanese study, FAS and ITT were defined as constituting all patients who were administered the prescribed durg. However, in our study, 59 patients did not complete treatment, and in the Japanese study, treatment was prematurely withdrawn in only 10 patients.1023 Treatment completion was shown to influence treatment outcome, because SOF + RBV-treated patients who underwent the HCV RNA test after completing the 12-week treatment showed excellent SVR. Factors influencing treatment completion were analyzed and low baseline Hb, high ALT, and decompensated LC were found to affect the completion of treatment. Therefore, low baseline Hb or high ALT were considered to probably affect incidences of A/Es and early dropout.
A few 3.4% (n = 32) of the patients in the SOF + RBV group had decompensated LC and not much research is available on the efficacy and safety of DAA in patients with decompensated LC.24 Recently, Dr. Michael P. Curry and the ASTRAL-4 investigators conducted a study using SOF and VEL with or without RBV to treat adult patients with chronic HCV infection with decompensated LC. The overall SVR rate following a 12-week treatment with SOF + VEL was 83%, and 94% when weight-based RBV was added. Furthermore, a 24-week treatment with SOF + VEL cured 86% of the patients. The differences between groups were not statistically significant. The combined overall SVR rate using SOF + VEL with or without RBV was 88%.2526
In our study, SOF + RBV-treated patients with decompensated LC showed 100% SVR after treatment completion, although the dropout rate was 37.5% (12/32) (Fig. 2B). This observation suggests that choosing SOF + RBV, which is the only available therapeutic agent for decompensated LC with HCV genotype 2 infection in Korea requires monitoring to encourage treatment completion. Moreover, careful monitoring is also needed for patients with low baseline Hb or high ALT.
In G/P-treated patients, SVR12 was 89.5% and 99.2% in the FAS and PPS groups, respectively. Contrary to our expectation, the relatively low SVR12 in the FAS analysis was due to the failure to test for SVR12, and the G/P regimen would be expected to show high SVR with both the FAS or PPS analyses as indicated by the results of other studies. In a real-world study reported from Italy, the SVR rates for the G/P treatment were 94% in the ITT set and 99.3% in the PP analysis (8 weeks vs. 12 or 16 weeks: 99.2% vs. 100%).27 In Japan, the ITT and PP analyses showed SVR rates of 92.8% and 99.2%, respectively only for an 8-week treatment.28
In the PPS analysis of all patients treated with SOF + RBV or G/P, univariate and multivariate analyses were performed for factors affecting SVR12. The results showed that age; presence of FL; HBV; LC; previous treatment; and baseline laboratory findings such as AST, ALT, GFR, HCV RNA, and RVR did not affect SVR. Furthermore, RVR was an important predictor of SVR when IFN therapy served as the main treatment protocol for chronic hepatitis C; however, for DAA treatment, RVR was no longer meaningful.
In the multivariate analysis, male patients and those with HCC showed a lower SVR12 than other patients and although the reason was unclear, adherence to medication, relatively higher HCC history (male patients: 9.2% vs. female patients: 2.4%, P = 0.000), and biological factors were associated with significantly lower SVR12 in male patients.23272829 Generally, similar to other studies, patients with a history of HCC showed significantly lower SVR than those with no history. In a previous meta-analysis, patients who presented with an HCV genotype 2 infection with HCC and who were treated with SOF + RBV (n = 125) reported a lower SVR than the patients presenting with an HCV genotype 2 infection without HCC (n = 2,743; 81.4%; 95% confidence interval [CI], 70.6–90.4% vs. 92.8%; 95% CI, 87.2–96.9%).29
The effect of HCC on low SVR is unknown, but the following hypotheses have been proposed. First, when comparing patients with and without HCC, SVR was thought to be influenced by factors such as age and LC, because patients with HCC were older and had more advanced LC than those without HCC. Second, HCC may be associated with lower SVR rates. Because the HCV is present in HCC cells, it may be inaccessible to DAA, thus, reducing their antiviral effect. Lastly, HCC develops in chronically inflamed liver tissue and destroys the structure, leading to conditions that may alter hepatic immune responses and reduce the response to DAA. Therefore, the importance of HCC is associated with the HCC environment rather than the HCC itself.3031
More A/Es were observed in the SOF + RBV group than in the G/P group, and 1.26% (n = 12) of the patients discontinued the medication. Anemia was observed in 54% of all patients and 18.2% experienced ≥ grade 2. Based on this observation, a low Hb baseline was considered a major cause of SOF + RBV treatment discontinuation and therefore, close monitoring and adequate RBV dose reduction may be required for patients with anemia.
Although there was a large number of patients in our multicenter study, there were some limitations. First, the enrolled patients were residents of Busan-Ulsan-Gyeongnam and therefore, caution should be exercised while applying these findings to all patients infected with the HCV genotype 2 in Korea and worldwide.
Second, the multicenter retrospective study design would make it difficult to identify the causes of the loss of patients during the follow-up period. Third, patients were enrolled for G/P treatment for 8 and 12 weeks in the groups with or without LC, but this was unified to 8 weeks of treatment. Lastly, some A/Es might have been missed because of the retrospective nature of the analysis and because each center had a different method of recording A/Es, with no consistent evaluation standard. Nevertheless, our study can be considered meaningful because it highlights the importance of early treatment of patients before their liver function worsens. Furthermore, we emphasized the need for precautions in real-world practice by identifying reasons for patient dropout and factors affecting treatment completion.
In conclusion, the SOF + RBV and G/P treatment regimens showed high effectiveness and safety for patients with HCV genotype 2 infection in a real-world setting, regardless of their baseline background characteristics such as age, sex, fibrosis stage, and renal function, upon treatment completion. Male sex and HCC history were negative factors for SVR, but male patients also did show a high SVR. The relatively low SVR identified in the FAS analysis was due to missing SVR12 data but in real practice, the G/P regimen can be expected to have high drug compliance, low A/Es, and high SVR in patients with no LC or compensated LC. SOF + RBV is the only therapeutic agent used in Korea for the treatment of patients with decompensated LC who have HCV genotype 2 infection.
Our study showed a high SVR in patients who completed the treatment, indicating the importance of effectively managing A/Es following treatment initiation and on completion. Patients with low Hb levels require special attention and monitoring before the initiation of SOF + RBV treatment. It is most important to select drugs with low incidences of A/E and high compliance and to treat patients early before the liver function worsens. Therefore, efforts to eradicate hepatitis C by implementing rapid treatment through early screening are necessary.
Go to :
 XML Download
XML Download