

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Sodium-glucose co-transporter (SGLT) is a membrane protein that supplies sodium ions
(Na+) and glucose like as glucose transporter. In human, there are 6 types of
SGLT and, among which SGLT1 and SGLT2 are known to be involved in glucose resorption in the
intestinal mucosa (mainly for SGLT1) or proximal tubule of the renal nephron (mainly for
SGLT2).1) SGLT1 is mainly located in the small
intestine and plays an important role in the absorption of galactose, in addition to
glucose. SGLT2 is primarily distributed in the kidney and is responsible for 90% of renal
glucose resorption.2) Under physiological conditions,
180 g of glucose are filtered and completely reabsorbed by the renal tubules. In diabetic
patients, glucose can be found in the urine when hyperglycemia.3) Whereas SGLT1 transports 2 Na+ per one molecule of glucose
and SGLT2 transports 1 Na+, SGLT2 can co-localize with the renal
Na+/hydrogen exchanger (NHE3), responsible for Na+ reabsorption in the
proximal tubule.4) SGLT2 inhibitors (SGLT2i) may
cross-react with this NHE3 so inhibit Na+ reabsorption and increase
natriuresis.
In general, the glucose-lowering ability of SGLT2i through urinary glucose excretion can
decrease hemoglobin A1c modestly (from 0.5% to 1.0%) in patients with diabetes. The
glucosuric effect of SGLT2i depends on the blood glucose concentration. So hypoglycemia risk
following SGLT2i use is low compared to other glucose-lowering drugs.
Patients with type 2 diabetes mellitus (T2DM) are at high risk of heart failure (HF), about
20–30% found in diabetes clinical practice and had higher rates of heart failure
hospitalization (HFH) with higher mortality.5) SGLT2i
exert consistent favorable effects on the HFH across all trials.6) However, these drugs have inconsistent results on mortality. Depending
on the trial, empagliflozin reduced the risk of cardiovascular (CV) death by 38% but by only
2% in the trial with dapagliflozin in T2DM.7)8)
Not only are patients with T2DM at higher risk for HF, patients with HF are also at high
risk for recurrent HFH, high CV mortality, and worsening of renal function with poor quality
of life. The combined risk of HFH or CV death in patients with heart failure with reduced
ejection fraction (HFrEF), was reduced by 25% with dapagliflozin or empagliflozin, mainly
driven by a reduction of HFH.9)10)
These benefits of SGLT2i relatively on short-term follow-up cannot be explained by their
glucose–lowering effects. Therefore, it is important to find out the crucial
mechanism of SGLT2i by carrying out large-scale trials in patients with various phenotype of
T2DM and well-characterized HF who are on guideline-directed medical therapy including the
device therapy.
Go to : 
BENEFITS ON HEART FAILURE EVENTS IN PATIENTS WITH TYPE 2 DIABETES MELLITUS
SGLT2i have demonstrated unanticipated cardiorenal benefits in several large randomized
clinical trials of patients who have T2DM and either established atherosclerotic
cardiovascular disease (ASCVD) or multiple CV risk factors. The effect of SGLT2i on
non-fatal HF events or CV death is summarized in 5 cardiovascular outcome trials (CVOT) with
5 different agents in T2DM, respectively (Table
1).
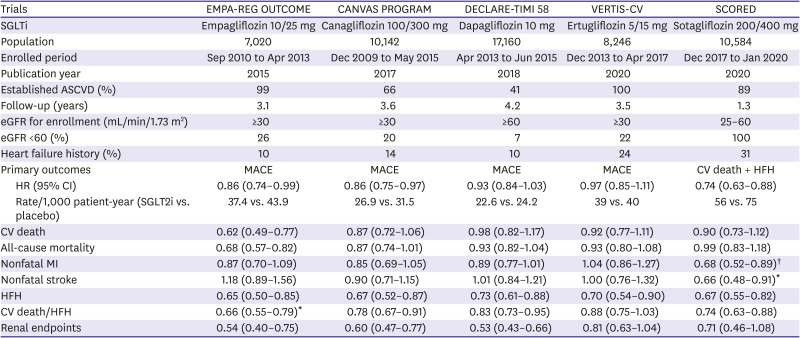
Table 1
Key characteristics of cardiovascular outcome trials for SGLT2i in type 2 diabetes mellitus
ASCVD = atherosclerotic cardiovascular disease; CI = confidence interval; CV =
cardiovascular; eGFR = estimated glomerular filtration rate; HFH = heart failure
hospitalization; HR = hazard ratio; MACE = major adverse cardiac events; MI = myocardial
infarction; SGLT = sodium-glucose co-transporter; SGLTi = sodium-glucose co-transporter
inhibitors; SGLT2i = sodium-glucose co-transporter 2 inhibitors.
