

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cardiovascular diseases (CVDs), primarily ischaemic heart disease and stroke, are the first and second leading causes of death worldwide, causing an estimated 16% and 11% of total global mortality respectively, or approximately 9 million total deaths.1)
CVD, which include ischaemic heart disease and stroke, collectively account for 23.4% of total deaths in South Korea.2) A rapidly aging population, accompanied by the increasing in the prevalence of lifestyle risk factors in South Korea has given rise to the growing burden of CVD, with escalating healthcare and socioeconomic costs.3)
Reducing the major risk factors for CVD is now a major strategy for reducing CVD prevalence. Therefore, risk factor reduction is now an established, effective global public health strategy, targeted at both for primary and secondary prevention of CVD. Deficiencies in primary prevention or pre-acute care, as well as secondary prevention/rehabilitation or post-acute care were recognized as the major underlying reasons for the South Korean “paradox” amongst Organization for Economic Co-operation and Development (OECD) countries.4) This “paradox”, where South Korea exhibited higher case-fatality rates for acute myocardial infarction (AMI) and stroke compared to OECD countries, despite excellent acute hospital care, was largely due in inadequate CVD risk factor prevention, sub-optimal emergency response systems, inadequate post-acute care, and marked disparities between rural and urban communities.4)
Governments across Europe, North America, and parts of Asia have embarked on the policies that utilize nationwide CVD registries which provided important data for the establishment of policies for improving the quality of cardiovascular care, patient outcomes, and health care costs. In this effort, we present evidence for the critical role of national registries in the South Korean context and recommend the need to expand regional cardio-cerebrovascular centers (CCVCs) and establishing new local CCVCs. Such efforts require a collective strategy involving public-private partnerships and the participation of academic and medical societies as well as national and local governments, including sustainable funding strategies.
TREND IN RISK FACTORS OF CARDIOVASCULAR DISEASE IN KOREA
Cigarette smoking
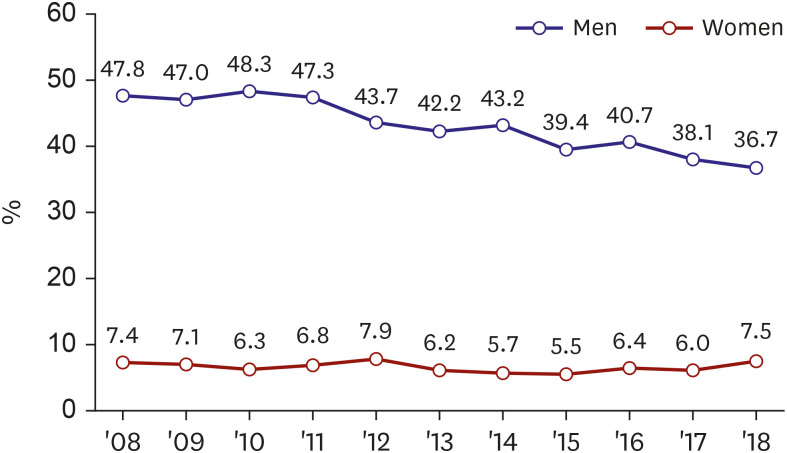
According to the World Health Organization 2019 report, globally, the number of males using tobacco, mainly cigarettes smoking, decreased for the first time since records had began. Government-led action played a significant role in this reduction, demonstrating the positive impact of such measures in preventing and reducing tobacco-related risks.5) Nevertheless, tobacco use remains a major global threat to public health, with more than 8 million annual deaths in the world.6) In South Korea, 41% of coronary artery diseases (CADs) and 26% of cerebrovascular disease are caused by tobacco, attributable to the high prevalence of smoking in adult Korean men.7)8) The smoking rate in adult Korean men declined rapidly from 79% in 1980 to 45% in 2007, but the rate of decline has slowed recently.9) According to the 2018 National Health and Nutrition Survey report, the smoking rate in adult men was 36.7%. Conversely, the smoking rate in adult women has increasing from 6.5% in 1998 and 7.5% in 2018 (Figure 1).10)
Figure 1
Trends in cigarette smoking in South Korea.
