

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since the first case of novel coronavirus disease 2019 (COVID-19) was reported in China on December 28, 2019, it has spread rapidly around the world.12 According to World Health Organization (WHO) report, by June 29, a total of 10,021,401 people were infected, and 499,913 people had died.3 Global public health is facing a crisis according to WHO definitions,4 and 160,000 new confirmed cases are reported worldwide a day. To mitigate the public health crisis caused by infectious diseases, WHO promotes cross-sectoral linkages and cross-governmental and cross-social integration through the Emergency and Disaster Risk Management for Health guidelines.5
The government response system for the public health crisis is different between countries. There are organizations in charge of crisis management for infectious diseases in each country, and several countries have implemented policies, including social or physical distancing, traffic restrictions, closure of schools and workplaces, or lockdown to prevent person-to-person transmission of COVID-19 and to reduce the burden of pandemic disasters.67 Regarding emergency care, most symptomatic and asymptomatic infected patients can primarily use emergency medical services (EMS). There is a need to isolate infected patients and appropriate emergency care in a timely manner, and it is also important to protect other noninfected emergency patients from infection and to provide adequate treatment according to acuity in disaster situations.891011 Therefore, the importance of the EMS system has become more prominent in pandemic disaster situations to protect the safety of society.12 Several countries have published emergency care-related health policies, such as designating centers for exclusive COVID-19 treatment.13 In Korea, the Ministry of Health and Welfare (MoHW) and National Emergency Medical Center (NEMC) implemented emergency care-related policies to respond to the COVID-19 pandemic.
The purpose of this study was to review nationwide emergency care-related health policies during the COVID-19 pandemic disaster in Korea and to analyze the effects of national emergency care-related policies on the safety of patients who visit emergency departments (EDs) during this period.
METHODS
Study design and data source
This study is a quasi-experimental study that consists of a review of emergency care-related health policies (natural experiments) and a before-and-after design to evaluate the effects of emergency care-related health policies on clinical outcomes for emergency patients during the COVID-19 pandemic.
The study period was classified into 5 phases according to the level of national crisis warning of infectious disease and the implementation of emergency care-related health policies: warning level 1 (Attention) and 2 (Caution) period (study phase 1: December 31, 2019 to January 26, 2020, for 27 days), warning level 3 (Alert) period (study phase 2: January 27 to February 22, 2020, for 27 days), warning level 4 (Serious) and preintervention (study phase 3: February 23 to March 20, 2020, for 27 days), warning level 4 (Serious) and run-in-intervention (study phase 4: March 21 to April 16, 2020, for 27 days), and warning level 4 (Serious) and postintervention (study phase 5: April 17 to May 13, 2020, for 27 days). National crisis warning levels and related health policies during the COVID-19 pandemic are described in Supplementary Data 1.
The National Emergency Department Information System (NEDIS) database was established to measure emergency care qualities and to provide evidence for developing national and federal emergency care policy in 2003. The NEDIS data collected from all 402 nationwide EDs in real time included demographics (such as gender, age, and insurance), symptoms (chief complaints and onset), prehospital (EMS use and treatment and means of transportation), and ED hospital (level of consciousness at presentation, emergency operative procedures, critical care requirement, disposition, hospital stay after admission and final clinical outcomes) information. For data quality management, the NEDIS data should be approved annually by Statistics Korea. NEMC, an administrative agency under the MoHW, is designated as an organization for managing the NEDIS data in accordance with Article 25 of the Emergency Medical Services Act.
Study population
The study population was defined as patients who visited all 402 emergency medical institutions in Korea between December 31, 2019, and May 13, 2020. Patients who visited the ED for nonmedical purposes, such as issuing a medical certificate, were excluded. Cases who were classified as dead on arrival were also excluded.
Study setting
Korea has a tax-based public EMS system operated by the National Fire Agency. Qualified emergency medical technicians provide necessary prehospital emergency care to patients. There were standard operation protocols for 4 major emergency conditions: out-of-hospital cardiac arrest, severe trauma, acute myocardial infarction (AMI), and acute stroke. During the COVID-19 outbreak, the critical protocol for patients with fever (≥ 37.5°C) conditions was added.
The MoHW in Korea designed 3 levels of ED according to emergency medical resources and capabilities (including facilities, equipment, and medical staffs) and operated 38 Level 1 EDs, 125 Level 2 EDs, and 239 Level 3 EDs (a total of 402 EDs) in June 2020. A Level 1 ED is designed to accommodate and to provide definite care to serious and severe emergency patients and to prepare and respond to disasters and mass casualty incidents. Level 1 EDs should designate special areas for isolation rooms, areas for severe and acute patients, and areas for pediatric patients. Before this pandemic, there were no standards of isolation beds for the level 2 and level 3 EDs.
