

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In the elderly population, hip fracture is a severe injury with high morbidity and mortality.1 Substantial efforts are needed and medical costs are incurred in restoring function in elderly patients with hip fractures.12 Expecting an increase in hip fracture patients in the future, medical and institutional efforts are being made to reduce social costs. Among these, proper pain control is important to reduce delays in ambulation and complications, and to shorten the length of hospital stay.3
Elderly patients with hip fracture often use various medications for underlying comorbidities and are less likely to use more drugs due to decline in organ functions, such as the liver and kidneys.4 Nevertheless, intravenous or oral medications, such as opioids and non-steroidal anti-inflammatory drugs (NSAIDs), are commonly used to control postoperative pain.
Opioids can cause side effects, such as dizziness, sedation, balance problems, vomiting, constipation, and respiratory depression. Long-term use can lead to physical dependence and tolerance, and worst case, to addiction.5 However, the use of opioids has been increasing because they are a favorable option in terms of pain control.6 There have been several reports on opioid use in elderly patients with hip fractures. In a Danish nationwide cohort study, the proportion of opioid users increased after hip fracture surgery, and 16.8% of preoperative non-opioid users reported using opioids even after one year.7 A small cohort study by Lindestrand et al.4 reported that the use of opioids was not related to mortality. A'Court et al.2 evaluated the relationship between opioid use and operative methods and Maiese et al.8 reported the cost to patients using opioids. Although these studies showed that the long-term use of opioids was not beneficial for patients, they did not analyze the effects of opioid use in the acute phase of hip fracture in elderly patients, and some of the studies were not conducted using representative big data.
Thus, the purpose of this study was to assess the use of opioids before and after hip fracture in elderly patients in order to determine the effect of opioid use on all-cause mortality, and to analyze how opioid use before fracture increased the risk of sustained use after hip fracture, using a nationwide cohort.
METHODS
Study subjects
Incident hip fracture patients in our retrospective observational cohort study were identified from the Korean National Health Insurance Service-Senior cohort (NHIS-Senior).9 NHIS-Senior consisted of 588,147 participants over 60 years of age (as of 2002) to represent elderly people in South Korea by simple 10% random sampling. All the individuals in the NHIS-Senior were followed until December 31, 2015, except those who were disqualified (emigration or death etc.). The NHIS has all personal information, such as medical utilization, demographics, and treatment information, for all Korean people.91011
Elderly hip fracture cohort
The inclusion criteria for elderly hip fracture patients were as follows3: 1) first-time admission to an acute care hospital with diagnostic codes of femoral neck fractures (International Classification of Diseases, 10th Revision [ICD-10] S720) or intertrochanteric fractures (ICD-10 S721)1213; 2) recipients of surgeries, including internal fixation (closed pinning [femur] and open reduction of a fractured extremity [femur]), hemiarthroplasty (hip), or total arthroplasty (hip); and 3) aged 65–99 years at the time of hip fracture to ensure the inclusion of osteoporotic hip fractures.13 To guarantee a one-year observation period, patients with hip fractures occurring less than 365 days before December 31, 2015 were excluded. Patients with their first hip fracture prior to December 31, 2004, were also excluded to ensure at least a 3-year hip fracture-free period. The last date of follow-up was defined as the date of death or December 31, 2015, whichever preceded. To identify opioid use during the acute phase, time zero (index date) was defined as 90 days after admission to an acute care hospital to fulfill the inclusion criteria for hip fractures in the elderly. Furthermore, to prevent immortal time bias, patients who died within 90 days after hip fracture were excluded from the study.
All-cause mortality
In the NHIS-Senior, each subject's unique de-identified number was linked to their vital statistics from the Korean National Statistical Office, including dates and causes of death.9 The dates of death were used to calculate survival periods.