Source: Generated from Korea National Health and Nutrition Examination Survey, KCDC.10)
Diet & physical activity
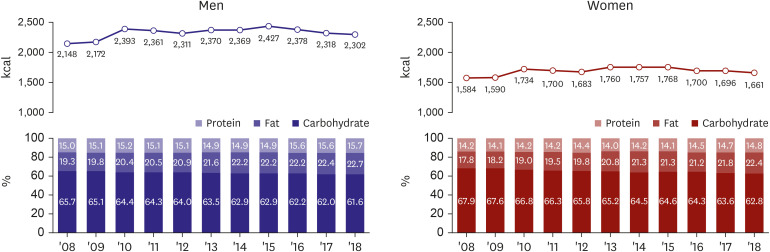
Industrialization and improved economic status led to an increase in total caloric intake per capita but reduced physical activity. Increased intake of saturated animal fats, trans-fats, and monosaccharides, with decreased intake of vegetables result in increased risks for CVD. According to the 2018 Korea National Health and Nutrition Examination Survey, total caloric and fat intake steadily increased for both men and women between 2008 and 2018 (Figure 2).10)
Figure 2
Trends in intake of energy and macronutrients.
Source: Generated from Korea National Health and Nutrition Examination Survey, KCDC.10)
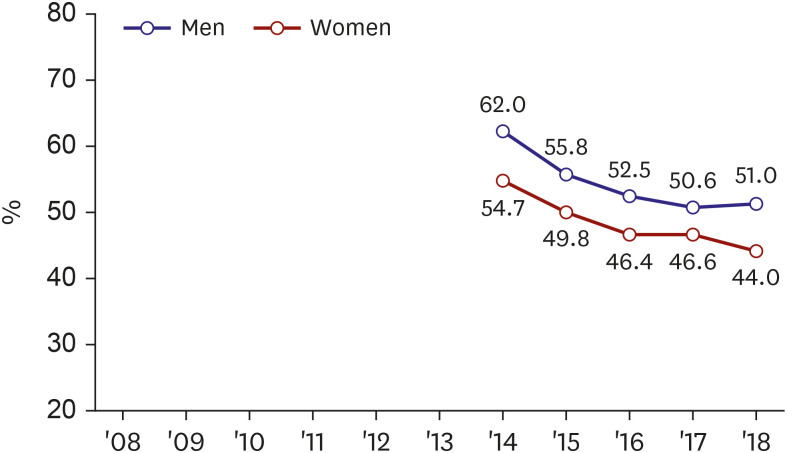
In 2018, the rate of aerobic physical activity was 51.0% for men and 44.0% for women (Figure 3). The strength training practice rate was 31.0% for men, twice as high for women (14.9%). For men in their twenties, this increased from 37.5% (2016) to 43.8% (2018). However, for women this decreased from 22.2% (2016) to 17.3%.10)
Figure 3
Trends in aerobic physical activity.
Source: Generated from Korea National Health and Nutrition Examination Survey, KCDC.10)
Cholesterol
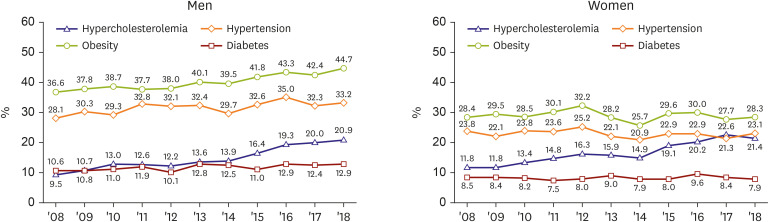
An estimated 56% of ischemic heart diseases and 18% of stroke are attributable to hypercholesterolemia.11) In many countries, averages total blood cholesterol levels tend to increase, with cholesterol levels tending to be higher in urban areas.12)13) According to the results of the 2018 National Health and Nutrition Survey in South Korea, the prevalence of hypercholesterolemia was less than 10% up until 2005, but rapidly increased to 21.4% in 2018.10)
Hypertension
High blood pressure is a major risk factor for CAD, peripheral vascular disease, and stroke. Mean blood pressure and the prevalence of hypertension also tend to increase with industrialization and urbanization. In low-income countries, underdiagnosis and inadequate treatment of hypertension are a serious concern, and has led to the high incidence of cerebrovascular disease.4) In South Korea, the prevalence of hypertension has not changed significantly, but over the past 20 years, the diagnosis, treatment, and management of hypertension have improved significantly, resulting in major reduction in mortality due to stroke (Figure 4).14)15)
Figure 4
Trends in the prevalence of chronic diseases.