*Excluding fatal stroke. †Total fatal or nonfatal
MI/stroke.
![]()
The first SGLT2i with the COVT result was empagliflozin through the EMPA-REG OUTCOME
trial.7) The study enrolled 7,020 T2DM patients with
established ASCVD such as coronary and peripheral artery disease, and followed up for 3.1
years. This trial showed a significant 14% reduction in the primary composite outcome (major
adverse cardiac events) including CV death, nonfatal myocardial infarction (MI), and
nonfatal stroke (hazard ratio [HR], 0.86; 95% confidence interval [CI], 0.74–0.99,
p=0.04 for superiority). This clinical benefit was primarily driven by a 38% reduction of CV
death (HR, 0.62; 95% CI, 0.49–0.77). The clinical effect of empagliflozin on nonfatal
MI or stroke was neutral, so the CV mortality reduction by empagliflozin seems to be largely
related to the HFH reduction (HR, 0.65; 95% CI, 0.50–0.85). Interestingly, these
benefits on CV mortality and HFH was found early after empagliflozin treatment initiation
(within 12 weeks after randomization).11) Following
this unanticipated finding, many researchers have paid attention to the direct myocardial
protective effect of SGLT2i. More detailed explanation for mechanism of cardiorenal effects
of SGLT2i was reviewed well in recent publication.3)12)
After empagliflozin became the first drug to show beneficial effects in T2DM patients with
high CV risk, the CVOT of additional SGLT2i followed and confirmed the benefit of SGLT2i.
The CANVAS program using canagliflozin enrolled 10,142 diabetic patients with and without
established ASCVD (positive for multiple risk factors), and followed up for 3.6 years.13) This trial demonstrated a significant 14% reduction
in the primary composite outcome including CV death, nonfatal MI, and nonfatal stroke (HR,
0.86; 95% CI, 0.75–0.97, p=0.02 for superiority). The clinical effect of
canagliflozin on each separate primary outcome was all neutral, and only HFH was
significantly reduced by canagliflozin (HR, 0.67; 95% CI, 0.52–0.87). In addition,
canagliflozin reduced the composite of HFH or CV death by 22% (HR, 0.78; 95% CI,
0.67–0.91).
The DECLARE-TIMI 58 trial using dapagliflozin enrolled 17,160 diabetic patients with and
without established ASCVD, and followed up for 4.2 years.8) This trial failed to show a significant reduction in the primary composite
outcome including CV death, nonfatal MI, and nonfatal stroke (HR, 0.93; 95% CI,
0.84–1.03; p=0.17). The clinical effect of canagliflozin on each separate primary
outcome was all neutral, and only HFH was significantly reduced by dapagliflozin (HR, 0.73;
95% CI, 0.61–0.88). Like canagliflozin, dapagliflozin also reduced the composite of
HFH or CV death by 17% (HR, 0.83; 95% CI, 0.75–0.95). However, in comparison with 38%
reduction of CV death in the CVOT using empagliflozin, but only 2% was noted in the trial
with dapagliflozin.
The VERTIS CV trial using ertugliflozin enrolled 8,246 diabetic patients with established
ASCVD, and followed up for 3.5 years.14) The trial
also failed to show a significant reduction in the primary composite outcome including CV
death, nonfatal MI, and nonfatal stroke (HR, 0.97; 95% CI, 0.85–1.11). The clinical
effect of ertugliflozin on each separate primary outcome was all neutral, and only HFH event
was significantly reduced by ertugliflozin (HR, 0.70; 95% CI, 0.54–0.90). However,
the benefit on the composite of HFH or CV death was not nominally significant with
ertugliflozin (HR, 0.88; 95% CI, 0.75–1.03).
