

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cognitive screening studies have shown that cognitive function scores increase rapidly in young children, and tend to peak in early adolescence.12 Children and adolescents are at a critical period of cognitive functional development, which has important influence on social adaptive function, including academic performance.34 Some medical illnesses, such as diabetes mellitus, idiopathic epilepsy, and β-thalassemia, may lead to cognitive impairment in children.567 Neurocognitive impairment, owing to the deterioration of kidney function, has been reported in various studies on children with chronic kidney disease (CKD)8910; however, despite improvements in their medical management, there are concerns regarding neurocognitive function in children with CKD.
While previous studies have reported lower intelligence quotients (IQs) in children and adolescents with CKD than in age-matched controls, it has also been reported that the deterioration of cognitive function varies according to the stage of CKD.8911 Additionally, a recent meta-analysis of neurocognitive and educational outcomes in children with CKD suggested that they may have a lower average cognition than the general population.12
Childhood and adolescence are important time periods of brain myelination and synaptic development13; thus, the neurocognitive impact of CKD and its associated clinical symptoms are of great concern. Among the various neurocognitive functions is intelligence, which refers to the ability to apply information and experience to accomplish challenging new tasks and has various educational and clinical implications. Intelligence testing is a comprehensive psychological measurement tool that measures and understands individual differences in intellectual characteristics. Intelligence testing can therefore predict ones' adaptability, education potential, or occupation, and it has great significance in research with respect to understanding children's neurocognitive function.14
Despite the important implications of intelligence, there is limited research on cognitive function in children and adolescents—compared with adults—with CKD, and few studies have used standardized intelligence testing. Particularly, there are no studies on intelligence in children and adolescents with CKD in Korea, and there are few studies on the clinical and sociodemographic factors related to intelligence in children with CKD. This study therefore aims to investigate the mean intelligence, as well as clinical and sociodemographic variables related to intelligence, in a pediatric CKD cohort in Korea.
METHODS
Study design and subjects
The KoreaN cohort study for Outcomes in patients With Pediatric Chronic Kidney Disease (KNOW-Ped CKD) is a prospective observational study that enrolled 437 participants aged under 18 years at seven pediatric nephrology centers across South Korea between April 2011 and March 2019.1516171819 The study design and its methods have been previously described.20
In this study, participants enrolled in the KNOW-Ped CKD were those who underwent standardized IQ testing. After excluding participants with central nervous system-related diseases, developmental delay, and cerebral palsy, a total of 81 participants were analyzed.
Intelligence test
The Korean-Wechsler Adult Intelligence Scale-Fourth edition (K-WAIS-IV), a modified and standardized WAIS-IV for the Korean population, is a standardized intelligence test that can measure intellectual characteristics in 16–69-year-olds.2122 The K-WAIS evaluates full-scale IQ, along with verbal and performance IQs, and was conducted in participants over 16 years of age. The Korean-Wechsler Intelligence Scale for Children (K-WISC-III) is standardized for Korean children by Kwak et al.,23 and based on the WISC-III. The test is suitable for children aged 6–16 years, and comprises verbal subtests and performance tests, which provides not only the full-scale IQ score, but also verbal and performance IQ scores. The K-WISC-IV, which is the newly revised fourth edition of the intelligence test for children developed by Wechsler, was standardized by Kwak et al.24 for the assessment of Korean children. This test provides full-scale IQ scores and four indicators: verbal comprehension, perceptual reasoning, working memory, and processing speed. The K-WISC-III or K-WISC-IV was performed at 6–18 years of age according to the available tests at each institution. In this study, the full-scale IQs of participants were analyzed.
Statistical analyses
Descriptive statistics for demographic characteristics and clinically-related variables were analyzed. Categorical variables were expressed as percentages, while continuous variables were expressed as mean ± standard deviation. Full-scale IQ was compared between groups using the independent t-test, and Pearson's correlation coefficients for continuous variables were used to determine the association between laboratory findings and full-scale IQ. The analysis of variance test was used to determine the correlation between use of vitamin D supplements and the biochemistry of bone mineral metabolism, whereas multivariate linear regression analysis was used to determine which CKD-related variables were associated with the full-scale IQ. Statistical analyses were performed using IRB® SPSS® statistics 24.0 for Windows (IBM Corp., Armonk, NY, USA).