The Central Accident Countermeasures Headquarters under the Ministry of Public Administration and Security is in charge of national disaster response in accordance with Article 14 of the Framework Act on the Management of Disasters and Safety. In the case of infectious disease, the Korea Disease Control and Prevention Agency responds to a national crisis warning in accordance with Article 38(2) of the Framework Act on the Management of Disasters and Safety.
National crisis warning level and emergency care-related health policies
On December 31, 2019, a total of 27 cases of unexplained pneumonia were reported in Wuhan, China, and the Korean government started the infection monitoring and surveillance response system (Crisis warning level 1 [Attention], study phase 1). The first COVID-19 case in Korea was confirmed on January 20, 2020 (Crisis warning level 2 [Caution], study phase 1). With the occurrence of 4 additional confirmed cases on January 27, 2020, the crisis warning level for infectious diseases was raised (Crisis warning level 3 [Alert], study phase 2). The quarantine of Korean immigrants began, and 288 medical centers operated separate COVID-19 screening stations (46 healthcare centers and 242 hospitals). Since some community infections had been identified, the level of national crisis warning had also been raised to the highest level to prevent the spread of COVID-19 infection nationwide on February 23, 2020 (Crisis warning level 4 [Serious] and national emergency care-related policies: preintervention, study phase 3).
Regarding emergency care, there were several shut-down events of the EDs because COVID-19 confirmed cases were detected among the patients admitted to the emergency room with the spread of the COVID-19 pandemic. It became necessary to designate EDs that could manage and treat suspected COVID-19 patients since the emergency care of patients with fever was delayed and the safety of patients was threatened. The MoHW and NEMC established the criteria for the designation of the Severe Emergency Medical Care Centers (SEMC) to treat appropriately suspected and confirmed COVID-19 patients with severe symptoms, to protect other uninfected emergency patients from infection and to provide appropriate care based on their severity; 5 or more isolation rooms with/without negative pressure, separate air-conditioning facilities, isolated areas for febrile patients, and designated triage areas in front of the emergency room. Of these level 1 and 2 EDs, 57 EDs were designated as the SEMC sequentially from Mar 21 to Apr 16, 2020 (Crisis warning level 4 [Serious] and the national emergency care-related policies: run-in-intervention, study phase 4). A total of 57 SEMC were operated since April 17, 2020. The number of isolation units increased from 1,558 to 1,700 after designation of the SEMC, and 49.2% (837 among 1,700) of isolation units belonged to the SEMC. In addition, the information on resources, including available isolation units and beds for suspected patients in the SEMC, was shared in real time through the web-based national emergency care information system (crisis warning level 4 [Serious] and the national emergency care-related policies: postintervention, study phase 5). Emergency care-related health policies during the COVID-19 pandemic are described in Table 1 and Supplementary Data 2.
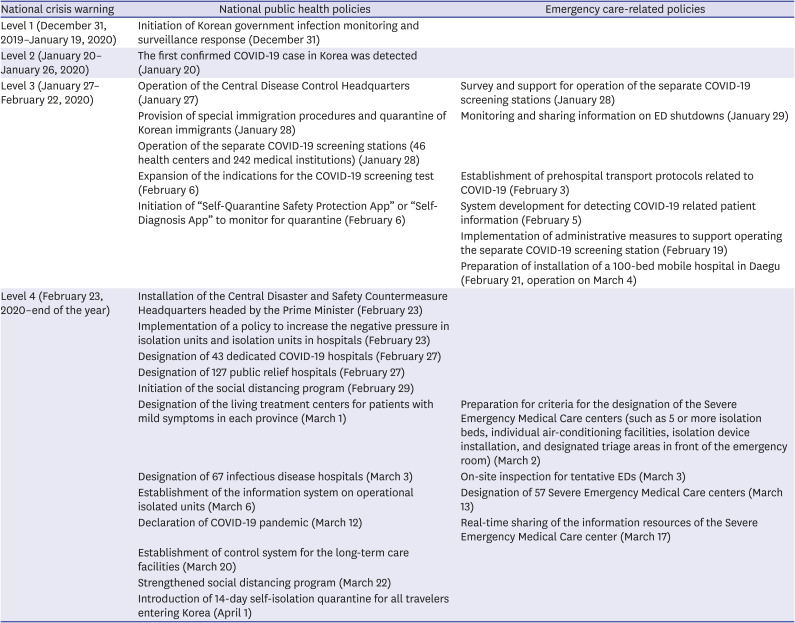
Table 1
The implementation of the policy by crisis alert level
![]()
Outcome variables and statistics
The primary outcome was in-hospital mortality, and the secondary outcome was length of stay (LOS) in the ED during the COVID-19 outbreak. In-hospital mortality was defined as death at the time of discharge from the ED or hospital and did not include hopeless discharge.