The latest SGLT2i to report CVOT is sotagliflozin in the SCORED trial.15) The study enrolled 10,584 type 2 diabetes, chronic kidney disease
patients with and without established ASCVD, and followed up for 1.3 years because of early
termination owing to loss of funding. The primary end point was changed to the composite of
the total number of CV death, HFH, and urgent visits for HF during the trial. This trial
demonstrated a significant 26% reduction in the primary composite (HR, 0.74; 95% CI,
0.63–0.88). This clinical benefit of ertugliflozin was primarily driven by a 33%
reduction of total number of HFH and urgent visits for HF (HR, 0.67; 95% CI,
0.55–0.82) but the CV mortality reduction by sotagliflozin was neutral (HR, 0.90; 95%
CI, 0.73–1.12).
Although these CVOTs seem to be similar, we could find some discrepancies in the baseline
characteristics among these trials. Firstly, regarding the inclusion criteria, the trials
using empagliflozin, ertugliflozin enrolled 100% established ASCVD, focusing on only the
secondary prevention. Whereas, the CVOT using canagliflozin, dapagliflozin enrolled diabetic
patients with and without ASCVD, focusing on both the primary and secondary prevention. We
could expect higher chance for statistical significance in secondary prevention trial rather
than in primary prevention trial considering higher event rates in secondary prevention
trials. This hypothesis may explain the neutral clinical benefit of dapagliflozin on primary
composite outcome. Secondly, there were 2 phases of enrollment period such as early 2010s
(for empagliflozin, canagliflozin) vs. mid 2010s (for dapagliflozin, ertugliflozin). In
general, the clinical trials which conducted in relatively late phase, could have lower
chance for statistical significance than those in early phase. The limited clinical benefit
of ertugliflozin could be resulted from these discrepancies among CVOTs or structure
difference among SGLT2i.16) However, all SGLT2i
including sotagliflozin, were proved to significantly reduce the risk of HFH in T2DM
patients, which confirmed by meta-analysis.17)
In these trials with T2DM patients, lack of information regarding the phenotype of HF or
use of concomitant guideline directed medical treatment of HF give us a skeptical
interpretation about the significant reduction of risk in HFH. Because the results of these
CVOT could be affected by the use of inhibitors of renin-angiotensin system and
beta-blockers, mineralocorticoid receptor antagonists or angiotensin receptor-neprilysin
inhibitor (ARNI) which showing the survival benefit in HFrEF patients. From the data of
EMPA-REG OUTCOME, concomitant use of spironolactone and eplerenone may attenuate the effect
of SGLT2i to reduce HF events.18) In addition, it is
not clear whether SGLT2i might interact with ARNI.
However, based on these lines of evidences, 2019 European Society of Cardiology guidelines
on diabetes, pre-diabetes, and CV diseases recommended SGLT2i (empagliflozin, canagliflozin,
and dapagliflozin) to lower the risk of HFH in patients with T2DM as class I recommendation
with level of evidence A.19)
Go to :
BENEFITS ON HEART FAILURE EVENTS IN PATIENTS WITH HEART FAILURE WITH REDUCED EJECTION FRACTION
The reduction of the risk of HFH with SGLT2i in patients with T2DM have been demonstrated
in all CVOT. This reduction for HFH risk was observed in both patients with and without a
previous HF history. However, patients with HF history comprised only small proportions of
the COVT populations, especially without documentation for left ventricular ejection
fraction (LVEF) or natriuretic peptide levels. These effects of SGLT2i on CV outcomes may
not be directly related to glycemic control, suggesting that these clinical benefits may
extend to non-diabetic patients, especially HF. In addition, the DECLARE-TIMI 58 trial
showed that the benefit of CV death or HFH was greater in patients with HFrEF than with
HFpEF. Especially, the benefit was remarkable in those with LVEF ≤30%.20) Therefore, the effect of SGLT2i in patients with HF,
especially HFrEF was explored in large-scale trials.
