

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Nephron-sparing surgery (NSS) is the standard treatment in surgical management of small renal tumors because of its excellent cancer control with less functional impairment.12 Several previous studies have reported that NSS for a renal tumor larger than 4 cm provides comparable perioperative and oncological outcomes to radical nephrectomy and that it is superior to radical nephrectomy in preserving renal functional outcomes.34567 Currently, if technically feasible, indications of NSS have been extended to larger, advanced renal tumors in terms of oncological and functional outcomes.8
Considering the invasiveness of open surgery, minimal invasive modalities such as laparoscopic and robotic surgery have gained more attention. Robot-assisted partial nephrectomy (RAPN) has various merits, including its ability to minimize pain, lessen bleeding, reduce hospital stay, and lower morbidity.9 In addition, surgical parameters of RAPN appear to be less affected by tumor complexity than laparoscopic partial nephrectomy (LPN).10 Mottrie et al.11 have described that RAPN is the real competitor of open surgery since it is able to bridge technical difficulties of LPN. However, there have been few studies comparing OPN and RAPN for renal tumors larger than 4 cm.
Thus, the aim of this study was to compare surgical parameters, functional outcomes, and oncological outcomes between OPN and RAPN for patients with single unilateral renal tumors larger than 4 cm with a normal contralateral kidney.
Go to : 
METHODS
Between June 2003 and April 2017, a total of 1,235 patients with primary renal tumor underwent NSS at Seoul National University Bundang Hospital, Seongnam, Korea. On preoperative computed tomography (CT), patients with bilateral disease, multiple tumors, solitary kidney, metastasis, or tumor size less than 4 cm were excluded. We retrospectively reviewed clinical records of 220 patients who underwent OPN (n = 92) or RAPN (n = 128) for a single renal tumor ≥ 4.0 cm with a normal contralateral kidney.
We investigated demographic parameters including age, sex, body mass index (BMI), and risk factors for renal impairment (hypertension, diabetes). Tumor characteristics (size, laterality, location, clinical T stage, and R.E.N.A.L. [R = radius, E = exophytic vs. endophytic, N = nearness of tumor to collecting system, A = anterior or posterior, L = location relative to polar lines] nephrometry score) were evaluated via CT scan. Serum creatinine levels were measured before and after surgery for all patients. Estimated glomerular filtration rates (eGFRs) were calculated using the Chronic Kidney Disease Epidemiology Collaboration formula for preoperative, 1 month, and 6 months postoperatively.12 Propensity score matching was done with age, sex, BMI, tumor size, clinical T stage, R.E.N.A.L. score, and preoperative renal function. After matching, we analyzed clinical data of 134 patients who underwent OPN (n = 67) or RAPN (n = 67).
The following variables were compared between OPN and RAPN groups: surgical parameters (operation time, ischemic time, estimated blood loss [EBL], transfusion, length of hospital stay, pain visual analog score [VAS] at 1 day postoperatively, and complications of Clavien grade III or higher) and pathologic outcomes (tumor cell types, pathologic T stage, Fuhrman nuclear grade, and resection margin). Renal function outcome was assessed based on change in eGFR (eGFRpostoperative–eGFRpreoperative).
Data analysis
Independent t-test and χ2 test were performed to compare demographics, surgical parameters, and functional outcomes between OPN and RAPN groups. Kaplan-Meier analyses were conducted to compare recurrence-free survival and cancer-specific survival between the two groups. All P values were estimated. P < 0.05 was considered statistically significant. All statistical analyses were conducted using statistical software SPSS ver. 20.0 (IBM, Armonk, NY, USA).
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Seoul National University Bundang Hospital (protocol number: B-1710-427-111). This study was based only on retrospective analysis of clinical records of patients, and there was minimal risk to patients during the study. Therefore, this study was exempted from obtaining informed consent after IRB review.
Go to :
RESULTS
After propensity score matching, clinical data of 134 patients with renal tumor ≥ 4.0 cm who underwent OPN (n = 67) or RAPN (n = 67) were finally analyzed. Table 1 compares demographic data. Mean age, sex, BMI, and the incidence of hypertension or diabetes mellitus were similar between OPN and RAPN groups (all P > 0.05). Differences in tumor characteristics such as tumor size, laterality, location, clinical T stage, and R.E.N.A.L. nephrometry score were also statistically insignificant between the two groups (all P > 0.05).
