

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Smartphones are indispensable tools for people of all ages around the world today, and it has become difficult to imagine everyday life without a smartphone. Smartphone use has been changing daily routines, habits, social behaviors, emancipative values, family relationships, and social interactions.1 For adolescents, who are particularly sensitive to new technology and media use, smartphones have become an important part of their lives.2 According to a recent study, the domestic middle and high school students' smartphone ownership rate exceeded 95%, which is about 8% higher than that of all age groups (87.2%).3 Adolescents are more susceptible to smartphone addiction than adults, which can be attributed to the former's use of various contents for interaction with peers and entertainment through their smartphones4 and their neurobiological vulnerability, as discussed in dual processing theory.56 A domestic study reported that the smartphone overdependence (addiction) prevalence rate of adolescents was 30.2%, which is higher than that of adults, at 18.8%.7
Smartphones are used for a variety of purposes, including learning, information search, social communication, and entertainment.8 Compared to traditional types of computers, the portability and connectivity of smartphones allow users to easily access information anytime and anywhere. Therefore, users who are vulnerable to behavioral addiction, such as adolescents, are more likely to develop an addiction to smartphones.9 Smartphone addiction is defined as a state involving the excessive use of a smartphone, with withdrawal symptoms of feeling anxious and nervous when without the smartphone. Higher tolerance to smartphone usage, which necessitates increased use to obtain the same level of satisfaction, is observed. Although these symptoms negatively affect the daily life of the person, they cannot control their use of the smartphone. Based on these characteristics, many researchers regard smartphone addiction as one of the behavioral addictions.1011
Previous studies reported that excessive smartphone use by adolescents is associated with their sex, health problems, psychopathological state (depression, anxiety, high stress, low mood, etc.), and behavioral problems.121314 This is because adolescents are easily affected by external stimuli, interpersonal problems, and emotional changes.2 Excessive smartphone use by adolescents can result in conflict with their parents, low academic achievement, and low satisfaction with life, leading to failure to perform developmental tasks and difficulties in adaptation.15 The focus of previous studies related to smartphone addiction has been on the characteristics of people who use smartphones excessively. These studies have been conducted to investigate smartphone users' addictive use of these devices, their side effects, and factors influencing smartphone addiction.1516 However, despite smartphones being used for various purposes, only a few studies focused on the relationship between usage types available for smartphones and smartphone addiction.1718
Jeong et al.14 suggested that more attention is needed to describe smartphone addiction, and that evaluating the role of usage types will help to understand the nature of smartphone addiction. Park and Hwang19 said that the addiction phenomenon of smartphones is closely related to the use of some applications and the media properties of applications. Smartphone usage types can be categorized into playing games, social network service (SNS), news reading, entertainment (music/videos), exchanging text messages, making and receiving calls, commercial transactions, and location-based services.19 Most of the preceding studies have been conducted on the relationship between smartphone use for playing games and SNS and smartphone addiction. However, no prior studies have been conducted in comparison with other key variables that predict usage types and smartphone addiction. Therefore, we aim to investigate the types of smartphone use and the impact of major variables predicting smartphone addiction based on the classification of smartphone usage by Jeong et al.14
Representative variables which explain smartphone addiction were selected as personal psychological factors, home environmental factors, social environmental factors, and technical factors presented by the National Information Society Agency.20 First, the individual psychological factors were depression and ADHD. According to a study of adolescent smartphone addicts visiting outpatients of psychiatry in Korea, many had symptoms of depression and ADHD.21 Depression has a significant impact on smartphone addiction,2223 and teenagers are known to be addicted to avoid negative emotions such as depression.24 In addition, 40% of ADHD patients were smartphone addicts and were more susceptible to addiction due to poor attention and inhibition.25 The parenting attitude of parents was selected among the family environment factors.26 Among the various variables that affect adolescents' smartphone addiction, those related to family issues were found to have the strongest influence because the parenting attitude of parents considerably influences adolescents whose independence as adults is delayed.2728 Of the social environment factors, interpersonal problems and stress were selected.2930 Recent studies reported that interpersonal problems have a positive effect on smartphone addiction.31 This is because adolescence is an important period in which a person prepares for adulthood by developing a healthy self-concept and acquiring various social skills.32 With regard to stress, teenagers avoid psychological conflicts and worries because they are not as good at dealing with stress as adults, or easily concentrate on using smartphones.33 Finally, the type of smartphone use was selected as a technical factor, and we will look at the connection with smartphone addiction with the key variables mentioned earlier.