The DAPA-HF trial was the first outcome trial to assess the effect of SGLT2i (using
dapagliflozin) in HFrEF patients with or without diabetes.9) The definition of HFrEF was LVEF <40% and elevated N-terminal-pro B-type
natriuretic peptide (NT-proBNP) level. The trial enrolled 4,744 patients including 2,607
non-DM patients and followed up for 18.2 months. The primary end point was the composite
outcome of CV death, HF, and urgent HF-related hospital visits. This trial demonstrated a
significant 26% reduction in the primary composite outcome (HR, 0.74; 95% CI,
0.65–0.85). This clinical benefit of dapagliflozin was primarily driven by a 30%
reduction of HFH and urgent visits for HF (HR, 0.70; 95% CI, 0.58–0.85) but
surprisingly, the CV mortality was also significantly reduced with dapagliflozin (HR, 0.82;
95% CI, 0.69–0.98). Although this trial was conducted in non-diabetic patients with
HFrEF, the frequency of adverse events such as volume depletion, renal dysfunction, and
hypoglycemia did not differ between dapagliflozin and placebo group.
The EMPEROR-Reduced trial was the following outcome trial to assess the effect of another
SGLT2i, empagliflozin in HFrEF patients with or without diabetes.10) The trial enrolled 3,730 patients including 1,856 non-DM patients and
followed up for 16 months. The primary end point was the composite outcome of CV death and
HFH. This trial demonstrated a significant 25% reduction in the primary composite outcome
(HR, 0.75; 95% CI, 0.65–0.86). This clinical benefit of empagliflozin was primarily
driven by a 30% reduction of HFH and urgent visits for HF (HR, 0.69; 95% CI,
0.59–0.81) but the CV mortality reduction by empagliflozin was neutral (HR, 0.92; 95%
CI, 0.75–1.12). In comparison with DAPA-HF trial, EMPEROR-Reduced trial enrolled
patients with higher CV risk factors, for example, lower ejection fraction (27% vs. 31%),
high level of NT-proBNP (1,900 vs. 1,437 pg/mL) and lower estimated glomerular filtration
rates (eGFRs) (62 vs. 66 mL/min/m2).21)
Interestingly, the annual rate of decline in eGFR was significantly slower in the
empagliflozin group than placebo (−0.55 vs. −2.28 mL/min/1.73
m2/year).10) In addition, exploratory
composite renal endpoint defined as chronic dialysis, renal transplantation, or the onset of
a sustained and profound decrease in renal function was significantly reduced by 50% with
empagliflozin (HR, 0.50; 95% CI, 0.32–0.77). However, in DAPA-HF trial, a composite
of renal events was reduced by 29%, which is not nominally significant (HR, 0.71; 95% CI,
0.44–1.26). In contrast, DAPA-HF trial reported a lower risk of CV death with a 18%
risk reduction, which is nominally significant and a 8% risk reduction in the
EMPEROR-Reduced trial, which is not. This discrepancy might be difficult in the
interpretation and conclusion due to heterogeneity of patients’ clinical
characteristics and short-term follow up duration, and so on.
The SOLOIST-WHF was the latest outcome trial to assess the effect of SGLT2i, sotagliflozin
in HFrEF patients with diabetes who were recently hospitalized for worsening HF.22) The trial enrolled 1,222 patients and followed up for
just 9 months because the trial ended early owing to loss of funding from the sponsor. The
primary end point was the composite outcome of CV death, HFH and urgent visits for HF. This
trial demonstrated a significant 33% reduction in the primary composite outcome (HR, 0.67;
95% CI, 0.52–0.85). This clinical benefit of sotagliflozin was also driven by a 30%
reduction of HFH and urgent visits for HF (HR, 0.64; 95% CI, 0.49–0.83) but the CV
mortality reduction by sotagliflozin was neutral, too (HR, 0.84; 95% CI, 0.58–1.22).
