

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
It has been shown that the inflammation plays a major role in the initiation and progression of atherosclerosis.1 Inflammation promotes coronary atherosclerotic plaque rupture and development of thrombosis, which are the main mechanisms in the pathophysiology of ST-segment elevation myocardial infarction (STEMI). The neutrophil-to-lymphocyte ratio (NLR) has emerged as an important inflammatory marker for cardiovascular risk stratification and has shown to be associated with worse outcomes in patients with acute coronary syndromes (ACS) and established coronary heart disease.2 Recent accumulating evidence points out that high NLR to be independently and strongly associated with increased risk of complications and mortality in post MI patients.3 Patients with ACS have higher mortality rates, especially during the first 30 days.4 NLR has been shown to predict adverse in-hospital mortality and morbidity.5 Furthermore, in previous studies, the NLR has been demonstrated to be related to in-hospital major adverse cardiac events (MACE) and cardiovascular mortality in patients with STEMI.67 Although the relationship between NLR and in-hospital MACE in STEMI has been studied, previous studies have not focused on the relationship between NLR and in-hospital mechanical complications in STEMI patients. Thus, we investigated whether an elevated NLR measured at admission is associated with mechanical complications of STEMI undergoing primary percutaneous coronary intervention (PCI).
Go to : 
METHODS
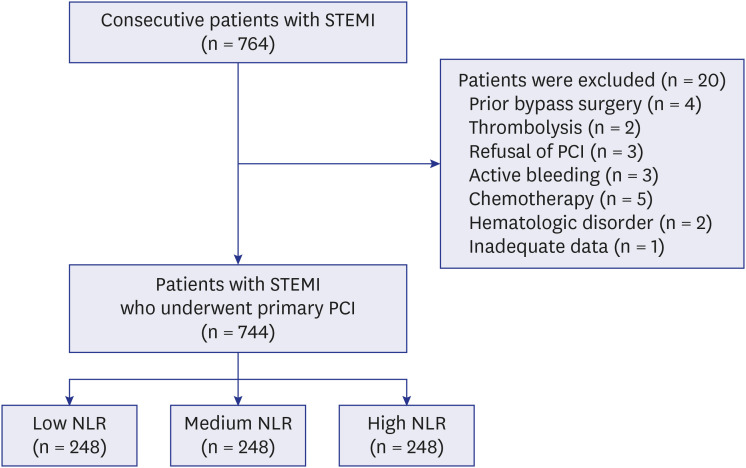
A total of 744 consecutive patients with STEMI who underwent primary PCI from July 2009 to June 2018 at Inha University Hospital were retrospectively included in this study (Fig. 1). STEMI was defined as the characteristic symptom of myocardial ischemia in association with persistent electrocardiographic changes of ST-elevation and positive cardiac enzymes. Exclusion criteria were mainly medical conditions that could affect the total or differential white blood cell counts such as hematologic disorders, malignancies, a history of chemotherapy or radiation therapy, evidence of inflammatory or infectious diseases, and use of corticosteroids. Patients with history of coronary artery bypass graft surgery and previous intravenous thrombolytic therapy before PCI were also excluded.
Total leukocyte count and its subtypes, including neutrophils and lymphocytes, were obtained initially at emergency room (ER). Complete blood cell count samples were analyzed by the XE-2100 (Sysmex Inc., Kobe, Japan). The NLR was calculated as the ratio of neutrophil count to lymphocyte count.
All patients were pre-treated with a loading dose of acetylsalicylic acid (300 mg) and clopidogrel (600 mg) or ticagrelor (180 mg) or prasugrel (60 mg). Unfractionated heparin was used before transfer to the catheter laboratory (5,000 U) and additional heparin was used during the procedure. Use of glycoprotein IIb/IIIa, aspiration thrombectomy and PCI technical strategies were performed according to the physician's decision. Coronary flow before and after the procedure was assessed and described according to the thrombolysis in myocardial infarction (TIMI) criteria. A baseline transthoracic echocardiogram was performed within 24 hours of primary PCI. Patients were divided into tertiles on the basis of their NLR.
Mechanical complication of STEMI was defined by STEMI combined with cardiovascular death, sudden cardiac arrest, stent thrombosis, post MI pericarditis, post MI ventricular septal rupture, ventricular free-wall rupture, left ventricular thrombus, and acute mitral regurgitation during hospitalization.
