

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
According to the World Health Organization's report, the annual prevalence of depression is 4.4%, and its lifetime risk is 15–18%. Depression is a common condition; one in five people experience it at least once during their lifetime.1 However, depression is more common when accompanied by a physical condition, and it is well known that depression is associated with chronic diseases, such as arthritis and diabetes.2 In chronic disease patients, depression management is important, as physical stress increases the risk of depression. The prevalence of major depression disorders is 3.7–6.7%, while the prevalence of depression accompanying physical illness is 5–10% for inpatients and 9–16% for outpatients.3 There is a clear association between depression and chronic disease in the elderly, with more than 75% of depressed elderly patients having physical illnesses and 30–50% of them having high morbidity.4 Although the prevalence of depression is generally lower in population groups aged 60 years and above than in younger age groups, high prevalence is reported in sub-groups such as those with chronic physical conditions.5 Depression affects the physical and mental state of a person, thereby reducing the quality of life and causing public health problems, such as alcohol consumption, smoking, and drug abuse, thus resulting in higher mortality and morbidity than that expected simply from the physical condition itself.
Multimorbidity, a term used to describe the presence of two or more chronic conditions, is increasing, given the trend of global aging with clusters of illnesses.6 A study found that 75% of individuals aged 65–74 years had multimorbidity, with the proportion rising to 80% in those aged 75 years and older.7 As our society continues to age, the prevalence of multimorbidity and mental problems is expected to increase; the mental problems, especially depression, must be addressed.
People with chronic diseases consume a lot of medical resources for treatment, and this increases the risk of depression by increasing stress vulnerability.8,9 The utilization of medical resources is more likely to increase with a combination of depression and chronic illness than in the case of chronic illness alone. Some studies show that depression is an important factor that leads to excessive use of medical resources in hospitalized and outpatient patients. High utilizers, who consume a lot of medical resources, account for 64% percent of the total cost of medical resources, 23.5% of whom are reported to have depression and 16.8%, dysthymic disorder. The disease burden of depression is reported to increase every year, and it is estimated to be the second most common disease by 2030.10-12
In the case of patients with chronic disease, it is important to evaluate not only the risk factors for existing diseases but also the social and psychological stress factors that can cause depression. Depression is highly relevant to social and cultural factors, so it is necessary to study the domestic population. Several epidemiological studies have reported the prevalence of depressive symptoms in the Korean population. Epidemiological surveys on mental disorders in Korea reported a gradually increasing lifetime prevalence of major depressive disorder (2001, 4.0%; 2006, 5.6%; 2011, 6.7%).13,14 Recently, there was a study consisting of a nationwide, population-based survey that assessed the prevalence of depression in the general population using the Patient Health Questionnaire (PHQ)-9. The point prevalence of depression was 6.7% and the prevalence of major depressive disorder was 2.7%. The study also reported that the factors associated with depression were perceived stress and the presence of chronic disease.15 This study aimed to investigate the combined effects of depression and multimorbidity on all-cause mortality using data from a large-scale cohort study of Korea.