However, due to the smaller-sized sample enrolled and shorter follow-up period (only 9
months) than planned, the SOLOIST-WHF trial did not have enough to provide a statistically
robust assessment for the effect of sotagliflozin on CV mortality. Regarding adverse events,
severe hypoglycemia (1.5% vs. 0.3%) and diarrhea (6.1% vs. 3.4%) were more common with
sotagliflozin group than placebo. Especially, a difference in diarrhea event was not
reported in the DAPA-HF or EMPEROR-Reduced trial so we could assume that it is related to
SGLT1 inhibition in the intestines considering higher affinity for inhibiting SGLT1 by
sotagliflozin than dapagliflozin and empagliflozin.21)
Unanticipated success in the SOLOIST-WHF trial may open more questions than answer
regarding the role of SGLT1 inhibition in HF. Is a sotagliflozin better for HF than other
SGLT2i? Is the big success of sotagliflozin mediated by higher SGLT1 inhibition than
dapagliflozin and empagliflozin? Is there any therapeutic role of SGLT1 inhibition in
intestines in HF, reflected by increased diarrhea in sotagliflozin group? Any role for
helping decongestion of third space or lymphatics? When we consider the SGLT1 expression in
heart is the second highest after small intestine and SGLT1 is highly expressed in human
cardiomyocytes, we can guess whether there is any other role of SGLT1 in heart just than
glucose transport. Further translational research should be warranted to answer these
questions.
Comparing the baseline characteristics of 3 trials of SGLT2i in patients with HFrEF (Table 2), the DAPA-HF populations had higher eGFR, lower
NT-proBNP level and lower use for ARNI, implantable cardioverter defibrillation, cardiac
resynchronization therapy than those from EMPEROR-Reduced and SOLOIST-WHF. The discrepancy
in these baseline risk factors may be related to lower event rates, especially HFH events in
DAPA-HF trial.
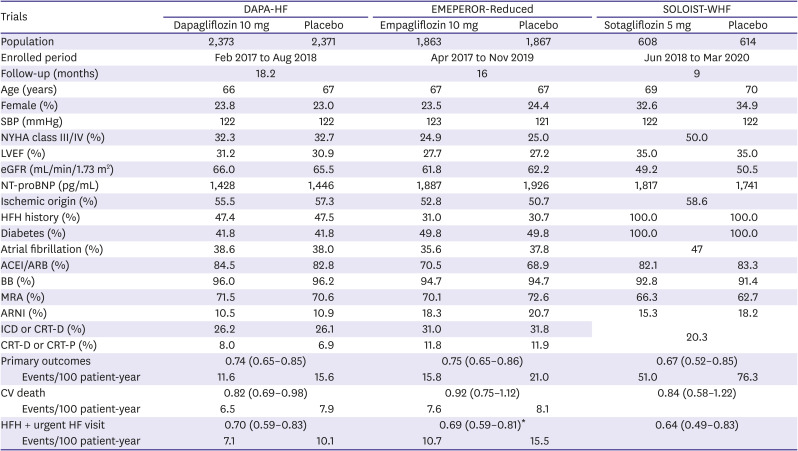
Table 2
Key characteristics of trials for SGLT2i in heart failure with reduced ejection fraction
ACEI/ARB = angiotensin converting enzyme inhibitor/angiotensin receptor blocker; ARNI =
angiotensin receptor-neprilysin inhibitor; BB = beta-blocker; CRT = cardiac
resynchronization therapy; eGFR = estimated glomerular filtration rate; HF = heart
failure; HFH = heart failure hospitalization; ICD = implantable cardioverter
defibrillation; LVEF = left ventricular ejection fraction; MRA = mineral-corticoid
receptor antagonist; NT-proBNP = N-terminal-pro B-type natriuretic peptide; NYHA = New
York Heart Association; SBP = systolic blood pressure; SGLT2i = sodium-glucose
co-transporter 2 inhibitors.
*Excluding urgent HF visit.