Statistical analysis
Categorical variables are expressed as frequencies (percentages) and Pearson's χ2 tests were used for analysis. Continuous variables are expressed as the mean ± standard deviation and one-way analysis of variance was used for analysis. Logistic regression analysis utilizing backward elimination method was performed to investigate the association between NLR and variables using clinical, laboratory, echocardiographic, and angiographic data. Omitted columns represent multivariate parameters which were not statistically significant. A P value < 0.05 was considered statistically significant. Statistical comparisons were performed using SPSS version 19.0 (SPSS Inc., Chicago, IL, USA).
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of the Inha University Hospital, Inha University College of Medicine (2016-12-002). Informed consent was submitted by all subjects when they were enrolled.
Go to :
RESULTS
The baseline clinical characteristics of the patients divided into 3 groups according to the NLR tertiles are listed in Table 1. Patients with high NLR were significantly younger and tended to have a higher frequency of dyslipidemia. White blood cell (WBC) counts were significantly higher in the high NLR group than those in the low and intermediate NLR groups. High-sensitivity C-reactive protein (Hs-CRP) and cardiac biomarker levels were also higher in the high NLR group than those in the low and intermediate NLR groups. Angiographic and procedural characteristics of the 3 NLR groups are shown in Table 2. The prevalence of multivessel disease was similar across all 3 groups (P = 0.199).
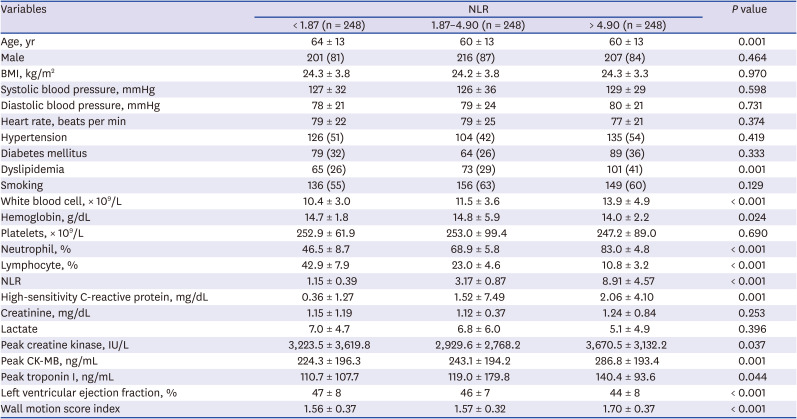
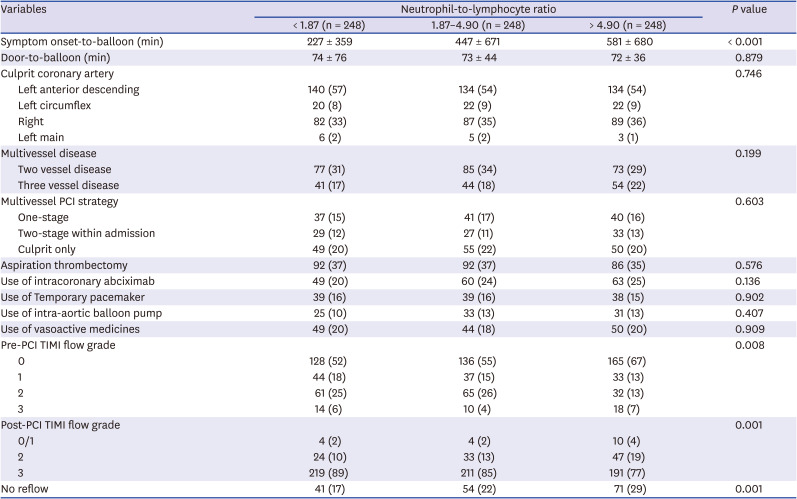
Table 1
Baseline clinical, laboratory, and echocardiographic characteristics according to NLR tertiles
BMI = body mass index, NLR = neutrophil-to-lymphocyte ratio, CK-MB = creatine kinase myocardial band.
![]()
Table 2
Angiographic and procedural characteristics according to NLR tertiles
![]()
Symptom onset-to-balloon time significantly increased with tertiles getting higher. However, door-to-balloon time was not significantly different by NLR groups. Pre-PCI TIMI flow grade 0 portion gradually increased as the NLR tertile increased. In contrast, post-PCI TIMI flow grade 3 portion gradually decreased as the NLR tertiles increased. In addition, a higher prevalence of no-reflow phenomenon after primary PCI was observed as the NLR tertiles increased.