Categorization by type of opioid and definition of opioid exposure
The opioids used were hydromorphone, morphine, dihydrocodeine, oxycodone, hydrocodone, codeine, fentanyl, pentazocine, pethidine, buprenorphine, nalbuphine, butorphanol, tapentadol, remifentanil, sufentanil and tramadol.71415 The opioids were classified into strong opioids (opioids other than tramadol) and tramadol.14 Patients who used both tramadol and strong opioids were classified as strong opioid users. Patients who had used opioids within six months before the hip fracture were defined as past users, and patients with no history of opioid use within six months before the hip fracture were defined as a past non-user. Patients who received opioids within three months after admission for hip fracture were defined as current users, and those who did not were defined as current non-users. The cumulative dose of current tramadol and strong opioid was calculated by adding the amount of dispensed defined daily doses (DDDs).16 To determine the sustained use of strong opioids and tramadol, their use was investigated during the period from 3-months to 1-year after hip fracture (sustained user).
The history of medication and use of antidiabetic, antihypertensive, anti-platelet agent, NSAIDs, steroids, COX-2 inhibitors, antidepressants, and benzodiazepines within 6-months before hip fracture and within 3-months after admission for hip fracture were investigated.
Statistical analysis
Demographics were identified at the time of admission. Survival time was defined in days as the period from the index date (at 90-days after admission) to the date of December 31, 2015 or death, whichever preceded. Patients who died during the 90-day landmark period were excluded. A multivariable-adjusted Cox proportional hazard model was used to investigate the effects of