Therefore, this study aimed to identify two things regarding the use of smartphones by adolescents. We investigated the relationship between smartphone usage types and smartphone addiction. Also, we investigated the effect of smartphone usage types on smartphone addiction when controlling the main predictive factor of smartphone addiction, and attempted to find out how each smartphone usage types affect to smartphone addiction.
Go to : 
METHODS
Participants
We surveyed a total of 487 middle school students, of which 253 were girls and 234 were boys in a region after requesting cooperation from the middle school.
Assessment
Smartphone addiction scale
A youth smartphone addiction self-diagnosis scale developed by the National Information Society Agency was used in this study.34 The 15 items of this scale are divided into four sub-factor categories as follows: 5 items on daily life disorders regarding difficulties in daily life due to excessive smartphone use, 2 items on the pursuit of the virtual world regarding a tendency to cling to the virtual world as it provides more enjoyment than the real world, 4 items on withdrawal symptoms of anxiety and nervousness when not using the smartphone and 4 items on higher tolerance that causes increased use for a sense of satisfaction. The items are constructed based on a 4-point Likert scale.
If a testee receives a total score of 45 points or more, or meets all the conditions including 16 points or more in daily life disorders, 13 points or more in withdrawal symptoms, or 14 points or more intolerance, the person is classified as a high-risk user. Testees who obtain a total score of 42 points or more to 44 points or less, or satisfy any of the following conditions–14 points or more in daily life disorders, 12 points or more in withdrawal symptoms, and 13 points or more intolerance–they are classified as potential risk users, whereas the rest are classified as general users. The overall scale reliability Cronbach's α value as reported by the developers was 0.88, and Cronbach's α in this study 'was 0.89.
Smartphone usage type scale
The smartphone usage type scale used in the study by Jeong et al.14 was used after being modified to reflect the characteristics of the subjects and supplemented with more types. Whereas the existing study divided smartphone usage types into 1) study, 2) entertainment (music/videos), 3) SNS (focused on conversation and social interaction), and 4) games, in this research we added the following three types based on preceding studies1217: voice calls and text messages, which are the most basic functions of the smartphone; information search; and other (shopping, schedule management, alarms, public transportation use, etc.). In the case of SNS, some platforms such as YouTube and Facebook include the use of music and video content, such as the use of social media for conversation and social interaction, as in the existing study.17 The instruction “Some items regarding the purposes of the app (e.g., Facebook) use may be confusing as the stated purposes can also be considered its functions, but choose an answer that best reflects your main purpose for using the app” was added to the questionnaire, so that the study subjects could distinguish their SNS types. Therefore, this scale was finally constructed with the following seven usage types: 1) calls and text messages, 2) study, 3) information search, 4) music/videos, 5) SNS, 6) games, and 7) other (shopping, schedule management, alarms, public transportation, etc.). Each item was structured on a 5-point Likert scale from “never use” to “use very often” to assess smartphone usage types.
Depression scale
The Korean version of the patient health questionnaire-9 (PHQ-9) developed by Kroenke et al.,35 which was standardized by An et al.,36 was used as a tool to provisionally diagnose depression. PHQ-9 is a self-report test designed to diagnose depression simply and assess the severity of the depression. The grades of depression indicated by each score range are as follows: “not depressive” by a score of 0–4 points, “mild depression” by a score of 5–9 points, “moderate depression” by a score of 10–14 points, “more than moderate depression” by a score of 15–19 points, and “severe depression” by a score of 20 points or more, which is a level at which treatment by a psychiatrist is required. Cronbach's α was 0.89 in the study by Kroenke et al.,35 0.95 in the domestic standardization study, and 0.87 in this study.34
ADHD scale
The Korean version of the attention-deficit hyperactivity disorder rating scale (K-ARS), which is a behavioral assessment scale for children developed by DuPaul et al.,37 was standardized for use in Korea by Kim et al.38 Designed to assess ADHD symptoms in school-age children, the scale has a high discriminant validity for discriminating between the ADHD patient group and the control group. Consisting of 18 questions, it is an efficient tool for distinguishing the three subtypes of ADHD (primarily inattentive, primarily hyperactive/impulsive, and combined). Cronbach's α was 0.90 in the study by DuPaul et al.,37 from 0.77 to 0.89 in the study by Kim et al.,38 and 0.92 in this study.