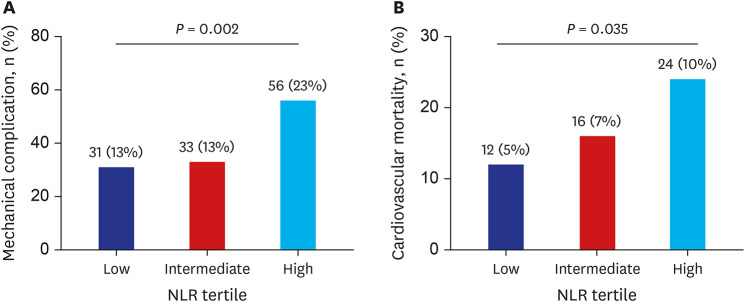
Clinical outcomes of mechanically complicated STEMI are summarized in Table 3. There were 120 mechanically complicated STEMI patients. Patients with high NLR had higher risk of mechanical complications of STEMI (23%) compared to those in low and intermediate groups (13%, 13%) (Fig. 2). Indeed, high NLR was independently associated with cardiovascular mortality, pericardial effusion and left ventricular thrombus during hospitalization.
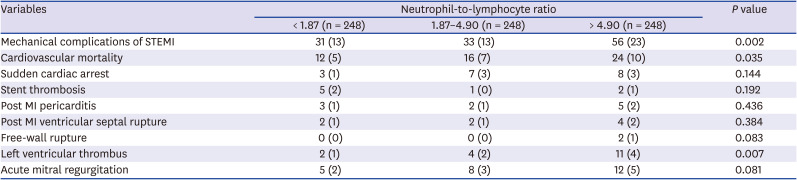
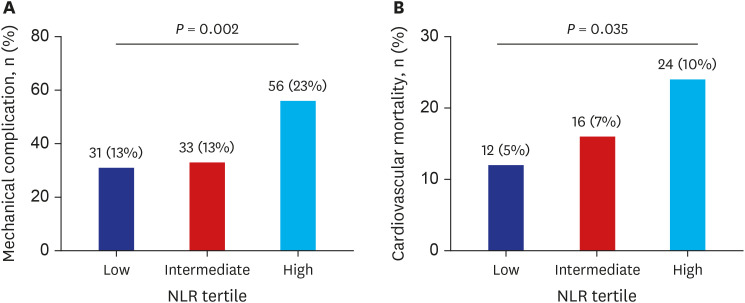 | Fig. 2Mechanical complication rate (A) and mortality rate (B) during hospitalization according to NLR tertiles.NLR = neutrophil-to-lymphocyte ratio.
|
Table 3
Mechanical complications of STEMI according to NLR tertiles
![]()
The independent predictors of mechanical complications of STEMI are presented in Table 4. Univariate logistic regression analyses revealed that NLR showed significant correlation mechanical complications of STEMI along with hs-CRP, left ventricular (LV) dysfunction, symptom-to-balloon time, pre-PCI TIMI flow grade 0, post-PCI TIMI flow grade 3 and no-reflow phenomenon. On multivariable analysis, NLR remained an independent predictors of mechanical complications of STEMI along with symptom-to-balloon time, and LV dysfunction.
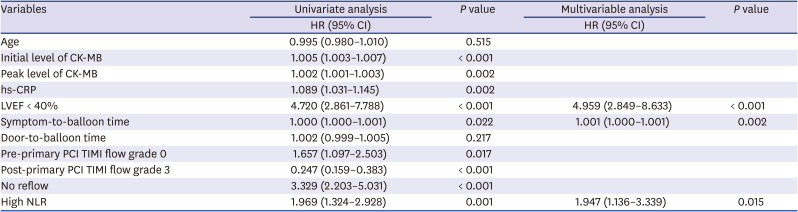
Table 4
Logistic regression analysis for mechanical complications of ST-elevation myocardial infarction
HR = hazard ratio, CI = confidence interval, CK-MB = creatine kinase myocardial band, hs-CRP = high-sensitivity C-reactive protein, LVEF = left ventricular ejection fraction, NLR = neutrophil-to-lymphocyte ratio, PCI = percutaneous coronary intervention, TIMI = thrombolysis in myocardial infarction.
![]()
Go to :
DISCUSSION
In this study we found that high NLR is related to higher rates of mechanical complications of STEMI undergoing primary PCI. Patients in the highest NLR tertile exhibited around two-fold increase in risk of in-hospital mechanical complications when compared with those in the low and intermediate tertile of NLR distribution. This association remained significant even after adjusting key predictors including age, initial and peak cardiac biomarkers, left ventricular dysfunction, pre- and post-primary PCI TIMI flow grade and no-reflow phenomenon.