Source: Generated from Korea National Health and Nutrition Examination Survey, KCDC.10)
Obesity
Obesity is the underlying driver of metabolic disease such as hypertension, diabetes, and dyslipidemia, with an attendant increased risk of CVD. Obesity rates and prevalence have increased and indeed escalated worldwide, especially in developing countries. In low-come countries, obesity and undernutrition often coexist.4) The prevalence of obesity (body mass index >30kg/m2, standardized) was 42.8% for men and 25.5% for women in 2018.10) Since 1998, the prevalence of obesity in men has increased significantly, while remaining largely unchanged in women.
Diabetes
The prevalence of diabetes is also increasing worldwide, due to rising prevalence of obesity and physical inactivity. Diabetes itself is an important risk factor for CVD, and it is highly correlated with high blood pressure. Genetic susceptibility to diabetes varies with ethnicity, with Asian at higher risk of diabetes compared to European population.16) In South Korea, the prevalence of diabetes was 12.9% in men and 7.9% in women 2018. The older the age in both men and women, the higher the prevalence of diabetes (Figure 4).10)
NATIONWIDE CARDIOVASCULAR REGISTRY
The purpose of this document is to propose a nationwide Korean Cardiovascular Registry to collect cardiovascular epidemiological information and care the registered patients under joint of public/private/academic society with community participation, for improving the quality of car, patient outcomes, and the reduction of health care costs.
Cardiovascular disease registry: the South Korean model
The Korea Acute Myocardial Infarction Registry (KAMIR), which began as a research project commemorating the 50th anniversary of the founding of the Korean Society of Cardiology (KSC) in 2005, was the first nationwide Korean prospective multicenter data collection registry for tracking patient with AMI. Initially, 44 institutions nationwide participated, with more than 76,000 patients with AMI enrolled. To date, KAMIR has conducted and published hundreds of clinical researches and developed guidelines and tools aimed at improving the prevention, early detection, and improved therapies for AMI.17)18)19) This includes the KAMIR risk score which is a risk stratification tool for prediction mortality and outcomes in patients with AMI.20)21)22)23)
Since 2011, KAMIR became the KAMIR-National Institute of Health (NIH), consisting of 20 centers (tertiary university percutaneous coronary intervention [PCI]-capable hospitals) funded by the NIH, that now oversees a prospective, multicenter, on-line cohort of Korean AMI patient. Between 2011–2015, KAMIR-NIH enrolled 13,707 Korean AMI patients, for short-and long-term follow-up for comparative analyses of the effectiveness of treatments and interventions according to patient characteristics, risk factors, and prognostic evaluation. The aim is to employ such findings as the basis for establishing policies and developing guidelines for improving the prevention, treatment, rehabilitation, and treatment of Korean patients with AMI.24)25)26)27)
Since 2016, the Korean Registry of Regional Cardiocerebrovascular center for Acute Myocardial Infarction (KRAMI), a web-based registry that includes 11 regional CCVCs began as a research project of the Korea Centers for Disease Control and Prevention, now renamed Korea Disease Control and Prevention Agency (KDCA). The KRAMI registry, funded by the Ministry of Health and Welfare (MOHW), initially focused on the treatment of AMI and stroke with the aim of improving health equity between local and urban community.28) As its capacity increased, the goal expanded to include rehabilitation and tertiary prevention. The KRAMI registry project is representative of the local population and collects epidemiological and on evidence-based care and health outcomes (Table 1).