tramadol and strong opioid use on all-cause mortality. The effect sizes are presented as hazard ratios (HRs) and 95% confidence intervals (CIs). A generalized estimating equation model with a Poisson distribution and logarithmic link function was used to estimate the adjusted rate ratios (aRRs) and 95% CIs to assess the association between past use and sustained use. The potential confounders included age group, gender, household income level, residential area, Charlson Comorbidity Score (CCS), type of fracture, surgery and anesthesia, calendar year of the hip fracture incidence, presence of transfusions, medication history, and recent medication use, which included strong opioids and tramadol. Quan's ICD-10 coding algorithm of the CCS diagnostic codes during the 3 years before admission for hip fracture was used to assess each subject's comorbidities.17 The presence of CCS disease-constituting categories was calculated by the presence of at least 2 outpatient visits or 1 admission for primary or first secondary diagnosis. Statistical analyses were conducted using SAS Enterprise Guide version 7.1 (SAS Institute, Cary, NC, USA). Statistical significance was set at P < 0.05.
RESULTS
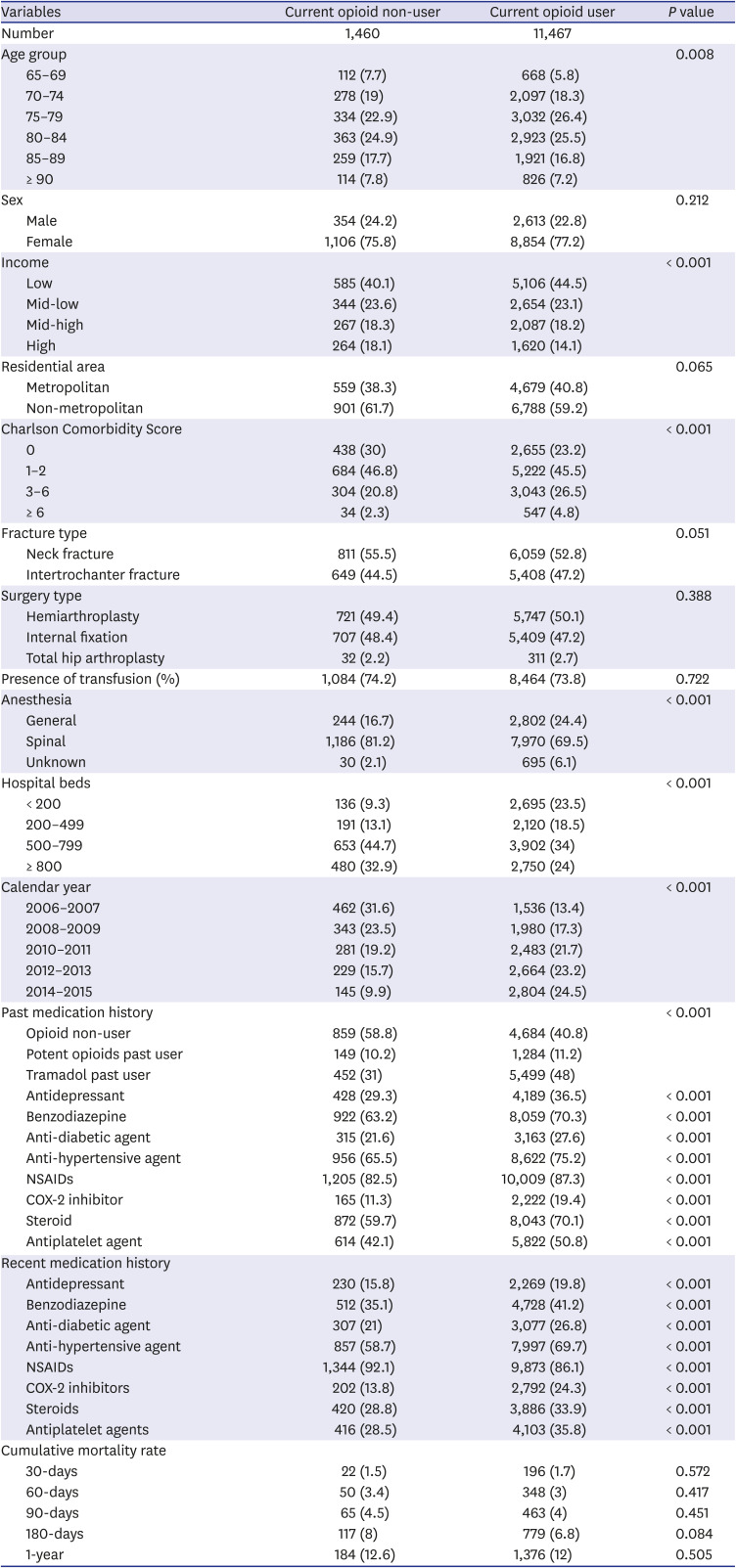
Between January 1st, 2002, and December 31st, 2015, 19,915 patients with hip fractures were identified. Among these patients, 1,478 patients did not undergo surgery and 3,571 patients were excluded for not meeting the eligible criteria. In addition, 921 patients with a history of neoplasms and 1,018 patients who died within 90-days of hip fracture were excluded. Ultimately, 12,927 patients were included in our study (Fig. 1). The patient demographics and medication history and recent medication use are presented in Table 1. There were no significant differences in the cumulative mortality rates between the two groups (P < 0.05).