The NLR is a combination of 2 independent markers of inflammation: neutrophils as a marker of the ongoing nonspecific inflammation through secretion of many inflammatory mediators and lymphocytes as a marker of the regulatory pathway of immune system.8 consequently, elevated NLR reflects both neutrophilia and relative lymphopenia. Mean NLR values of each tertiles were similar to that of other prior studies which reinforce the validity of our data.9 With growing understanding of the role of inflammation in the atherosclerotic process, many studies have demonstrated an association between elevated NLR and adverse clinical outcomes in patients with ACS undergoing PCI.
NLR was an independent predictor of long-term mortality.1011 but it was mainly due to increases in 3-day mortality. Núñez et al.12 reported that the major separation between Kaplan-Meier curves of top quintiles and lower quintiles of NLR was observed during the first months of follow-up for the long-term mortality. Park et al.8 showed that although 24-hour NLR was an independent predictor of long-term mortality, it was mainly due to increases in 30-day mortality, as demonstrated by the landmark analysis.
The association between high NLR and worse short-term outcomes in patients with ACS have been reported in recent years,1314 but little research has been made regarding the complications during hospitalization. Umesh et al. showed that NLR is an independent predictor of in-hospital mortality in patients with ACS.1 Machado et al.15 found that a low NLR has an excellent negative predictive value for in-hospital MACE (all-death, new MI, ST and stroke after primary PCI) in STEMI patients after primary PCI. Akpek et al.16 reported that the NLR is independently associated with in-hospital MACEs in patients with STEMI undergoing primary PCI.
Our result is in line with these studies. In addition to these results, we found that the NLR at ER is a predictor of mechanical complications of STEMI undergoing PCI.
Although the NLR was an independent predictor of mechanical complications of STEMI, it was primarily due to increased death rate, which is considered as one of the most important mechanical complication. In addition, we confirmed by logistic regression analysis, the prognostic role of NLR, predicting complicated STEMI except for death (hazard ratio, 1.842; 95% confidence interval, 1.063–3.192, P = 0.029).
Interestingly, the hs-CRP at ER was not an independent risk factor for mechanical complications of STEMI. This is probably due to the fact that initial hs-CRP taken at ER does not fully represent myocardial necrosis and infarct size since they are time dependent. Had it been peak hs-CRP level, it would have mirrored infarct size more accurately.17 Furthermore, Smit et al.18 was able to demonstrate that elevated CRP level was a poor prognosticator with respect to re-infarction and mortality. However, final logistic regression model devised to predict infarct size after adjusting for age, gender, CRP, baseline WBC count and hypotension showed that baseline WBC and hypotension were the only independent prognosticators.
Delayed symptom-to-balloon time could affect myocardial perfusion and mortality in patients with STEMI who had undergone primary PCI.19 In addition, we have previously shown that symptom onset-to-balloon time was significantly longer in the high NLR group in patients with STEMI undergoing primary PCI.20 Chia et al.13 demonstrated that elevated neutrophil counts after primary PCI in patients with STEMI are directly related to myocardial infarct size and the left ventricular ejection fraction (LVEF). Our data also showed that NLR was correlated to symptom-to-balloon time, cardiac enzymatic biomarkers, LVEF and wall motion score index. Taking all of these factors into account, the NLR could reflect the extent of myocardial damage and might explain at least part of the correlation between NLR and mechanical complications of STEMI.
Early risk stratification is important in managing STEMI patients. It informs decisions regarding pharmacologic and interventional treatment, allocation of clinical resources, and triage of alternative levels of hospital care.2122
Our current study provides a clinical tendency of NLR; patients with high NLR have almost two-fold risk for mechanical complications of STEMI and should receive prompt and more intensive treatment as well as risk factor modification.
This study has several limitations. The study was designed as a single-center retrospective trial. Thus, although we performed adjustment for significant clinical variables, the possibility of selection and confounding bias cannot be completely excluded. Despite these limitations, this is the first study to demonstrate the correlation between NLR at ER and mechanical complications of STEMI undergoing primary PCI.
In summary, NLR at ER is an independent predictor of mechanical complications of STEMI undergoing primary PCI. STEMI patients with high NLR are at increased risk for complications during hospitalization, therefore, needs more intensive treatment after PCI.
Go to :
 XML Download
XML Download