Go to : 
METHODS
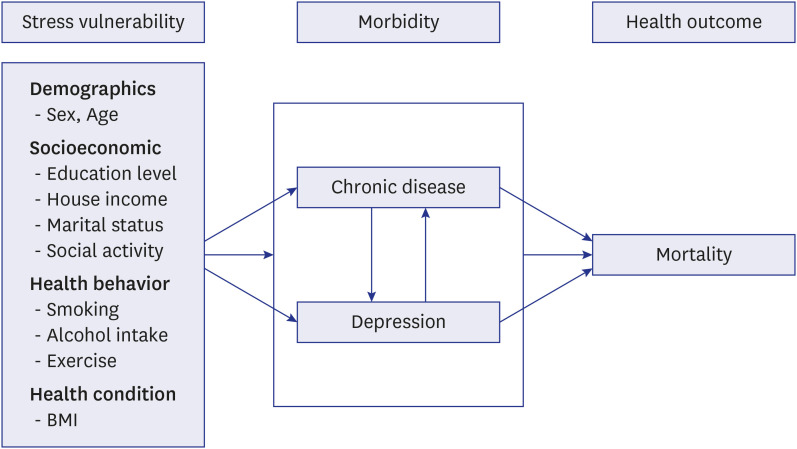
Hypothesis
Study population
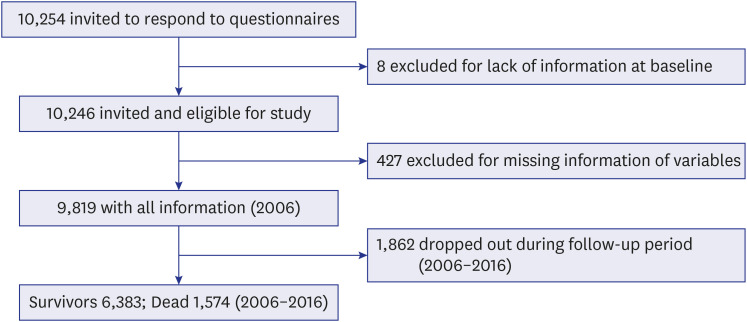
We used data from 2006 to 2016 from the Korean Longitudinal Study of Aging (KLoSA), conducted by the Korea Labor Institute of the Ministry of Labor every two year. KLoSA is an ongoing longitudinal panel survey of a sample of community-dwelling people aged 45 to 79 years old who were alive at the time of the baseline interview in 2006. The data were collected using structured questionnaires with computer-assisted personal interviewing (CAPI) method. CAPI is an interviewing technique in which the interviewer uses an electronic device to answer the questions. In the 2006 baseline survey, the original panel interviewed 10,245 participants. Our study sample included 9,819 individuals; we excluded 435 individuals whose health information was absent at baseline. The flow chart of participant selection is shown in Fig. 2.
Covariates
The baseline characteristics, demographics, and health behaviors of the study participants were the variables of interest. The demographic variables were age (45–65 years or ≥ 65 years), marital status (married, divorced/widowed, or never married), social activity (none, more than one, more than two), education level (≤ 6 years, 7–11 years, 12–15 years, ≥ 16 years), and annual household income (≤ 10,000,000 KRW, 10,000,000–30,000,000 KRW, ≥ 30,000,000 KRW). Health behavior variables included cigarette smoking (current smoker, former smoker, or never smoked), alcohol consumption (current drinker, former drinker, or non-drinker), and physical activity (more than once a week or less). Additionally, body mass index (BMI) was calculated using the height and weight, and the participants were categorized as underweight (< 18.5), normal weight (18.5–24.9), overweight (25–29.9), or obese (≥ 30).
Health status assessment
The health status variable was the number of chronic diseases. It was collected from self-reported disease history. The respondents reported the presence of one or more physician-diagnosed diseases, namely hypertension, diabetes mellitus, cancer, chronic lung disease, chronic liver disease, cardiovascular disease, stroke, arthritis, and psychiatric disorders. Psychiatric disorders include depression, anxiety, insomnia, excessive stress, neurological problems and interpersonal relationships. Respondents with psychiatric disease were excluded in this study. We categorized study participants according to their multimorbidity status at baseline as having either no, 1 condition or over 2 conditions (multimorbid).
Measurement of depression
Depression was measured by the short version of the Center for Epidemiologic Studies for Depression Scale (CESD-10), a brief screening instrument that assesses depressive symptoms experienced during the most recent week. The Korean version of the scale was translated by Cho et al.17,18 and the validity of the scale was established by Shin et al.19 The CESD-10 has good internal consistency, acceptable test-retest reliability and has shown a statistically significant correlation in many reliable studies.20-26 In the KLoSA dataset, participants are asked to rate how often they have experienced feelings such as “depressed” or “lonely.” Items range from 0 (rarely or none of the time; less than one time per day) to 3 (most of the time; 5–7 days). Total scores range are 0–30, and higher scores indicate the presence of more depressive symptoms. We used cut-off score of 10 or greater in the CESD-10 to identify clinically relevant depressive symptoms. This cut-off was reported to be valid in population study.27-29 The depression group was divided into two groups to differentiate the severity of depression, if the CESD-10 score was 14 or higher, the participant was considered severely depressed.