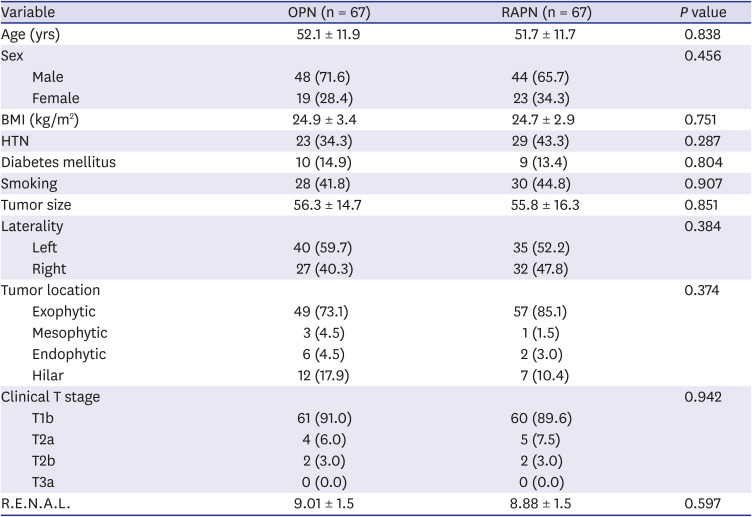
Table 1
Demographics of patients who underwent OPN or RAPN
Continuous variables are shown as mean ± standard deviation and categorical variables are shown as number (%).
OPN = open partial nephrectomy, RAPN = robot-assisted partial nephrectomy, BMI = body mass index, HTN = hypertension.
![]()
Table 2 presents comparative data of perioperative parameters. The RAPN group had significantly longer operation time (149.0 ± 47.1 minutes vs. 173.3 ± 77.8 minutes, P = 0.030) and longer ischemic time (20.3 ± 8.2 minutes vs. 29.4 ± 8.5 minutes, P = 0.001), but shorter hospital stay (8.2 ± 1.8 days vs. 6.0 ± 1.8 days, P = 0.001) than the OPN group. Mean EBL was 271.7 mL for the OPN group and 198.7 mL for the RAPN, showing no significant (P = 0.053) difference between the two groups. There was no significant difference in mean VAS at 1 day postoperatively between the two groups (4.5 ± 1.0 for OPN group versus 4.3 ± 0.9 for RAPN group, P = 0.194). There was no radical conversion in either group. Five patients in each group received blood transfusions. Grade III or higher complications occurred in 4 (6.0%) patients in the OPN group and 2 (3.0%) patients in the RAPN group (P = 0.403).
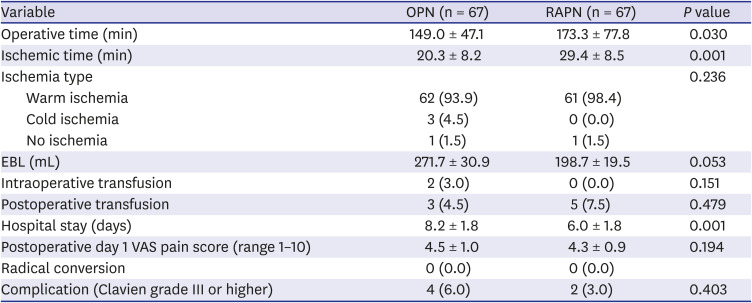
Table 2
Perioperative outcomes of patients in OPN or RAPN group
Continuous variables are shown as mean standard ± deviation and categorical variables are shown as number (%).
OPN = open partial nephrectomy, RAPN = robot-assisted partial nephrectomy, EBL = estimated blood loss, VAS = visual analog scale.
![]()
Table 3 shows pathologic outcomes in OPN and RAPN groups. There was no significant difference in tumor cell type (P = 0.672) or pathologic T stage (P = 0.798) between the two groups. There was no positive surgical margin (PSM) in either group. Mean safety margin was 1.8 mm for the OPN group and 2.4 mm for the RAPN groups, showing no significant (P = 0.090) difference between the two groups.
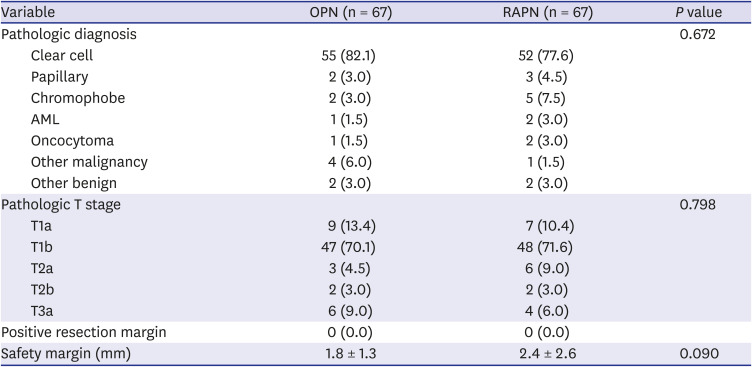
Table 3
Pathologic outcomes of patients in OPN or RAPN group
Continuous variables are shown as mean ± standard deviation and categorical variables are shown as number (%).
