

 PDF
PDF Citation
Citation Print
Print



A 42-year-old woman, who underwent aortic valve (AV) replacement with a 21 mm On-X valve and graft replacement of ascending aorta six months ago, visited out-patient clinic for a routine checkup. Her postoperative pre-discharge echocardiogram at six months ago showed normal left ventricular systolic function and normal reference range of the pressure gradient (PG) across the mechanical AV (peak/mean PG 20/11 mmHg) (Figure 1A). She had maintained sinus rhythm without systemic diseases or a history of taking oral contraceptives. During taking warfarin, international normalized ratio (INR) was checked every month, and maintained at 2.0–2.5. On routine follow-up echocardiography 6 months after surgery, the AV PG was slightly elevated to 29/17 mmHg and the acceleration time on the continuous wave Doppler was prolonged to 90 msec. Peak AV velocity was 2.7 m/sec (Figure 1B). On the same day, cardiac computed tomography (CT) was performed to evaluate the graft of the ascending aorta without suspicion of prosthetic valve abnormalities. Unexpectedly, a rounded low-attenuated structure on the right side of the mechanical AV was found (Figure 1D-F, Supplementary Video 1). After five days of intravenous unfractionated heparin therapy, the low attenuated structure disappeared on follow-up CT, and PG and acceleration time were normalized (Figure 1C, G, and I, Supplementary Video 2). Currently, she is taking aspirin once daily and warfarin (INR 2.5–3.0) without signs of systemic embolism. This case displays the role of cardiac CT in detecting subclinical prosthetic valve thrombosis,1)2)3) when the Doppler findings are out of the reference range but not diagnostic.
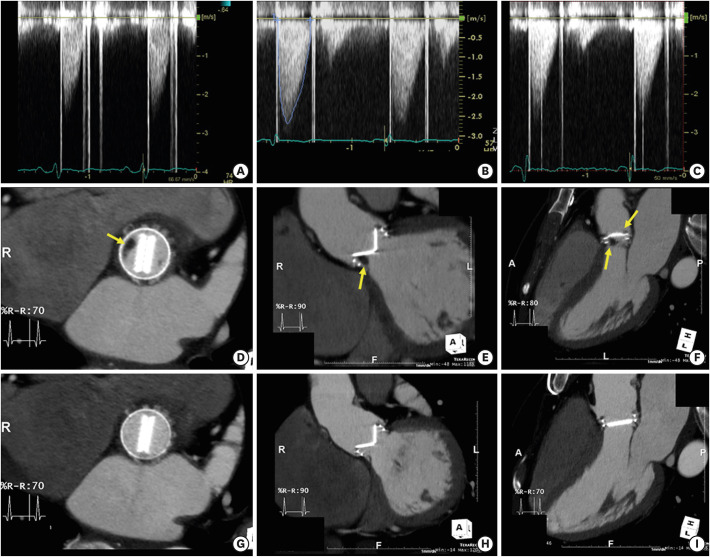 | Figure 1Echocardiography and cardiac computed tomography of subclinical mechanical valve thrombosis. (A) Continuous-wave Doppler of the mechanical aortic valve on postoperative pre-discharge echocardiogram. (B) Continuous-wave Doppler of the mechanical aortic valve on 6-month follow-up echocardiogram. (C) Continuous-wave Doppler of the mechanical aortic valve after intravenous unfractionated heparin therapy for 5 days. (D-F) Low attenuating mass lesions on the right side of the mechanical aortic valve on 6-month follow-up CT. (G-I) Resolution of mass lesions on the right side of the mechanical aortic valve on the follow-up CT after intravenous unfractionated heparin therapy for 5 days.CT = computed tomography.
|

 XML Download
XML Download