Outcome assessment
The main outcome in this study was all-cause mortality. Mortality risk was assessed using survival status and survival months calculated from months lived from the baseline (2006) to 2016. Death over a maximum follow-up period of 10 years was determined by death certificates.
Statistical analysis
Analysis was performed in two directions. First, Pearson's chi-square test was used for comparative analysis between the groups. Second, Cox proportional hazard regression was conducted longitudinally to investigate the relationship between depression and mortality risk by stratifying multimorbidity. The hazard ratios (HRs) for all-cause mortality with 95% confidence intervals were expressed for the results. SPSS for Windows version 18.0 was used for statistical analysis. Statistical significance was set at P < 0.05.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Daegu Catholic University Hospital (approval No. CR-19-153). Informed consent was waived because of the retrospective nature of the study.
Go to :
RESULTS
This study comprised a total of 9,819 participants at baseline, i.e., 2006. Of these, 8,099 (82%), 988 (10%), and 732 (7.4%) were categorized as having no depression, mild, and severe depression, respectively. Most participants with mild and severe depression were elderly and female, had low education and income levels, and had normal BMI. However, there was a major difference in the prevalence of underweight among those with depression and those without. A large proportion of participants with mild and severe depression were underweight. Further, participants with mild and severe depression showed significantly low social engagement (social activity and marriage status) and physical activity and heavy smoking and alcohol drinking, which tended to increase with the severity of depression. Of participants with one chronic disease, 12.4% had mild depression and 8.5% had severe depression. And of participants with multimorbidity, 16.6% had mild depression and 15.4% had severe depression. The higher the number of chronic diseases, the higher the prevalence of depression (Table 1).
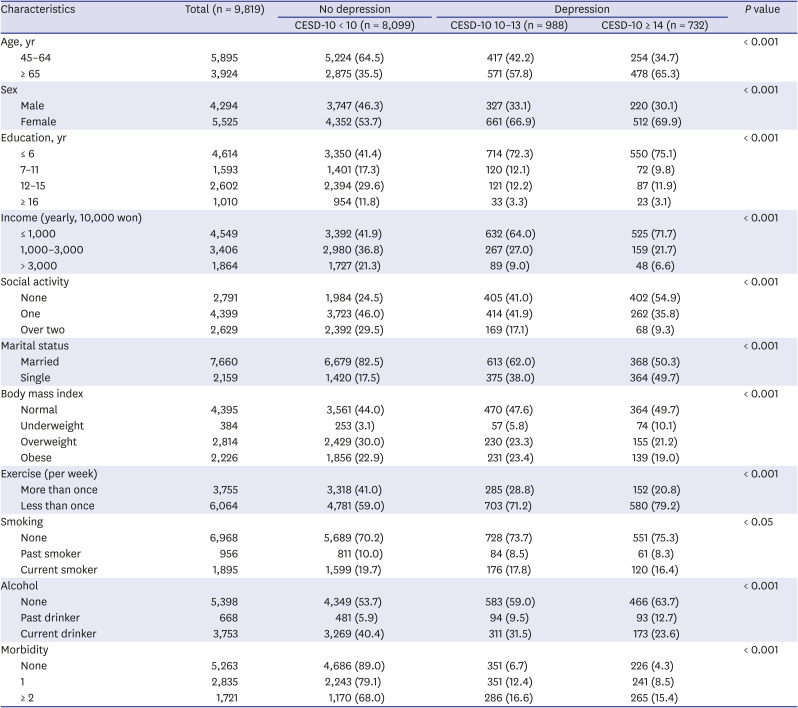
Table 1
General characteristics of the study population (n = 9,819) by depressive status as per the CESD-10 at baseline 2006 of KLoSA
Values were presented as number (%) and mean ± standard deviation.