OPN = open partial nephrectomy, RAPN = robot-assisted partial nephrectomy, AML = angiomyolipoma.
![]()
Table 4 summarizes baseline and follow-up eGFRs in OPN and RAPN groups. Mean preoperative eGFR was similar in both groups (88.6 ± 20.2 mL/min/1.73 m2 for OPN group vs. 91.2 ± 20.1 mL/min/1.73 m2 for RAPN group, P = 0.444). No statistically significant difference was noted in mean change of 1-month eGFR (−8.4 ± 11.7 mL/min/1.73m2 for OPN group vs. −7.5 ± 10.8 mL/min/1.73m2 for RAPN group, P = 0.638) between the two groups. However, mean change of 6-month eGFR was significantly better for the RAPN group than for the OPN group (−8.2 ± 11.8 mL/min/1.73m2 vs. −3.1 ± 10.7 mL/min/1.73m2, P = 0.027).

Table 4
Baseline and follow-up eGFR calculated by the Chronic Kidney Disease Epidemiology Collaboration formula
Continuous variables are shown as mean ± standard deviation and categorical variables are shown as number (%).
eGFR = estimated glomerular filtration rate; OPN = open partial nephrectomy, RAPN = robot-assisted partial nephrectomy.
![]()
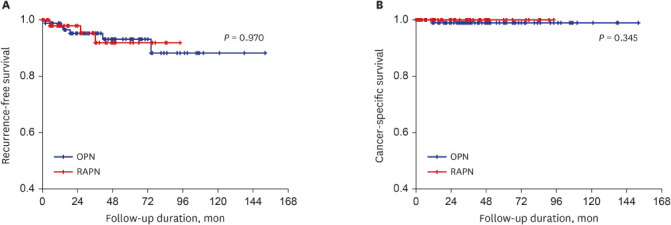
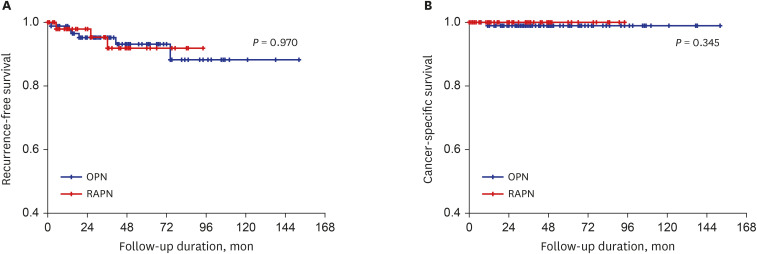
Kaplan-Meier analyses showed no statistical difference in recurrence-free survival (P = 0.970) or cancer-specific survival (P = 0.345) between OPN and RAPN groups (Fig. 1). Five-year recurrence-free survival rate was 94.6% for the OPN group and 98.4% for the RAPN group. Five-year cancer-specific survival rate was 98.4% for the OPN group and 100% for the RAPN group.
Go to :
DISCUSSION
NSS is the gold standard treatment for renal tumors less than 4 cm because of its comparable oncological survival with excellent renal function preservation to radical nephrectomy.12 A previous study has evaluated the impact of tumor size on tumor recurrence and patient survival following NSS and found that cancer-free survival is significantly worse in patients with tumors 4 cm or more than that in those with smaller tumors.13 Different from these results, a comparative study has reported no statistical difference in disease-free survival rate between NSS and radical nephrectomy for renal cell carcinoma (RCC) up to 7 cm in size.14 Accumulating evidence supports that NSS can provide oncological results similar to radical nephrectomy for renal tumors with size of 4 cm or more.34567 One study has compared outcomes of NSS for small (≤ 4 cm) and large (> 4 cm) RCC and found that 5-year and 10-year recurrence-free survival rates are comparable for small and large tumors.15 The authors recommended that the criteria for selecting NSS rather than radical nephrectomy are safety and surgical resectability rather than tumor size.15 A comparative study has reported that patients treated with partial nephrectomy in T2 N0 M0 tumors have better overall survival than those treated with radical nephrectomy, although they have more PSM.16 Overall survival is correlated with age, comorbidity index, histologic subtype, and Fuhrman grade.16 Therefore, indications for NSS are currently expanding into larger and more advanced renal tumors if technically possible.8 In the present comparative study of the management of renal tumors larger than 4 cm, patients who underwent RAPN and those who underwent OPN had comparable recurrence-free survival (P = 0.970) and cancer-specific survival (P = 0.345).