Table 1
Comparison of the KAMIR and KRAMI registry28)

National and provincial models: The SWEDEHEART registry and cardiac care network Ontario (Canada)
The Swedish National Quality Registries or SWEDEHEART is a national quality registry supported and funded by the government and the Uppsala Clinical Research Center established in 1995 that oversees the national registry for heart disease. It provides on-line reports for general public, media, and policymakers regarding patient with AMI, secondary prevention data, patients undergoing angiography, PCIs, heart surgery, and patients with the cardiogenetic disease.29)
In Ontario, Canada's most populous province, the University of Toronto manages the province's Cardiac Care Network of Ontario (CCN). Since 2017, the CCN merged with Ontario Stroke Network into CorHealth Ontario. Responsibility for the management of CVDs and stroke expanded to provide both patients and health care providers with the basic data needed for improving the quality of clinical care, planning, resource allocation, and performance.30)
Singapore's acute myocardial infarction registry
In Singapore, the Singapore Myocardial Infarction Registry (SMIR) established in 1988 was initially managed by the government's Ministry of Health and has been fully government funded since 2001. The SMIR oversees the national management of the AMI registry, which collects and analyses epidemiological data to support policy, planning, and evaluation of patients with CVD and stroke. This includes AMI cases diagnosed in all public and private hospitals, as well as AMI deaths that occurred at home, as certified by general practitioners. Since September 2012, Singapore enacted legislation to mandate such notifications from all healthcare institutions. Their annual report in 2018 included trends on the incidence, mortality, 30-day case fatality, symptoms, and risk factors for Singapore residents with AMI during the period 2009 to 2018.31)
US registry provided by professional societies
The National Cardiovascular Data Registry
The National Cardiovascular Data Registry (NCDR) in the USA is suite of data registries—eight hospital-based and two outpatient-based registries—by the American College of Cardiology that is designated to assist hospitals, health systems, and private practices measure and improve the quality of care their cardiovascular care services. In addition to these data-driven performance services, the NCDR aims to ensure that such care services are evidence-based and designed to foster cost-effective care that improves patient outcomes within its network of cardiovascular care provider.32)
The Get With the Guidelines
The American Heart Association (AHA) has an innovative commitment to promoting the clinical registries. The potential value derived from investing clinical registry is demonstrated by national clinical CVD and stroke registries that have matured over the past decade. Prominent examples include the AHA's Get With The Guidelines (GWTG) registries for CAD (GWTG-CAD), congestive heart failure (GWTG-CHF), stroke (GWTG-Stroke).33)
Hospital Compare
Hospital Compare was a California, USA-based initiative that arose out of Hospital Initiative through the efforts of the Centers for Medicare and Medicaid Services (CMS) and the Hospital Quality Alliance (HQA). The HQA was a public-private collaboration established in December 2002. The HQA disbanded in December 2011, and CMS currently maintains the Hospital Compare Web site providing information for consumers to make informed decisions and select hospitals through direct performance comparison related to many conditions.34)
European Society of Cardiology Registries
The EURObservational Research Programme (EORP) was started by the European Society of Cardiology (ESC) in 2009, with the aim of improving medical practice based on observational data collected using robust methodologies.35) It is a large clinical database that includes 20 different registries from more than 2,500 centers with more than 240,000 patients enrolled. Additionally, EORP aims to complement the development of guidelines by measuring how well they are being applied in clinical practice. As such, EORP registries help complete the circle of knowledge that can lead to better treatments. The full involvement of the ESC National Cardiac Societies and relevant ESC constituent bodies will contribute to the ESC mission to reduce the burden of CVD in Europe.