CESD-10 = the 10-item version of the Center for Epidemiologic Studies Depression scale, KLoSA = Korean Longitudinal Study of Aging.
![]()
During 10-year follow up, out of the 9,819 participants gathered at baseline, 1,574 (16.0%) were reported deceased. The proportion of the depressed with CESD-10 or higher was higher in the deceased group, and the proportion of the chronic disease was also significantly higher in the deceased group (Table 2).
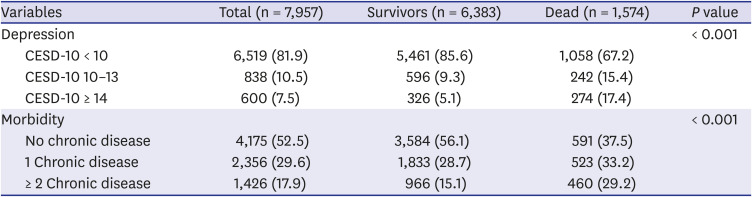
Table 2
Association between depression and multimorbidity by survival status
![]()
Table 3 shows the HR of all-cause mortality according to depression and multimorbidity. Regarding depression, those with a CESD-10 score of < 10 served as the reference group. On multivariate analysis, a significantly increased risk of mortality was indicated for participants with mild and severe depression; the HR was 1.28 (95% CI, 1.11–1.48) with mild depression and 1.91 (95% CI, 1.65–2.21) with severe depression. Regarding multimorbidity, no chronic disease served as the reference group. Increased risk of mortality was also significantly associated with multimorbidity. From the multivariate analyses, the HR was 1.18 (95% CI, 1.05–1.34) for 1 chronic disease and 1.61 (95% CI, 1.42–1.83) for multimorbidity (Table 3).
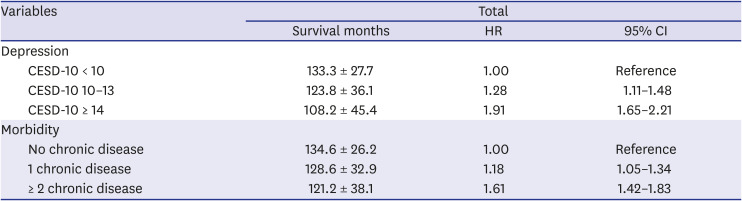
Table 3
Hazard ratios of all-cause mortality according to depression and multimorbidity for 10-year-all-cause mortality
Values are presented as number (%) and mean ± standard deviation and hazard ratio (95% CI).
Model adjusted for age, sex, education level, marital status, house income, social activity, exercise, alcohol consumption, smoking, and body mass index.
HR = hazard ratio, CI = confidence interval, CESD-10 = the 10-item version of the Center for Epidemiologic Studies Depression scale.
![]()
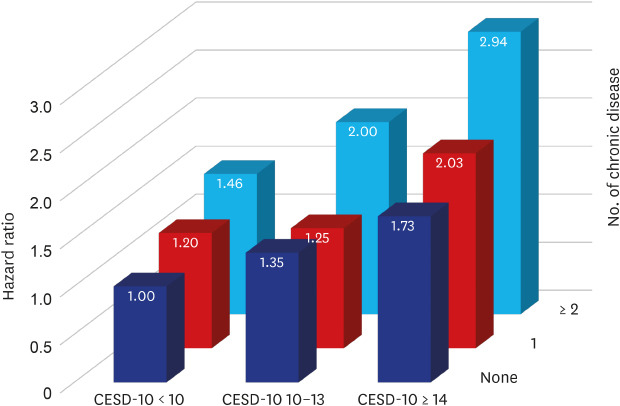
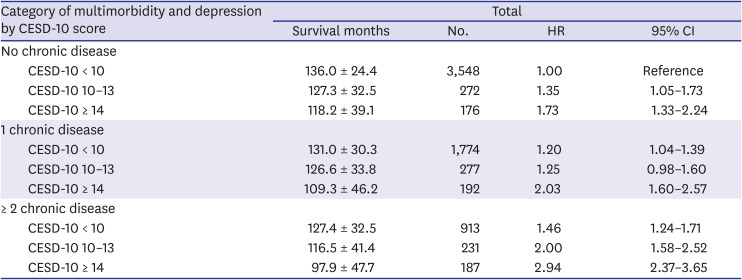
Next, we examined the combined effect of depression and multimorbidity on all-cause mortality. As shown in Table 4, the HR associated with mild depression increased from 1.35 (95% CI, 1.05–1.73) for no chronic disease, to 1.25 (95% CI, 0.98–1.60) for 1 chronic disease, and to 2.00 (95% CI, 1.58–2.52) for multimorbidity. The HR associated with severe depression increased from 1.73 (95% CI, 1.33–2.24) for no chronic disease, to 2.03 (95% CI, 1.60–2.57) for 1 chronic disease, and to 2.94 (95% CI, 2.37–3.65) for multimorbidity. The combined effect of depression and chronic disease was greater on total mortality than of each independent factor. We found a statistically significant effect of the interaction between multimorbidity and depression on mortality (P < 0.001) (Table 4 and Fig. 3).