Parenting attitude scale
The parenting attitude scale devised by Heo39 and modified by panel researchers with expertise in youth issues was used in this study. The original scale was composed of the sub-factors of the supervision, affection, inconsistency, excessive expectations, excessive interference, and rational explanation of parents. In this study, these sub-factors were divided into a positive parenting attitude (supervision, affection, and rational explanation) and a negative parenting attitude (inconsistency, excessive expectations, and excessive interference). In the study by Heo,39 the Cronbach's α values for each factor ranged from 0.68 to 0.86. In this study, the Cronbach's α value for the 10 items related to the three sub-factors of positive parenting attitude was 0.88, and that of the 11 items related to the three sub-factors of negative parenting attitude was 0.87.
Perceived stress scale (PSS)
The PSS developed by Cohen et al.40 and validated by Park and Seo41 for use in Korea was selected to measure stress. The PSS consists of 10 items that were constructed on a 5-point Likert scale with a score range from 10 to 50 points. The higher the score, the higher the perceived stress level. The reliability Cronbach's α value of the original tool was 0.75 and the Cronbach's α values for negative and positive perceptions were 0.77 and 0.74, respectively, in the study by Park and Seo.41 In this study, Cronbach's α was 0.81.
Interpersonal problem scale
The short form of the Korean-inventory of interpersonal problems circumplex scale (KIIP-SC) developed by Hong et al.42 was used in this study. The scale is composed of a total of 40 items and 8 sub-factors including a circumplex of personality, such as domineering, egocentric, cold, socially avoidant, nonassertive, overly-nurturing, self-sacrificing, and intrusive, with 5 questions for each sub-factor. This scale is based on a 5-point Likert scale; the higher the score, the more serious the interpersonal problem. In the study by Hong et al.42 Cronbach's α was found to range from 0.61 to 0.81, and that in this study ranged from 0.78 to 0.89.
Statistical analysis
Data analysis was performed using the Statistical Package for Social Sciences (SPSS/PC), version 15 (SPSS, Chicago, IL, USA), and the predictors of smartphone addiction were examined using correlation analysis and hierarchical multiple regression analysis.
Ethics statement
The Institutional Review Board of Dankook University permitted this study (DKU 2020-09-025). Informed written consents were provided by all participants before participation.
Go to :
RESULTS
Demographic characteristics of the study subjects
The final study subjects were 487 middle school students, of which 253 (52%) were female students and 234 (48%) were male students. Among the total students, 264 students (54.2%) were in the first grade, 113 (23.2%) in the second grade, and 110 (22.6%) in the third grade. Depending on the family's financial status, 55 of the total students were classified into the high-level group (11.3%), 418 into the mid-level group (85.8%), and 14 into the low-level group (2.9%). The mean and standard deviation of each measurement are as follows (Table 1).
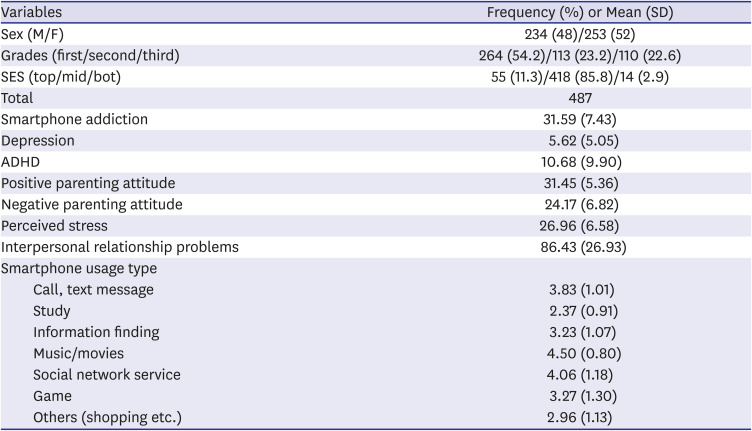
Table 1
Epidemiological characteristics of study subjects
SD = standard deviation, M = male, F = female, SES = socio-economic status, Smartphone addiction = a youth smartphone addiction self-diagnosis scale, Depression = the Korean version of the patient health questionnaire-9, ADHD = attention deficit hyperactivity disorde, Positive parenting attitude = parenting attitude scale devised by Heo, Negative parenting attitude = parenting attitude scale devised by Heo, Stress = the perceived stress scale, Interpersonal relationship problems = the short form of the Korean-inventory of interpersonal problems circumplex scale.