Implementation of nationwide registry under the collaboration of professional society and government
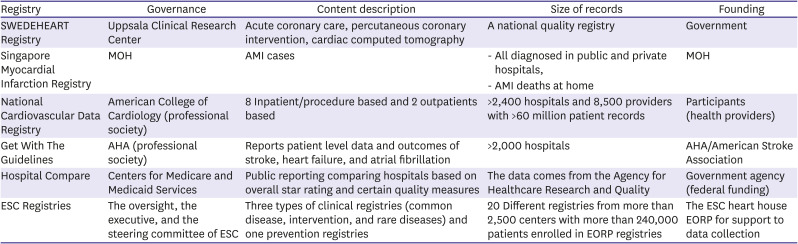
Therefore, when analyzing data and outcomes across a global spectrum, both across and within various countries, cardiovascular patient registries have proven to be effective, and are being rapidly adopted to improve patient care and outcomes provided by specialized healthcare organizations (Table 2).36) They are invariably government-funded efforts, with the USA being an outlier because of the fragmented nature of the American healthcare.
Table 2
Description of representative cardiovascular disease national registries in North America, Europe, and Asia
Within the South Korean context, the establishment of cardiovascular patient registries can be a key part of the national strategy for improving prevention and quality care for AMI and stroke patients. Therefore, such registries supported by the national level are central for helping Korean hospitals and systems in measuring, standardizing, and monitoring improvements in cardiovascular care across the spectrum of pre-acute, acute, and post-acute care for patients with cardio-cerebrovascular disease. Ensuring the accuracy of data collection that is seamlessly integrated with existing electronic medical record systems will significantly improve the usefulness of such registries. Therefore, a key role of professional cardiovascular societies in charge of registries includes the development of standards and definitions of conditions and outcomes that span across all registries to maximize efficiency and integration.
As registries expand, so does the administrative burden on participating hospitals to manually extract and validate data prior to reporting. The current reimbursement system for health care in Korea does not prioritize participation in such registries, preferring instead a less-proactive strategy based on evaluating outcomes based on administrative data. Such an approach is not forward thinking, as more proactive registry-based strategies have shown promise in improving patient care and cost-effective outcomes, both of which are essential for long-term sustainability.
Efforts by the professional societies (e.g., KSC) and other health organizations (e.g., KDCA) are required to initiate and manage nationwide cardiovascular data registry.
To overcome the barriers for sustainable data registry in the all hospitals, a Network of Regional and local CCVCs should be introduced to organize the national registry system in order to upload registry data, with funding support from government and health authorities.
In case of National Cancer Registration Program in South Korea, the Central Cancer Registration Headquarter was established at the National Medical Center in 1980 to execute the Korea Central Cancer Registry by the MOHW. Cancer registration program was started with voluntarily participation of the hospitals and has since expanded nationwide, including all hospitals that can diagnose and treat patients with cancer.
The Cancer Registration Headquarter was transferred to National Cancer Center in September, 2000 and National Cancer Control Institute was designated as a new organization in December, 2004 according to the Cancer Control Act.37)
We propose that the tentative name “National Myocardial Infarction Patient Registry Project” should begin with both the KSC and KDCA, followed by promoting voluntary participation of all CCVCs nationwide. To this end, we propose that this project should receive funding and support from government and local governments for patient management costs.
Additionally, the registry management headquarter can be temporarily established in one of the regional CCVCs. Thereafter, when the central CCVC is launched, a roadmap can chart for formal transfer the dedicated the headquarter.
IMPLEMENTATION OF NATIONWIDE CARDIOVASCULAR CARE NETWORK
The Cardio-cerebrovascular Disease Prevention and Control Act was enacted in May 2017 in Korea. This law has become the first ever legislative countermeasure against stroke and CVD in Korea. The government have made a “Comprehensive Plan to Promote Cardio-cerebrovascular Disease Control Programs” with input from a council consisted of stakeholders. In accordance with the government plan, a nationwide approach is expected to make five strategies to reducing the burden of disease and to prolong healthy life expectancy.
It is time to for the cardiac professional societies to recommend expanding regional CCVCs, improving their functions, and implementing a regional network system including local cardiovascular centers in relation to community emergency response and enhancement of treatment capabilities—consistent with one of the five strategies for the National Health Plan for Cardiovascular Disease.