Ethics statement
This study was approved by the institutional review boards of the participating centers in South Korea, namely Jeju National University Hospital (Jeju, JEJUNUH-2013-11-019-002), Pusan National University Children's Hospital (Yangsan), Severance Children's Hospital (Seoul), Kyungpook National University Children's Hospital (Daegu), Seoul National University Children's Hospital (Seoul), Samsung Medical Center (Seoul), and Asan Medical Center (Seoul). Children with CKD aged under 18 years were enrolled in this study after written informed consent was obtained from their parents or legal guardians according to the principles of the Declaration of Helsinki. This clinical trial is registered at the ClinicalTrials.gov, NCT number NCT02165878 (June 2014, https://www.clinicaltrials.gov/).
RESULTS
Baseline characteristics of the KNOW-Ped CKD
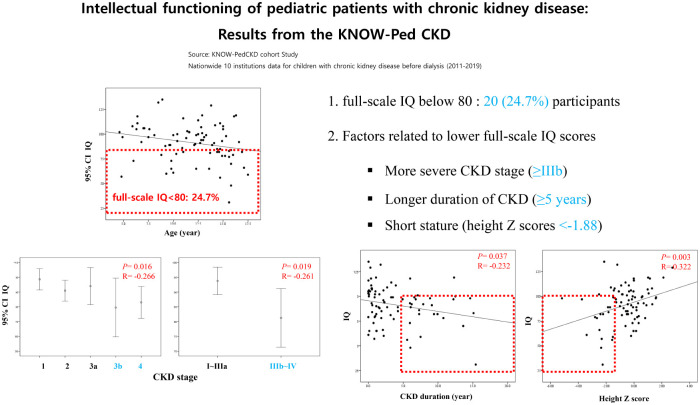
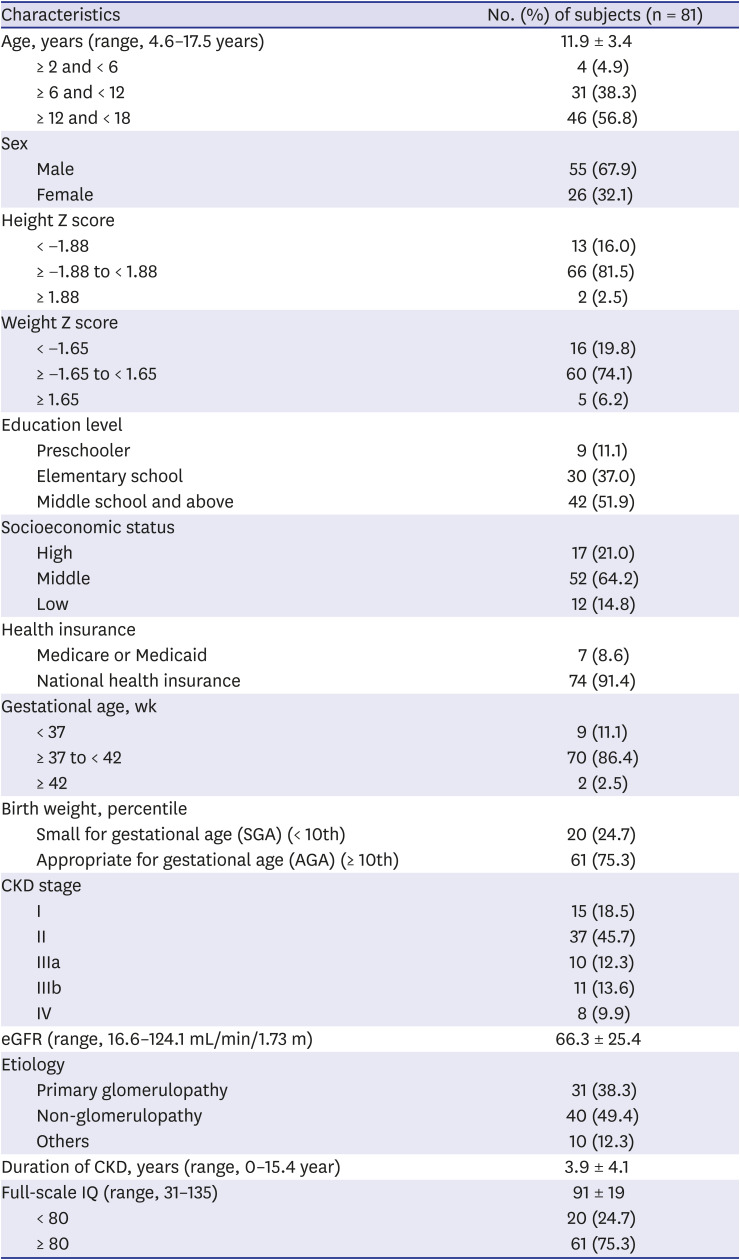
Of the 437 participants enrolled in the KNOW-Ped CKD, 81 participants were included in the study; the mean age was 11.9 ± 3.4 (range, 4.6–17.5) years. There were 55 males (67.9%) and 26 females (32.1%); 30 participants (37.0%) were elementary students, and 42 (51.9%) were middle or high school students. Seven participants (8.6%) were Medicare or Medicaid beneficiaries, and 9 (11.1%) had a history of preterm birth. There