Smartphone usage type scale: call, text message, study, information finding, music/movies, social network service, game, others, shopping etc.
![]()
Correlation between smartphone addiction and related variables
Table 2 shows the correlation between smartphone addiction and sex, grade, financial status, smartphone usage type, depression, ADHD, positive parenting attitude, negative parenting attitude, stress, and interpersonal problem. Smartphone addiction was found to have a significant positive correlation (r = 0.09–0.39, P < 0.5) with all variables except for financial status and the three usage types including calls/text messages, information search, and games among the variables used in the study. We also found a negative correlation (r = −0.11 to 0.21, P < 0.5) between smartphone addiction and the two variables study and positive parenting attitude (Table 2).
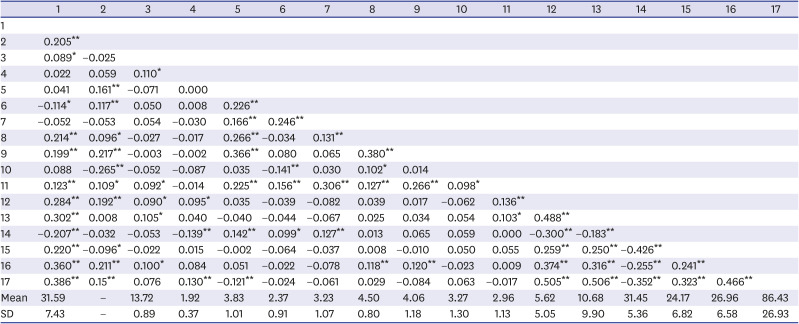
Table 2
Correlation between smartphone addiction and related variables
![]()
A hierarchical multiple regression analysis among variables influencing smartphone addiction
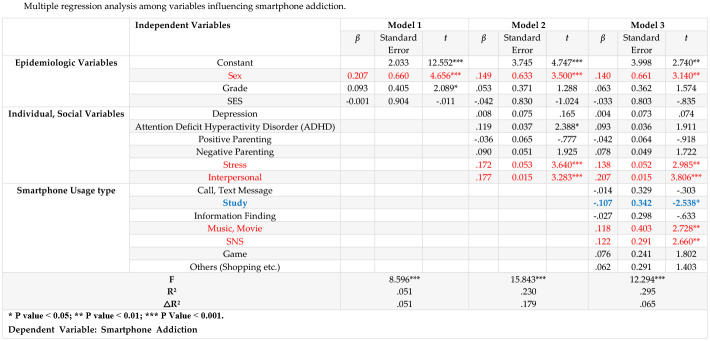
Smartphone was set as dependent variables, and Epidemiologic variables, individual and social variables, and smartphone usage types were used as independent variables. A hierarchical multiple regression analysis was performed to determine whether smartphone usage types have a significant additional explanatory power for smartphone addiction (Table 3).
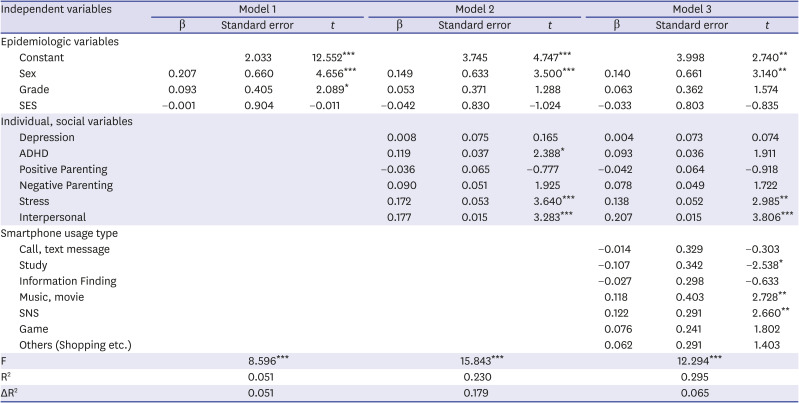
Table 3
Multiple regression analysis among variables influencing smartphone addiction
SES = socio-economic status, ADHD = attention deficit hyperactivity disorder, SNS = social network service.