Establishment of regional cardio-cerebrovascular centers and unmet needs
Regional CCVCs were implemented for the prevention and treatment of CVD and initially funded by the MOHW in 2008. Each province was comprised of nine zones, expect for the metropolitan areas, National hospitals and private university hospitals serve as regional CCVCs in each region. The program was continually expanded to up to 2018, and 14 regional CCVCs are now in operation.38) The government builds and operates a system in regional CCVC that could receive intensive care quickly within 3 hours when the disease occurred. The goal of this project was to minimize the incidence of complications and mortality through the provision of timely medical services anywhere in the country and to facilitate earlier return to society after complete recovery.
As a result of these efforts, the treatment of myocardial infarction and stroke has been partially improved. The results, however, were mixed. This led to improved outcomes and less acute fatality rates for patients who arrived within the golden hour. However, the same could not be said for overall in-hospital mortality.39)
The OECD Health Care Quality Assessment Report and in 2012 recommended the need to improve the overall quality of care for CVDs in all sectors in South Korea. They highlighted a significant variation the quality of cardiovascular care and health outcomes that exist between in-patient hospital care compared to outpatient care, specifically, primary prevention and rehabilitation were insufficient.4)
In addition to primary prevention and rehabilitation, the establishment of an efficient and appropriate national health care system for acute patients to receive appropriate treatment during golden hour remains an important task. Therefore, it is essential to establish an appropriate system for the management of cardio-cerebrovascular diseases in regional CCVCs for rapid and effective treatment of acute patients and regional network system including local CCVCs that can primarily respond to emergency situations in the community. First of all, when looking at the current status of regional cardiocerebrovascular disease centers and the status of professional workforce, there are currently 153 institutions for primary PCI nationwide.
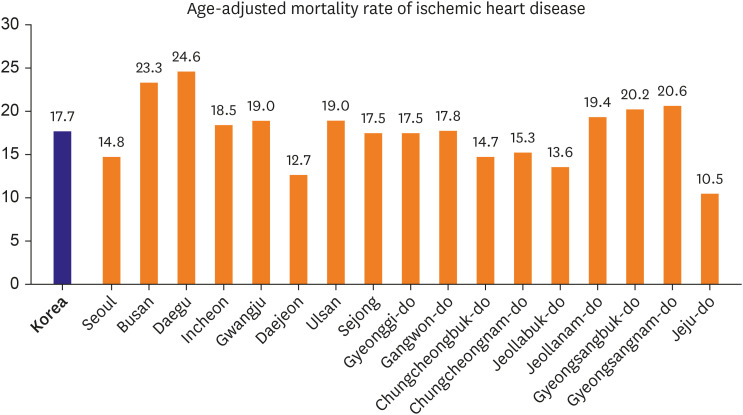
According to the human resources data from the PCI certification system of the Korean Society of Interventional Cardiology,40) there are 84 qualified PCI centers. Average number of certified doctors are 3.4 at each certificated center. Among them, only 17 centers including regional CCVCs have more than 5 certified doctors enough to response emergency care. However, the glaring disparity is that only 20% of AMI patients are managed at regional CCVCs which receive partial government support. In addition, most of these 84 institutions have regional emergency medical centers, but diagnosis, treatment, and procedures for patients with myocardial infarction are operated by separate medical staff from the emergency center. The existing Emergency Medical Care Act does not make provisions for such funding by the government. Therefore, limitations in staffing and availability of emergency personnel, as well as health insurance coverage, pose major challenges for improvements in acute care, as well as pre-and post-acute care services. Therefore, government support is essential to maintain appropriate staffing at such regional centers. Building a network of existing regional CCVCs and private hospitals in the community is, therefore, critical for strengthening emergency response and preventive care for AMI patients and stroke. Institutions in the rural area are especially not equipped to handle 24-hour coverage year-round, primarily due to the unavailability or lack of full-time certified personnel, including cardiologist and internal medicine specialists.41) Due to the geographic maldistribution of healthcare infrastructure, AMI patient mortality rates are higher in rural areas compared to urban areas, including Seoul.14) In addition, the data on the mortality rate of ischemic heart disease in the 17 regions42) shows marked differences in mortality rates between regions (Figure 5).