Fig. 1
Flowchart for the selection of the study subjects.
NHIS-Senior = Korean National Health Insurance Service-Senior cohort.
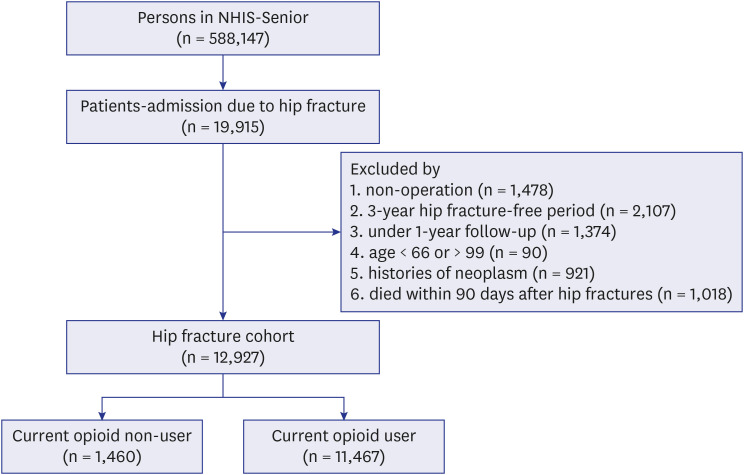
Table 1
Demographics and medication histories and crude mortality rate according to current use of opioid
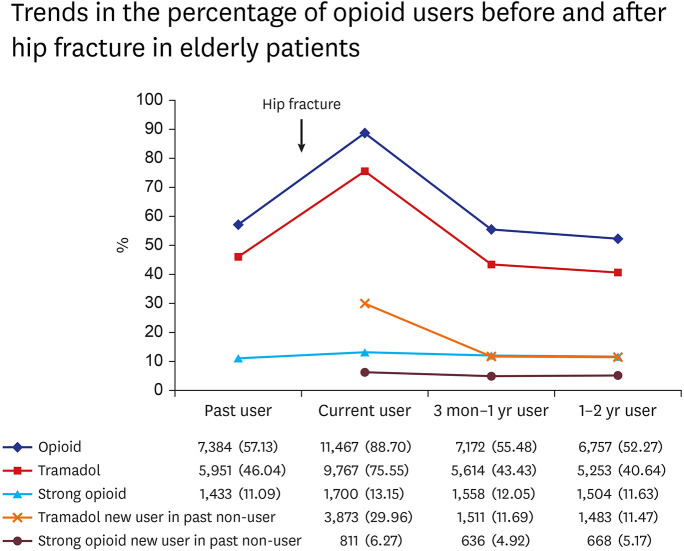
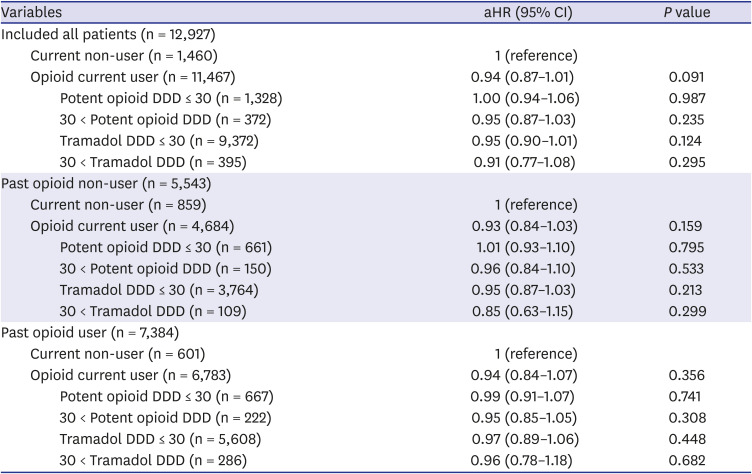
There were 7,384 (57.12%) opioid past users (5,951 [46.04%] tramadol past users, and 1,433 [11.09%] strong opioids past users) (Fig. 1). The number of opioid current users increased to 11,467 (88.71%) after hip fracture, with the number of tramadol and strong opioid current users being 9,767 (75.56%) and 1,700 (13.15%), respectively. The number of patients with a sustained use of opioids decreased to 7,172 (55.48%) patients. The proportion of strong opioid and tramadol current users increased in comparison to the proportion of past users in both categories, respectively. However, there was a greater increase in the number of tramadol current users than in strong opioid current users. The proportion of sustained users decreased to a level similar to that of past users, when compared to the proportion of current users (Fig. 2). The number of new users of tramadol and strong opioids among past non-users also increased after hip fracture. Moreover, the proportion of sustained users among new opioid users in the past non-user group decreased after one year. On death risk comparison according to current use and the DDD of strong opioids and tramadol in each patient group according to past opioid use, there were no significant differences in the adjusted HR compared to the current non-users in all groups (P > 0.05) (Table 2).
Fig. 2
Trends in the percentage of opioid users before and after fracture in older patients with hip fractures.