![]()
Combining these 3 HFrEF trials together, recently published meta-analysis showed that
SGLT2i could reduce CV death or first HFH (HR, 0.74; 95% CI, 0.68–0.81), CV death and
total HFH (HR, 0.74; 95% CI, 0.67–0.82), CV death (HR, 0.86; 95% CI,
0.76–0.97) and all-cause mortality (HR, 0.86; 95% CI, 0.77–0.96) in HFrEF
patients.21) Following these lines of clinical
evidences, we can expect future HF guidelines may strongly recommend SGLT2i for HFrEF
patients with or without diabetes.6) It seems to be
time for triple therapy to evolve to quadruple therapy including beta-blockers, ARNI,
mineralocorticoid receptor antagonists, and SGLT2i in HFrEF.23)24) Recent comparative analysis of 3
randomized controlled trials including EMPHASIS-HF (eplerenone), PARADIGM-HF
(sacubitril-valsartan, ARNI) and DAPA-HF (dapagliflozin), supported this quadruple therapy
as a new standard for HFrEF treatment.25)
Go to :
EFFECTS ON HEAT FAILURE EVENTS IN PATIENTS WITH HEAT FAILURE WITH PRESERVED EJECTION FRACTION
Since 2010, there has not been a drug that can reduce clinical events in patients with
HFpEF.26)27)
In January 2021, the US Food and Drug Administration (FDA) expanded indication to
sacubitril-valsartan (ARNI) that would allow for use of the therapy in at least some
patients with HFpEF, based on the results from the PARAGON-HF trial.28) The new FDA label includes the following note: “Benefits are
most clearly evident in patients with LVEF below normal.”, which supported by further
analysis of PARAGON-HF.29)30) Following the first drug for HFpEF, more attention have been paid to
SGLT2i, a next nominee for HFpEF drug. An important uncovered question is whether the
observed clinical benefits of SGLT2i is present in HFpEF patients like in T2DM or HFrEF
patients. Until now, there have been limited data for SGLT2i in HFpEF. In each of the CVOT,
approximately 10–15% of patients had a HF history,31) but the definition for HFrEF or HFpEF and documentation for LVEF were poor in
CVOT and real-world evidence.32)33)34)
In a post hoc analysis of SOLOIST-WHF, the key subgroup of interest was LVEF <50% vs.
≥50%, which showed a consistent clinical benefit with that in the main results of the
trial. Sotagliflozin therapy reduced primary composite outcome in both LVEF <50% (HR,
0.72; 95% CI, 0.56–0.94) and LVEF ≥50% (HR, 0.48; 95% CI, 0.27–0.86)
groups.22) This result could hint at efficacy of
SGLT2i in HFpEF similar to that in HFrEF, even though the number of patients with a LVEF
≥50% (n=256) was modest. In a further subgroup analysis regarding LVEF, the HR for
the primary composite outcome was 0.69 (95% CI, 0.51–0.92) in patients with a LVEF
<40% (n=725) and 0.68 (95% CI, 0.45–1.03) in patients with a LVEF ≥40%
(n=494).21)
There are 2 ongoing trials which designed to investigate the clinical effect of SGLT2i in
HFpEF patients. The EMPEROR-Preserved trial enrolled 4,126 HFpEF patients to empagliflozin
or placebo (NCT03057951),35)36) and the DELIVER trial enrolled 4,700 patients to dapagliflozin or
placebo (NCT01297257); both clinical trials are expected to be completed and reported
in 2021–2022.
Go to :
CONCLUSION
SGLT2i have been emerged as a powerful therapeutic option to reduce the risk of HF and HFH
in patients with T2DM, and to reduce CV mortality and HFH in HFrEF patients with or without
T2DM. These favorable benefits of SGLT2i could be attained by taking once daily without
up-titration like renin-angiotensin system blockers or beta-blockers. In addition, the risk
of hypotension, hyperkalemia, or worsening of renal function, which concerns that often
accompany the use of HF medication is relatively low with low risk of other safety issues
such as bone fracture, low extremity limb ischemia, and diarrhea. Ongoing study to evaluate
the clinical effect of SGLTi for HFpEF may further widen the clinical implication of these
novel cardiorenal protective drugs beyond their metabolic effects. Further translational or
reverse translational studies should be warranted to elucidate the pharmacological
mechanisms of SGLT2i on protection for heart, kidney and human being.
Go to :
 XML Download
XML Download