Expanding regional cardiocerebrovascular centers and implementation of regional network system including local cardiocerebrovascular centers
To increase the effectiveness of the regional CCVCs project, it is necessary to establish and designate the “Central Cardiocerebrovascular Disease Center” as the control tower and policy support for the national project, as well as designating local CCVCs to cooperate with the regional CCVCs. A variety of models should be developed and applied based on the size of the local center and capability. It is essential to establish a regional network system where active participation of related organizations such as local governments, emergency medical centers, and 119 Emergency Center is ensured.
To overcome the barriers to rapid reperfusion therapy in the community, a regional ST-segment elevation myocardial infarction (STEMI) network was introduced to organize care between non-PCI hospitals, ambulance, and PCI centers facilitate rapid reperfusion therapy in the western community as recommended by the AHA and the ESC clinical guidelines.43)
The STEMI networks introduced in Europe and the United States has increased the utilization of rapid reperfusion therapy in the community.44) This served as a model for several countries for establishing national and regional STEMI networks for improving outcomes for STEMI patients in (Figure 6).
Figure 6
Flowchart for reperfusion strategy based on 2017 ESC guidelines for the management of STEMI.
Adapted from Ibanez B, James S, Agewall S, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J 2018;39:119‐77.45)
EMS = emergency medical services; ESC = European Society of Cardiology; PCI = percutaneous coronary intervention; STEMI = ST-segment elevation myocardial infarction.
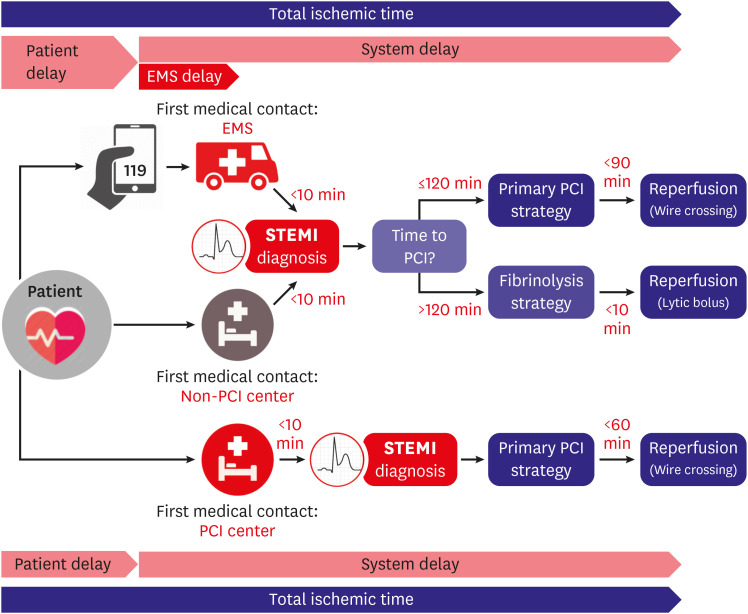
Ischemic time begins with the onset of chest pain in the pre-hospital/community setting. To increase awareness of the community, a public health campaign for optimal management of chest pain should be implemented. At non-PCI center, the process of care begins with when the patient at the hospital's emergency department (ED) until the initiation of reperfusion therapy. The time of admission-to first medical contact are all included in the process of non-PCI center care. The performance of treating STEMI patients at non-PCI center can be measured by the door in-door out (DI-DO) time defined as the duration of time from patient arrival to discharge from the referring center.45) A door-to-device time <60 minutes for STEMI patients begins with the patient arrives at the ED to the time for device deployment at PCI centers. This includes several care steps from ER admission to activate the cardiac catheterization laboratory, transfer patient, and begin the definitive PCI procedure.
The management of patients with STEMI requires a standardized system of care to minimize delays to reperfusion therapy at each step, with the aim for continuing improvements. In such cases, the DI-DO time is likely to be an important ischemic time metric in determining the overall delay to primary PCI that correlates with total ischemia time (Figure 6).