Study subgroups were defined as emergency patients with clinically important diagnoses at discharge from the ED and/or hospital among those who visited the ED within 7 days from the onset of the symptoms and who were aged 15 years old or older; AMI included I21.0–I21.9; acute ischemic stroke included I63.0–I63.9; acute hemorrhagic stroke included I60.0–I62.9; severe trauma included any S or T code and ICD-derived injury severity score less than 0.9.14
The characteristics and outcomes of the study population and subgroups were compared by study phase. The descriptive analysis for the study subject was compared using univariate analysis. The χ2 test for categorical variables and the Wilcoxon signed-rank test method for nonnormally distributed continuous variables were used.
Multivariable logistic regression analysis and general linear models were conducted to evaluate the effects of the study phase on study outcomes. Adjusted odds ratios (aORs) with 95% confidence intervals (CIs) were calculated for in-hospital mortality, and beta coefficients and 95% CIs were calculated for ED LOS.
Regarding the regional variation of COVID-19 outbreak, the subgroup analyses were conducted for 1) Daegu Metropolitan City and Gyeongsangbuk-do (hereafter, Daegu and Gyeongbuk), where cluster infection occurred among a religious group called “Shincheonji” at the time of the initial COVID-19 outbreak, and 2) Other 15 provinces (Supplementary Tables 1 and 2). All statistical analyses were performed using SAS software ver. 9.4 (SAS Institute Inc., Cary, NC, USA).
RESULTS
Demographics of emergency patients during the COVID-19 pandemic
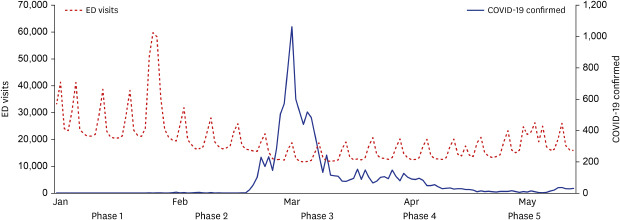
The number of ED visits during the study period was 2,636,341. Compared to phase 1, the number of ED visits decreased rapidly according to the COVID-19 outbreak: 803,160 (30.5%) in phase 1, 551,903 (20.9%) in phase 2, 377,212 (14.3%) in phase 3, 407,447 (15.5%) in phase 4, and 496,619 (18.8%) in phase 5. The median and interquartile range of ED LOS were 92 (43–162) minutes in phase 1, 95 (43–174) minutes in phase 2, 94 (37–185) minutes in phase 3, 95 (38–188) minutes in phase 4, and 93 (36–183) minutes in phase 5, respectively (P-for-trend 0.04). In-hospital mortality rates were 1.4% during the study period, 1.1% in phase 1, 1.4% in phase 2, 1.9% in phase 3, 1.7% in phase 4, and 1.5% in phase 5 (P-for-trend < 0.01) (Table 2). The trends of daily ED visits and COVID-19 confirmed patients during the study period are shown in Fig. 1.
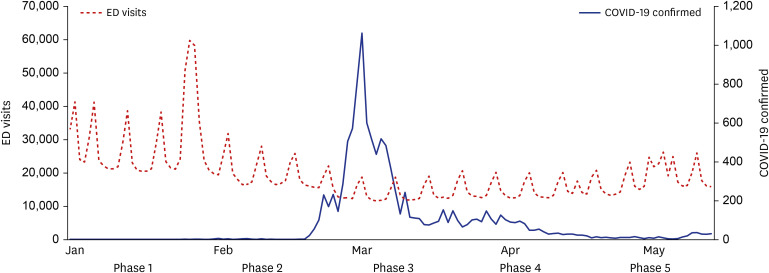
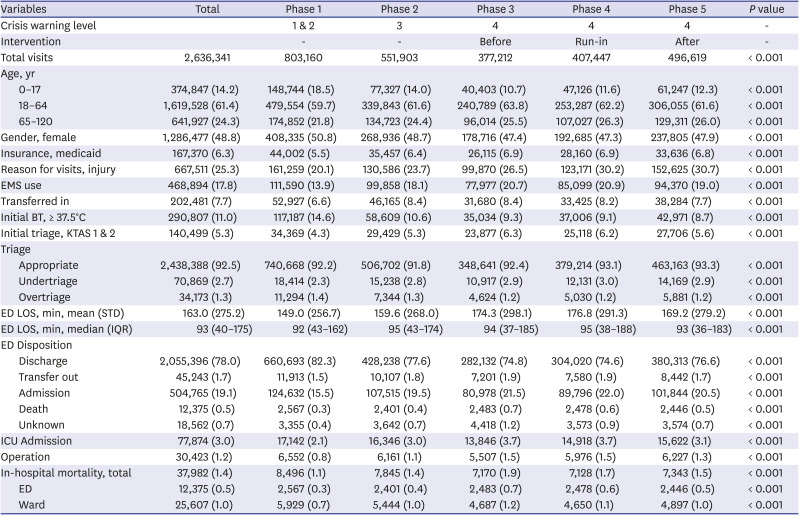
Fig. 1
Daily number of ED visits and confirmed COVID-19 patients during the study period.