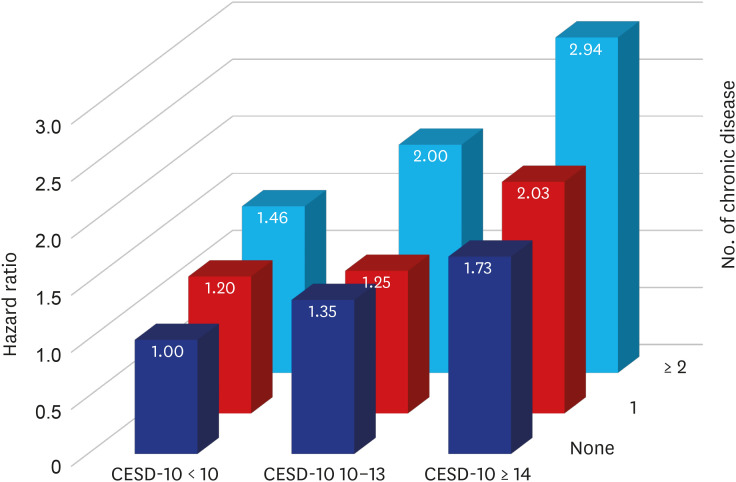 | Fig. 3Hazard ratios (95% confidence interval) of the combined effect of depression and multimorbidity on all-cause mortality; the Korean Longitudinal Study of Aging, 2006–2016.CESD-10 = the 10-item version of the Center for Epidemiologic Studies Depression scale.
|
Table 4
HR (95% CI) of the combined effect of multimorbidity status and depression on all-cause mortality from the Korean Longitudinal Study of Aging, 2006–2016
Values are presented as number (%) and mean ± standard deviation and hazard ratio (95% CI).
Model was adjusted for sex, age, education level, marital status, house income, social activity, body mass index, exercise, alcohol consumption, and smoking. There was a significant interaction between multimorbidity and depression (P < 0.001).
HR = hazard ratio, CI = confidence interval, CESD-10 = the 10-item version of the Center for Epidemiologic Studies Depression scale.
![]()
Go to :
DISCUSSION
Our study showed the findings of the survival analyses examining the combined effect of depression and chronic disease on all-cause mortality among people of the KLoSA cohort over a 10-year follow-up period. This study found that individuals with coexisting multimorbidity and depression are at an increased risk of all-cause mortality compared with those with chronic disease or depression alone. Chronic disease and depression are independent factors that increase the risk of death, and a combination of these two diseases can be a strong predictor of mortality. These results were significant even after having controlled for age, sex, marital status, social activity, education, income, BMI, alcohol consumption, smoking, and exercise. The mortality risk increased for 1 chronic disease in all 3 depression statuses (none, mild depression, severe depression) at 1.20, 1.25, and 2.03, respectively, and for 2 chronic disease at 1.46, 2.00, and 2.94, respectively, compared to the no chronic disease and no depression groups.