were 15 patients (18.5%) with stage I, 37 (45.7%) with stage II, 10 (12.3%) with stage III, 11 (13.6%) with stage IIIb, and 8 (9.9%) with stage IV CKD. The most common cause of CKD was non-glomerulopathy (49.4%), and 38.3% of participants had primary glomerulopathy. The mean duration of CKD was 3.9 ± 4.2 (range, 0.0–15.4) years; there were 26 patients (32.1%) with a CKD duration more than 5 years. The mean full-scale IQ score was 91 ± 19, and 20 participants (24.7%) had a full-scale IQ < 80 (Table 1).
Table 1
Clinical and demographic information
IQ difference according to demographic and CKD-related variables
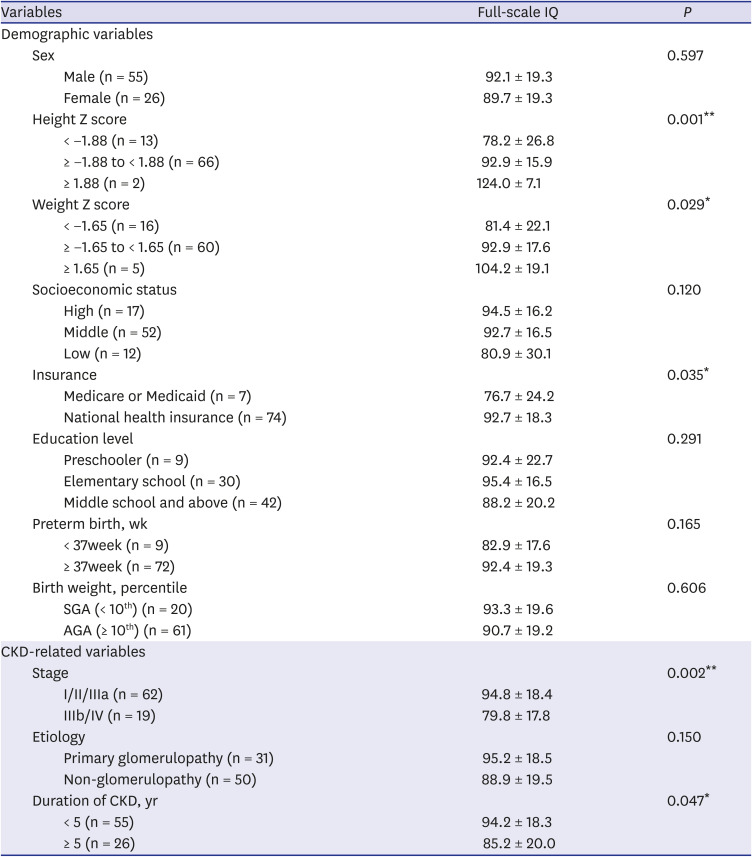
Full-scale IQ scores were significantly lower in children with a short stature (height Z scores < −1.88), failure to thrive (weight Z scores < −1.65), more severe CKD stage (≥ IIIb), longer duration of CKD (≥ 5 years), and those who were Medicare or Medicaid beneficiaries (Table 2). However, there were no differences between the groups in terms of sex, education level, preterm birth weight history, and etiology of CKD for the full-scale IQ. Additionally, there were no significant differences in intelligence between groups regarding full-scale IQ according to the presence of hypertension, proteinuria, and anemia, which are known risk factors for cognitive decline in patients with CKD (data not shown).