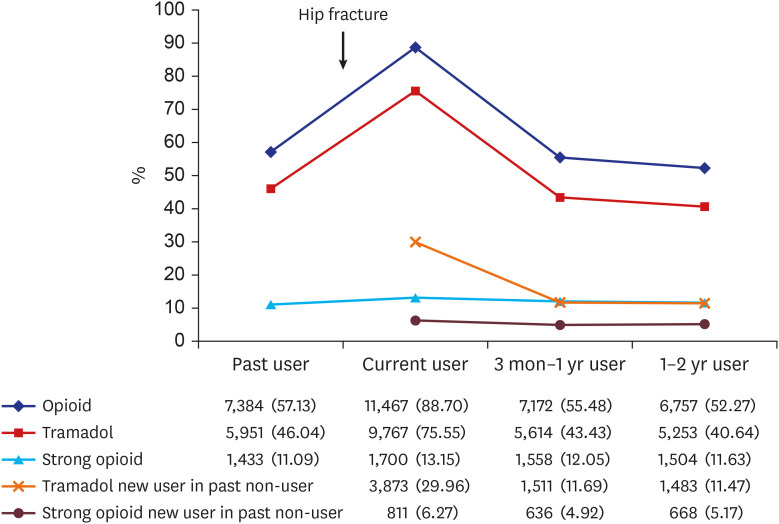
Table 2
Comparison of hazard for death according to current use and DDD of opioid in each patient group according to the presence of past opioid use
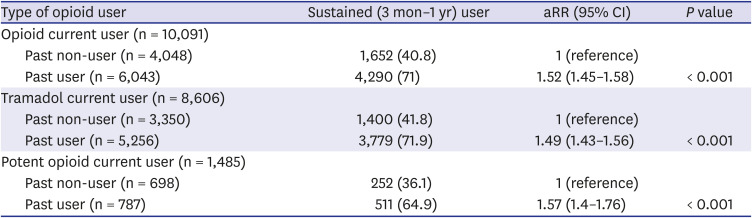
Among those who survived up to one year after hip fracture (1,376 patients died before 1-year after hip fracture), opioid past-use increased the risk of opioid sustained use by 1.52-fold (aRR; 95% CI, 1.45–1.8; P < 0.001). Tramadol and strong opioid past-use in current users increased the risk of a sustained use of tramadol and strong opioid by 1.49-fold (aRR; 95% CI, 1.43–1.56; P < 0.001) and 1.57-fold (aRR; 95% CI, 1.4–1.76; P < 0.001), respectively, compared to past non-users (Table 3).
Table 3
In the opioid current user, the relationship between past user and sustained user of opioid in survivors until 1 year after hip fracture
DISCUSSION
The main findings of this study are as follows. First, the current and past use of opioids did not increase all-cause mortality after hip fractures in elderly patients. Second, the opioid prescription rate increased rapidly within three months after hip fracture compared to before the hip fracture, but decreased three months after hip fracture. Third, current users with a history of opioid use had a higher risk of sustained opioid use compared to those who did not.
In 1995, the American Pain Society reported pain as a fifth vital sign that should be treated appropriately.18 This change in the concept of drug prescriptions for pain control increased the prescription of opioids, resulting in increased patient satisfaction. Since then, opioids have become an essential component of multimodal postoperative analgesia and are still widely used.19 However, this trend has led to opioid abuse for chronic musculoskeletal pain in the United States and Europe, and has emerged as a social problem.2021 Birke et al.20 reported that the use of opioids for non-cancer pain in a Danish population was highest in those aged 65 years and older. Several studies have shown that the side effects of opioids, such as cognitive impairment, dizziness, addiction, mortality, increased fall and fracture risk, are more likely to occur in elderly patients.2223 Paradoxically, insufficient pain control can lead to delirium, day-night inversion, and depression.2
Opioid-related deaths are among the most frequent types of drug-related deaths.24 Summers et al.25 reported that hip fracture patients with opioid use disorders had higher mortality rates than hip fracture patients with non-opioid use disorders. Patients with opioid use disorder had more comorbidities than those who did not. Therefore, they should be distinguished from patients with a history of opioid use. Lindestrand et al.4 investigated the use of opioids in patients with hip fractures and the potential relationship between the perioperative prescription of opioids, mortality, and chronic opioid use. In their study, the 30-day mortality rate was 10% and 1-year mortality rate was 27%. They found that mortality was associated with old age and increased comorbidities, but was not associated with opioid use. Therefore, they suggested that there was no general reason to refrain from prescribing opioids to hip fracture patients based on a fear of increased mortality. Our results are consistent with these findings. Tramadol has a lower analgesic potency than strong opioids, but is relatively safer due to a lower risk of respiratory depression and addiction.26 Therefore, we expected that all-cause mortality would be higher in the group using potent opioids at follow-up in both groups. However, neither tramadol nor strong opioids increased all-cause mortality. In addition, we found that opioid use before and after hip fracture did not contribute to increased mortality. Our study also showed that there was no increase in mortality even in groups taking high opioid doses after hip fracture, when compared to the non-user group. In elderly patients, the combination of several drugs is an important issue, and there are reports that the combination of central nervous system active drugs, including benzodiazepines and tricyclic antidepressants, with opioids can increase mortality.2728 However, our study found that opioids, after adjusting for several other drugs, including benzodiazepines and tricyclic antidepressants, did not significantly affect postoperative mortality.