*P < 0.05; **P < 0.01; ***P < 0.001.
Dependent variable: smartphone addiction.
![]()
First, in Model 1, in which demographic variables were measured, we found that sex (β = 0.207) and grade (β = 0.093) had a statistically significant effect on smartphone addiction (F = 8.596, P < 0.001). In Model 2, depression, ADHD, positive and negative parenting attitudes of parents, stress, and interpersonal problems were added to the demographic variables of Model 1, and sex (β = 0.140), ADHD (β = 0.119), stress (β = 0.172), and interpersonal problems (β = 0.177) showed a positive significant effect (F = 15.843, P < 0.001). The explanatory power of Model 2 was 23%, which was 17.9% higher than that of Model 1. The grade (β = 0.053), which was significant in Model 1, was excluded from Model 2.
Finally, in Model 3, the smartphone usage type was added to the variables of Model 2 (F = 12.294, P < 0.001). Sex (β = 0.140), stress (β = 0.138), interpersonal problems (β = 0.207), and the usage type of study (β = –0.107) had a negatively significant effect, while the usage type of music/videos (β = 0.118) and the usage type of SNS (β = 0.122) were found to have a positive significant effect. The explanatory power of Model 3 was 29.5%, which was 6.5% higher than that of Model 2. ADHD (β = 0.093), which was significant in Model 2, was excluded from Model 3. The results suggested that the level of smartphone addiction is higher among girls, and with the following: higher stress, more serious interpersonal problems, less use of the smartphone for study, more time spent enjoying music and videos, and more use of social media.
Go to :
DISCUSSION
We investigated the relationship between user characteristics, personal psychological factors, home, and social environment characteristics, and smartphone usage types, which may be predictors of individual smartphone addiction. The results showed that in terms of smartphone usage types, music/videos and social media use had a positive relationship with smartphone addiction, whereas the usage type study showed a negative relationship. Additionally, the contents that affect smartphone addiction were identified as music/videos, social media, and study, in descending order. Games did not show any relationship with smartphone addiction in adolescents, contrary to the results of previous studies. And leading variables showed that in female students, interpersonal problems and stress were positively associated with smartphone addiction.
Among the smartphone usage types, SNS and music/videos positively predicted smartphone addiction. This result is consistent with previous research findings that the use of social media is a predictor of smartphone addiction41443; enjoying music/videos is also a positive predictor of smartphone addiction.1444 We classified smartphone usage types into social media use and music/videos. In the case of YouTube and Facebook, however, these platforms combined their function related to the formation of social relationships, which is intrinsic to social media and other various functions related to music/videos. Since the two factors that influence smartphone addiction are combined in a complex manner in the two platforms, further exploration of their influence is needed.
Study, as a smartphone usage type, was found to negatively influence smartphone addiction. This is consistent with the results of a previous study that found that smartphone applications intended for user convenience, such as educational programs/dictionaries, have a negative effect on smartphone addiction.19 This suggests that training students on how to use smartphone content in a balanced manner through an educational approach can help prevent smartphone addiction in the future. The results of this study on the relationship between smartphone addiction and games were not consistent with those of previous studies, which reported that games had a positive effect on smartphone addiction.414 Lee et al.10 reported that smartphone usage types differ according to age and sex. The subjects of this study were middle school students, whereas those of previous studies414 were elementary school students in the fourth to sixth grades. According to the smartphone application use rates in 2018, the use rate of game apps (38.3%) was the highest in elementary school and higher grades, followed by the use rate of instant messenger apps (17.9%). In contrast, the most frequently used apps by middle school students were instant messenger apps (24.3%), followed by game apps (20.1%). These results suggest that smartphone usage patterns differ depending on the grade.3 Higher grades of elementary school are in the stage of “industry vs. inferiority” according to Erikson's psychological development theory, and experiencing a sense of accomplishment by making efforts has an important influence on them. As many of the smartphone games are designed for single players rather than for group players, it seems that smartphone games stimulate a sense of accomplishment in higher grades of elementary school, engrossing them in these games.
As middle school students are in a stage of “identity vs. role confusion” that characterizes adolescence, peer relationships are important to them. Therefore, they seek to be part of a community where they can share culture and play together with their peers rather than engaging in smartphone games that are relatively more focused on a single play. Therefore, computer games in computer cafes where they can interact with their peer community are more preferred by adolescents to smartphone games. This suggests that research on which platform each age group mainly plays games with their developmental age is also necessary.