Table 2
Difference of the full-scale IQ according to demographic and disease associated variables
IQ difference according to laboratory findings and medication history
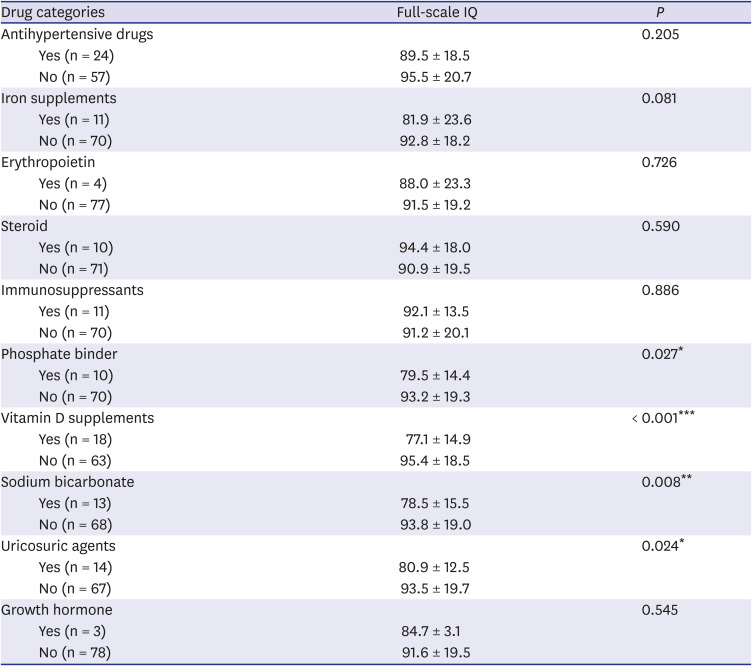
Lower serum calcium and higher phosphorus were positively correlated with the full-scale IQ (Fig. 1). Among the medications, there were significant differences in the full-scale IQ of participants with a history of phosphate binders (P = 0.027), vitamin D supplements (P < 0.001), sodium bicarbonate (P = 0.008), and uricosuric agents (P = 0.024) (Table 3).
Fig. 1
Correlation between laboratory findings and full-scale IQ.
IQ = intelligence quotient, PTH = parathyroid hormone, 1,25(OH)2D = 1,25-dihydroxyvitamin D, 25(OH)D = 25-hydroxyvitamin D.
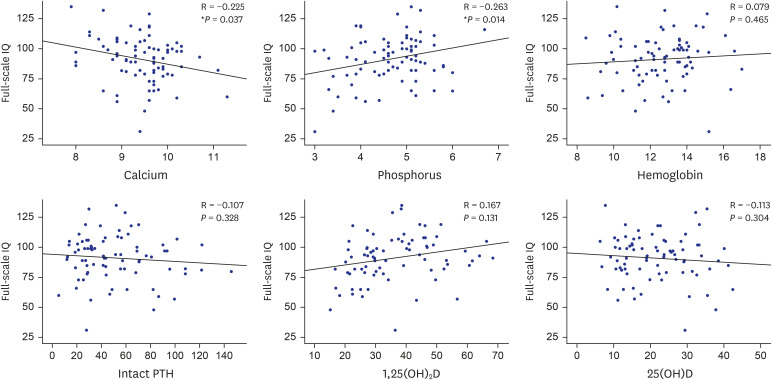
Table 3
Difference of the full-scale IQ according to medication history
Correlates of intellectual functioning in pediatric CKD
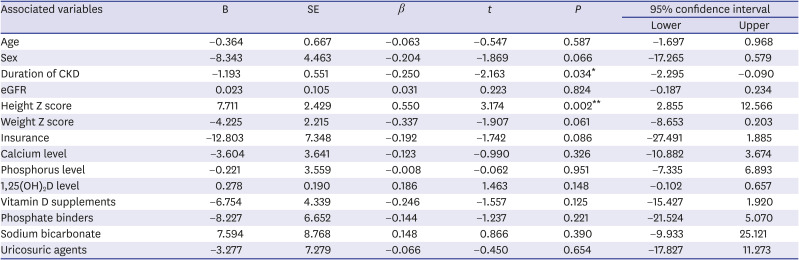
In our multivariate linear regression model, the association between the full-scale IQ and duration of CKD and height Z score remained significant after controlling for demographic and clinical variables regarding pediatric CKD (Table 4).