According to many studies, depression is an important risk factor contributing to poor outcomes for chronic illnesses, such as cardiovascular diseases.30 Major depression is reported as the most important independent predictor of poor outcomes over 12 months after myocardial infarction. Moreover, depressed patients with coronary heart disease were 6 times more likely to have ventricular tachycardia in a 24-hour evaluation than patients who were not depressed.31-36 Considering that depression is a preventable risk factor for poor outcomes of physical illnesses, our findings could have important implications for the treatment of depression in chronic disease patients.
It is vital to consider the possible mechanisms behind the increased mortality due to the combination of depression and chronic disease. The increased risk of mortality due to depression in chronic disease can be explained by the changes in the neurobiological system. First, changes in the heart rate caused by excessive stress lead to abnormal response of the autonomic nervous system and enhanced platelet aggregation/activation causing blood clots, subsequently increasing the risk of coronary disease. Second, in stress situations, the body activates the hypothalamus-pituitary-adrenal axis and sympathetic neural tones, thereby increasing serum levels of low-density lipoprotein (LDL) and increasing the risk of cardiovascular disease. Third, increased levels of biomarkers such as tumor necrosis factor, interleukin-6, and C-reactive protein lead to chronic inflammation as well as insulin resistance, thus increasing cardiovascular risk, which can affect mortality.37-41 Besides these biological factors, depression affects individuals with chronic diseases by affecting their behaviors. Lack of acceptance of treatment, limited problem-solving skills, and hopelessness contribute to poor treatment adherence, compromised outcomes, and increased risk of negative health behavior such as alcohol consumption and smoking. These factors aggravate comorbidity and mortality.42
There is insufficient evidence on the treatment of depression in chronic disease and its effect on survival rates. In one randomized study, the risk of mortality was not significantly different between depressed patients with the highest level of medical comorbidity and depressed patients with minimal medical comorbidity, both receiving interventions, and nondepressed patients receiving interventions showed a similar mortality risk to those two groups.43 This means that depression management can mitigate the combined effect of multimorbidity and depression on mortality. Therefore, depression management should be integral to optimal patient care.
Our study has several limitations, mostly related to the KLoSA dataset we analyzed. First, depressive symptoms were assessed in this study using only CESD-10, a symptom rating scale. The dataset included a four-point-scale rather than the conventional two-point scale18 usually used in South Korea, which may have weakened the validity of findings. And the cut-off level between mild depression and severe depression is not established. It is a value that to classify the severity of depression to indicate the relationship between depression and multimorbidity. Furthermore, all the factors related to depression may not have been considered. Second, data collection was based on self-report, which is a standard practice in community studies, but there is a possibility of inaccuracy and subjectivity. Data were collected on limited variables through questionnaires – multiple factors could have been involved in depression, chronic disease, and risk of mortality. So, it is hard to generalize the findings to a more specific population (e.g., inpatient). Third, we did not consider the weight of relatively serious diseases such as cancer, cardiovascular disease, or stroke. However, the survey results were not significantly affected because of the low frequency of severe diseases. Finally, we were unable to measure the changes in depressive symptoms, chronic diseases, and other variables throughout the follow-up period because the 2006 baseline data were cross-sectional data.
Our study has some strengths. The sample size is large, and the follow-up period is relatively long compared with that in other studies. The outcome showed significant results for the general population in Korea and not for specific disease groups such as cardiovascular disease patients.
This study analyzed the combined effect of depression and multimorbidity on all-cause mortality using data from a 10-year cohort of the KLoSA. This study showed that individuals with coexisting multimorbidity and depression are at an increased risk of all-cause mortality compared with those with chronic disease or depression alone. Chronic disease and depression are independent factors that increase the risk of death, and a combination of these two diseases can be a strong predictor of mortality. Therefore, depression should be recognized as a risk factor for worse prognosis of chronic disease and patients with multimorbidity and severe depression must be provided integrated assessment and treatment.
Go to :
 XML Download
XML Download