Over the past two decades, LPN and RAPN have been accepted as minimally invasive surgical techniques for NSS. However, the role of LPN is currently quite limited due to its steep learning curve, although it has been proven to be able to provide less postoperative pain, faster convalescence, shorter hospitalization lengths, and better cosmetic results than OPN.17 RAPN incorporates the superior dexterity and three-dimensional optics of OPN and the high-definition of LPN with tremor filtration and an ergonomic design.1819 RAPN overcomes technical difficulties of LPN. Surgical parameters of RAPN appear to be less affected by tumor complexity than LPN.10 There have been several systematic reviews and meta-analysis comparing perioperative results of OPN and RAPN.2021 However, these studies did not analyze renal tumors larger than 4 cm only. Our study was meaningful because surgical parameters, functional outcomes, and oncological outcomes between RAPN and OPN for renal tumors larger than 4 cm were compared after propensity score matching. The RAPN group had a longer operation time and a longer ischemic time, but a shorter hospital stay. No significant difference was found for other surgical parameters such as EBL, mean VAS at 1 day postoperatively, margin status, radical conversion, transfusion rate, or postoperative complications (Clavien grade ≥ III) between the two groups.
Partial nephrectomy is superior to radical nephrectomy in the preservation of renal function. However, renal function is inevitably deteriorated after partial nephrectomy.2 During partial nephrectomy, temporary clamping of ipsilateral renal hilum enables better visualization for tumor resection and parenchymal reconstruction, while long-term ischemia will result in irreversible kidney damage.22 Based on results of previous studies, it is now established that a shorter duration of ischemic time is important for preserving the quality and function of nephrons remaining after partial nephrectomy, thus optimizing postoperative renal function.23 Our analysis showed that the RAPN group had significantly longer ischemic time than the OPN group. However, mean change of 1-month eGFR did not differ significantly between the two groups, although mean change in 6-month eGFR was better for the RAPN group than that for the OPN group. In a comparative study of postoperative renal function by using Tc-99m diethylenetriaminepentaacetic acid renal scintigraphy, postoperative renal function impairment was similar between patients who underwent OPN and those who underwent RAPN despite the long ischemic time of RAPN.24 One study has performed trend analysis for eGFR changes after OPN and found that 1-year eGFR has a steeper decrease when ischemic time exceeds 40 minutes.2 In our study, the mean ischemic time was within 30 minutes for both groups. It has been reported that preserving more residual parenchymal tissue during partial nephrectomy is more important than reducing ischemic time in terms of renal function recovery.25 Simmons et al.26 have reported that parenchymal atrophy is minimal after partial nephrectomy when ischemic time is less than 40 minutes and that the reduction in renal function observed soon after partial nephrectomy can gradually recover. These findings suggest that kidney volume reduction after partial nephrectomy is predominantly associated with resection. Unfortunately, we were unable to obtain residual parenchymal volume data. However, we calculated resected specimen volume and non-neoplastic parenchymal volume and found that they were similar between the two groups (data not shown). Compensation by the remaining contralateral kidney might have an effect on these functional outcomes in this study. In addition to ischemic time, various factors might have affected renal function recovery after partial nephrectomy.
The present study has some shortcomings. First, the design of this study was retrospective and non-randomized. It had a relatively short follow-up period, making it difficult to assess long-term outcomes in patients who underwent RAPN, especially those with large renal tumors. Another limitation was the possibility of selection bias as the surgeon's choice of technique might have been influenced by the complexity of renal tumors. However, no significant difference was found in R.E.N.A.L. score between the two groups. To measure renal functions, we used eGFR instead of measured GFR or renal scintigraphy. To confirm our findings, randomized and prospective studies with large sample sizes and long follow-up periods are needed.
In conclusion, RAPN is a safe and feasible surgical modality comparable to OPN for managing renal tumors larger than 4 cm in terms of surgical, functional, and oncological outcomes. NSS is still challenging in the management of large renal tumors. However, the use of RAPN as a minimally invasive modality is expanding. Further prospective randomized studies are needed to determine the feasibility of OPN and RAPN for large-sized renal tumors.
Go to :
 XML Download
XML Download