Table 4
Adjusted multivariable linear regressions to determine predictors of full-scale IQ
DISCUSSION
Our results demonstrated a mean intelligence of 91 ± 19 in the KNOW-Ped CKD. Previous studies have reported an intelligence of 76.8 ± 14.9 to 87.9 ± 2.7 in patients with end-stage renal failure,2526 while a total intelligence of 106 was reported in patients with autosomal recessive polycystic kidney disease in the Chronic Kidney Disease in Children (CKiD) cohort study.27 Our results are comparable with those of a previous study, in which 368 pediatric patients with mild-to-moderate CKD demonstrated an average intelligence of 96.4 ± 16.5.28 In a recent meta-analysis of neurocognitive outcomes in children with CKD, the mean intelligence was 92.7 as lower full-scale IQ.12
Growth retardation is a common complication experienced by children with CKD. Previous reports indicate that the growth rate of patients with CKD correlates with glomerular filtration rate (GFR); therefore, the association between short stature and cognitive decline in our study likely reflects that the GFR decline negatively affects cognitive function in pediatric CKD patients.29 Our results also showed that the mean intelligence of participants with a CKD duration longer than 5 years was significantly lower than those with a duration less than 5 years. Another previous study reported that a longer duration of CKD and a younger age at CKD onset have a negative impact on cognitive function, resulting in poor academic skills.1230 This suggests a decline in cognitive function, with prolonged uremic insults in the central nervous system. These results suggest that clinicians should consider an intelligence decline in children with a duration of CKD longer than 5 years, and should consider appropriate interventions in clinical practice. The effect of CKD on GFR affects IQ over time; therefore, early renal transplantation is thought to have a positive effect on IQ in children with CKD. This is supported by studies that have reported IQ recovery following early kidney transplantation.3132
In previous studies, children with mild-to-moderate CKD and higher blood pressure were reported to exhibit poorer performance in neurocognitive tests than those with a normal blood pressure.2833 Hypertension, identified through ambulatory blood pressure monitoring in children and adolescents with CKD, was independently associated with impairments in neurocognitive performance34; however, in this study, the difference in intelligence with or without hypertension was not significant. In addition, a previous study reported that children with CKD and proteinuria had lower IQs than those without proteinuria.28 A large amount of albuminuria was associated with poor cognitive function in the young general population35; however, there was no difference in intelligence according to the presence of proteinuria in our study. In healthy children, anemia is associated with decreased cognitive function,36 whereas anemia in adults with CKD is known to be a risk factor for neurocognitive function deterioration.30 Still, little is known about the relationship between anemia and cognitive function in children with CKD, and there are no studies on whether maintaining optimal hemoglobin levels helps to maintain cognitive function. The relationship between medical problems accompanying CKD—such as hypertension, proteinuria, and anemia—and cognitive function in pediatric CKD patients is still lacking in evidence, and varies according to medical problems, participant's age, cognitive function, and timing of evaluation. It is therefore necessary to investigate the effect of medical problems accompanying CKD on the development of cognitive function in children and adolescents.
Participants with intake of phosphate binders showed a relatively low mean intelligence. A previous study suggested a negative correlation between cognitive impairment and serum calcium in patients with moderate-to-severe CKD.37 This is similar to our results; however, the CKiD cohort study reported that calcium and phosphorus Z scores were not associated with cognitive test scores.38 The relationship between calcium and phosphate balance and cognitive function in pediatric CKD patients therefore requires further investigation.