Necessary interventions include training the emergency physicians and nurses work at non-PCI community centers, along with rapid ECG transmission and transfer decisions, rapid ambulance coordination, and possible fibrinolytic therapy whenever there are delays in the transfer of patients with high probability for primary PCI. In PCI centers, future improvements for avoiding delays for primary PCI include bypassing the ED process by transporting patients directly to the catheterization laboratory. In such a scenario, care received at the non-PCI center care will play a pivotal role in minimizing total ischemic time. 119 emergency medical services (EMS) services could be equipped to diagnosis AMI in the field, notify a PCI center capable of timely reperfusion, and transfer directly to the catheterization suite.
Health authorities and local government need to improve public awareness to promote early seeking 119 assistance, as well as coordination of EMS with the network of regional PCI centers and community non-PCI centers. This can be made possible by expanding the role of pre-existing regional CCVCs and implementation of new local cardiocerebrovascular centers. It is difficult to improve access and follow-up management of CVDs like AMI by establishing a single regional CCVC in each province. Based on the analysis of the patient access and the status of local medical resources, local CCVCs require additional designation and government support.
A national plan for fostering and distributing cardiovascular health professional workforce is required, rather than relying on private hospitals for the establishing conditions at regional centers. To establish effective regional networks for coordinating patient care at regional and local centers, collaboration between all health care stake holders and local governments is essential. To do so, regulations and health insurance reimbursement policies must be improved. In addition, regional emergency centers and primary local medical institutions that are not included in regional or district centers should be encouraged to participate in patients' medical information collections and all-inclusive treatment systems (information, transfer, and timely care network).
Finally, innovation in health technology for improved ECG transmission and communication between non-PCI centers, ambulance, and PCI centers, along with routine performance measures of the STEMI network should help in implementing regional cardiovascular healthcare systems. This program can be possible only through collaboration between the national medical societies, local government, and health care authorities.
CONCLUSION
The prevalence of CVD in South Korea is expected to increase, as it has one of the most rapidly ageing populations—a non-modifiable risk factor for CVD—with those aged 65 years projected to reach 37% by 2050.4) Therefore, focusing on modifiable lifestyle risk factor prevention, proactive primary care services will be critical for reducing the future burden of CVD.
While the government's strategy for improving CVD quality of care is geared mainly toward strengthening prevention and in-hospital care, adopting best-practice care delivery models for CVD—in the view of paradox between high-quality hospital care and weaker out-of-hospital care for CVD—is s a highly recommended addition to the current policy. The Korean government's Comprehensive Plan for CVD is the major national policy driver for improving the quality of care, most notably through the creation of regional cardiovascular centers. Ideally, these centers should serve as vertical institutions that provide services ranging from acute care to health promotion and rehabilitation.46) To eliminate or minimize the disparities in acute care and case fatalities between rural and urban areas, expansion of regional CCVCs and establishment of new local CCVCs are highly recommended.
Cardiovascular patient registries are proven, effective strategies in tackling the escalating socioeconomic burden of CVDs. Among leading countries, such registries managed by specialized health care organizations and medical institutions provide key data used to plan health strategies and improve patient care and outcomes. There is consensus that healthcare infrastructure should be incorporated and emphasized promotion of acute care accessibility, effective primary and secondary prevention of CVD to minimize adverse sequelae in Korea.
We propose a nationwide Korean Cardiovascular Registry to collect epidemiological information for quality of care under joint public/private/academic societies. In concert with preventive strategies, it is essential to establish an emergency response system at the community level to optimize acute cardiovascular care for patients within the golden hour. For such a response system to succeed, it will require local and national government support, as well as inputs from medical and academic societies. The government and the 11 regional CCVCs have been effective in improving the case-fatality rate of AMI during acute in-hospital care.
However, to eliminate existing disparities that characterize the Korean CVD mortality “paradox”, we recommend expanding regional CCVCs, improving their functions, and implementing a regional network system that includes local CCVCs to improve and enhance community emergency responses in accordance with the National Health Plan for Cardiovascular Disease. Furthermore, to improve health outcomes for all stages in acute CVD management, the development of a regional STEMI network that includes the pre-and post-hospital care is essential to achieve the stated national goals.
 XML Download
XML Download