Most recently, a large epidemiological study on opioid use after hip fracture surgery was published in Denmark. The authors performed a cohort study that included all patients (65 years old and over) who underwent hip fracture surgery (from 2005 to 2015), as selected from the Danish Multidisciplinary Hip Fracture Database.7 In their study, similar to the results of our study, the rate of opioid users increased rapidly after hip fracture and then decreased. They also found that the proportion of opioid users increased after hip fracture surgery and increased by 1.4% in the fourth quarter compared to before hip fracture. Of the opioid nonusers before surgery, 16.8% were opioid users in the fourth quarter after surgery. They suggested that opioid use at 1-year after surgery for hip fracture was common, both in patients who were opioid users and non-users before surgery. However, opioids are essential for postoperative pain control. In addition, depending on the degree of fracture reduction or the result of surgery, chronic pain or complications may persist, and pain control may be necessary. Therefore, it is necessary to detect and be aware of the risk of future abuse among patients who currently need opioids.
Simoni et al.7 reported that 8.3% of opioid non-users and 52.3% of opioid users before surgery used opioids one year after surgery. Morris and Mir29 also reported that pre-injury opioid users among orthopedic trauma patients had a high risk of postoperative opioid abuse. In addition, the use of preoperative opioids among orthopedic patients has been reported to cause poor clinical outcomes and increase the risk of reoperation.3031 We also found that among the current opioid users within three months after fracture, patients with a history of opioid use within six months prior to the fracture had a higher risk of sustained opioid use. This finding is in agreement with the results of a study that reported that preoperative opioid experience could increase the likelihood of opioid abuse.32 This may be due to dependence of past opioid use or opioid-induced hyperalgesia, making it difficult to discontinue opioids.33 Thus, before opioids are used after hip fracture surgery, a history of opioid use before the fracture should be carefully noted. Furthermore, for past opioid users, care should be taken not to prescribe opioids for a long period of time. In addition, it is necessary to follow-up to assess dependence or addiction in patients using opioids after surgery.
This study has several limitations. First, there was no analysis of functional or pain scores for hip fracture treatment. Therefore, there was no analysis of the effect of opioids on functional aspects or pain control. Second, since this study was solely based on a South Korean database, it may have had potential biases, such as regional and cultural biases. Spain and Sweden are both European countries, but the rate of opioid use before hip fracture was different between the two countries. As such, the guidelines for opioid use and medical systems are different in each country.4 However, this study compared the relative risk of mortality and the sustained use of opioids between subgroups. Third, our study did not define addiction. Drug addiction is not simply defined by dosage, but various factors such as dependence must be considered. Fourth, the specific cause of death could not be analyzed because of inherent limitations in the claims database.
In conclusion, the current use and past use of opioids did not increase all-cause mortality after hip fracture in elderly patients over 65 years of age. In current opioid users, past use of opioids before hip fracture increased the risk of sustained use of opioids compared to those without.
 XML Download
XML Download