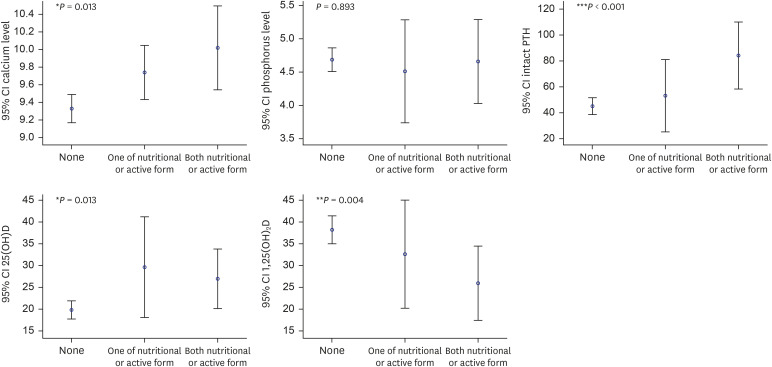
In our study, participants receiving both nutritional and active forms of vitamin D supplements had higher calcium, intact parathyroid hormone, and 25-hydroxyvitamin D (25[OH]D) levels; however, the level of 1,25(OH)2D was not elevated (Fig. 2). This suggests that although vitamin D supplementation increased the level of 25(OH)D, the level of 1,25(OH)2D did not increase correspondingly; it is therefore believed that mineral metabolism or uremic state disorders affect cognitive function in children with CKD, owing to the reduction in GFR.
Fig. 2
Correlation between vitamin D supplements and biochemistry of bone mineral metabolism.
CI = confidence interval, PTH = parathyroid hormone, 1,25(OH)2D = 1,25-dihydroxyvitamin D, 25(OH)D = 25-hydroxyvitamin D.
*P < 0.05, **P < 0.01, ***P < 0.001.
Low levels of 1,25(OH)2D and use of vitamin D supplements correlated with poor intelligence in our pediatric CKD cohort, and remained a risk factor for low intelligence after adjusting for demographic and clinical variables. Vitamin D acts through the vitamin D receptors—expressed in the hippocampus, hypothalamus, cortex, and subcortex, which are essential for cognition39—and plays both neuroprotective and regulatory roles in the central nervous system.4041 Vitamin D is hydroxylated to 25(OH)D in the liver, and is converted into its active form, 1,25(OH)2D by the enzyme 1α-hydroxylase in renal tubular epithelial cells. CKD patients are therefore susceptible to the development of 1,25(OH)2D deficiencies,42 and circulating 1,25(OH)2D may thus be superior to 25(OH)D as a marker of kidney disease severity.43 The results of our study suggest that a 1,25(OH)2D deficiency in pediatric CKD patients may directly affect the development of cognitive function, as well as reflect the severity of CKD by indirectly affecting cognition due to poor kidney function.
Some studies on adults with CKD have reported an association between vitamin D deficiency and cognitive decline444546; however, it has been reported that 1,25(OH)2D and 25(OH)D dysregulations do not mediate cognitive function impairment in advanced CKD.46 Data regarding the relationship between vitamin deficiency and cognitive function in pediatric CKD patients remains insufficient; therefore, further studies are needed to investigate this relationship.
There are some limitations to our study; first, as a cross-sectional study, cognitive decline was not observed with the progression of CKD. Further investigation of the risk factors associated with cognitive decline through follow-up of the cohort is needed. Second, it was assumed that the full-scale IQs of the K-WISC-III, K-WISC-IV, and K-WAIS-IV tests were identical. Previous studies have found the index scores of these tests to be largely similar; however, this remains controversial and caution must be exercised when interpreting the results. Third, a normal control group was not included in the study; although demographic variables such as socioeconomic status, education level, age, and sex were considered, various environmental factors that affect the development of intelligence were not investigated. Finally, our cohort included pediatric patients with CKD and multiple anomalies or syndromic CKD. Additionally, some patients were diagnosed with ADHD or autism; therefore, there were many limitations while evaluating cognitive function in our cohort. By excluding patients with underlying diseases that may affect cognitive function, 81 subjects with pediatric CKD were included in this analysis.
In conclusion, the mean intelligence of participants was of a low-average level, while being a Medicare or Medicaid beneficiary, having a low 1,25(OH)2D level, and intake of vitamin D supplements independently predicted low intelligence in pediatric CKD. Children and adolescents are at a critical period of cognitive functional development—which includes academic achievement and adaptation to social life—and is an important prognostic factor in pediatric CKD. Therefore, it is necessary to investigate the various risk factors for cognitive decline in children and adolescents with CKD, as well as to develop early interventions.
 XML Download
XML Download