Similar to the results of previous studies on smartphone addiction and sex,1345 we found that female students are more likely to be addicted to smartphones. Lin and Chiang13 reported that young women use smartphones to communicate, maintain relationships, achieve socialization, and find information and entertainment. Female users have a strong emotional attachment to these devices and can become dependent on them.13 In addition, women are under higher stress regarding the maintenance of social relationships than men, and such stress is more likely to lead to habitual and addictive smartphone-related behaviors.8 In line with the findings of previous studies on smartphone addiction and interpersonal problems,31 the presence of interpersonal problems was found to affect smartphone addiction in this study. Another study reported that students who are isolated and evasive in relationships with others show a compulsive addiction to smartphones. Those who are cold and closed in interpersonal relationships have a higher tendency to be addicted to smartphones.46 Those with a higher level of social discomfort, a lower level of social problem-solving ability, and more interpersonal problems were found to have a higher tendency to develop Internet addiction.47 Consistent with the results of previous studies on smartphone addiction and stress,1433 we found that the higher the stress, the stronger its influence on smartphone addiction. When adolescents face stress, they choose passive and superficial solutions rather than actively seeking solutions to the problems, and prefer cyberspaces with guaranteed anonymity and easy access as a space for releasing their stress.28
Depression, ADHD, and the parenting attitudes of parents showed a significant relationship with smartphone addiction. However, these correlations were not observed in the regression analysis. This suggested that interpersonal problems and stress can be stronger predictors of smartphone addiction than depression, ADHD, and parenting attitudes.
First, the subjects of this study were limited to middle school students in an area of North Chungcheong Province, Korea. Differences may exist in students' smartphone addiction levels according to regions, and smartphone addiction levels and usage types in one area cannot represent those in the entire region. Although this study was conducted on middle school students who are younger adolescents, there may be differences in smartphone usage types and levels depending on the developmental stage and adaptation levels of adolescents. In particular, high school students who are preparing for the college entrance exam may have different smartphone experiences from those of middle school students. Therefore, it will be necessary to consider the regional differences among study subjects and to extend the age range of the subjects in future studies. Second, we classified smartphone usage types based on previous studies comparing smartphone use types. The classification was specially performed by supplementing the types presented by Jeong et al.14 However, this approach has limits in classifying the various functions of smartphones simply by type. There were also limits in terms of how the study subjects' smartphone usage types are determined. That is, related items that are relatively simple and the evaluation of use frequency of each type based on a Likert scale suggest that the validity of this approach may be weak. In the future, a more elaborate scale should be developed to classify the types of smartphone usage. Third, since the measurement was carried out using the study subjects' responses based on their perception using a self-report questionnaire, the respondents' subjective interpretations may be included in the survey results. Therefore, there are limits on generalizing the results of this study, and follow-up studies that investigate the perspectives of parents and teachers are needed.
In Model 2 of hierarchical regression, ADHD appeared to be a significant variable for smartphone addiction, consistent with prior research, but did not significantly affect smartphone addiction in Model 3, where content types were added. In the case of depression, it is difficult to distinguish between depression and anxiety in adolescence. In fact, the strong relationship between anxiety and depression has already been reported in various studies.4849 Some scholars saw that anxiety and depression were on a continuous line and that anxiety preceded it.5051 This shows that perceived stress variables similar to anxiety are significant. Thus, in this study, perceived stress variables preceded depression, and mixed results appear to have been shown.
Despite these limitations, this study is important as it provides basic data for studies on smartphone addiction and usage types, as few studies have been conducted on these topics. Particularly with the rapid spread of smartphones, although studies on smartphone use and addiction have been actively conducted, there are relatively fewer studies on content related to the unique functions of smartphones, that is, smartphone applications that correspond to smartphone usage types. We focused on the types of smartphone usage and examined the relationship between these types and smartphone addiction to verify the significant differences in the levels of smartphone addiction according to these smartphone usage types when the variables predicting smartphone addiction are controlled. This suggests that selective intervention according to the main smartphone usage type can be effective in preventing addiction. Accordingly, further studies are needed on the relationship between smartphone usage types and smartphone addiction.
Go to :
 XML Download
XML Download