ED = emergency department, COVID-19 = coronavirus disease 2019.
![]()
Table 2
Characteristics of the study population according to national crisis warning level and intervention
Data are presented as number (%).
EMS = emergency medical services, BT = body temperature, KTAS = Korean triage and acuity scale, ED = emergency department, LOS = length of stay, STD = standard deviation, IQR = interquartile range, ICU = intensive care unit.
![]()
The proportion of emergency patients with clinically important diagnoses among ED visits increased significantly (all P-for-trends < 0.01). For AMI, the in-hospital mortality rate was 10.0% during the study period (10.1% in phase 1 and 8.3% in phase 5); for acute ischemic stroke, the in-hospital mortality rate was 5.3% (5.3% in phase 1 and 5.0% in phase 5); for acute hemorrhagic stroke, the in-hospital mortality rate was 14.2% (13.3% in phase 1 and 14.9% in phase 5); and for severe trauma, the in-hospital mortality rate was 2.1% (2.1% in phase 1 and 1.9% in phase 5) (all P-for-trend < 0.01) (Table 3).
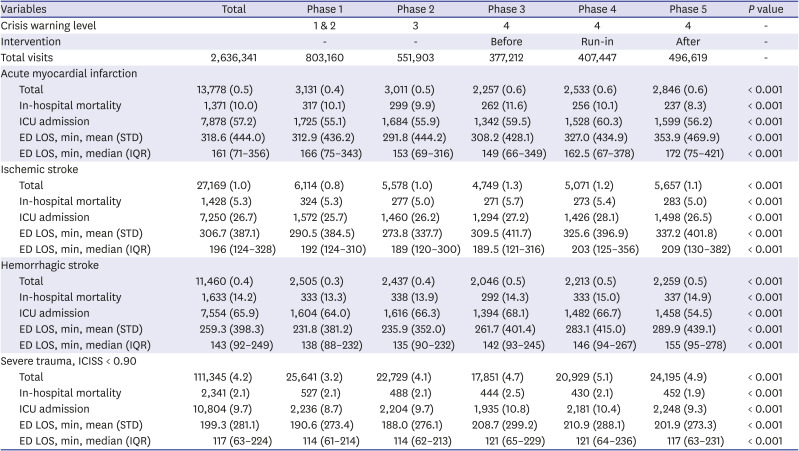
Table 3
Characteristics of patients with clinically important diagnoses according to the study phase
Data are presented as number (%).
ICU = intensive care unit, ED = emergency department, LOS = length of stay, STD = standard deviation, IQR = interquartile range.
![]()
Effects of emergency care interventions on safeties for emergency patients
For in-hospital mortality among the study population, compared to the study phase 3, the adjusted ORs (95% CIs) were 0.63 (0.61–0.65) for phase 1, 0.77 (0.74–0.79) for phase 2, 0.90 (0.87–0.93) for phase 4, and 0.77 (0.74–0.79) for phase 5. By subgroup for region, for the patients in Daegu and Gyeongbuk, the adjusted ORs (95% CIs) were 0.78 (0.71–0.87) for phase 4 and 0.57 (0.51–0.64) for phase 5 compared to phase 3, and for other 15 provinces, the adjusted ORs (95% CIs) were 0.93 (0.90–0.97) for phase 4 and 0.81 (0.78–0.84) for phase 5 compared to phase 3. By subgroup for diagnosis, for the patients with AMI, the adjusted ORs (95% CIs) were 0.69 (0.57–0.83) for phase 5 compared to phase 3, and for severe trauma, the adjusted ORs (95% CIs) were 0.83 (0.73–0.95) and 0.76 (0.67–0.87) for phase 4 and phase 5, respectively, compared to phase 3. For acute ischemic stroke and hemorrhagic stroke, the effect measures were not significant during any of the study phases (Table 4).

Table 4
Adjusted odds ratios and 95% CIs for in-hospital mortality for the study population
Data are presented as adjusted odds ratios (95% CI).
Odds ratios were adjusted for age and gender.
CI = confidence interval.
![]()
For ED LOS among the study population, compared to the study phase 3, the adjusted coefficients (95% CIs) were −18.1 (−19.2 to −17.1) minutes for phase 1, −12.3 (−13.5 to −11.2) minutes for phase 2, 1.7 (0.52 to 2.9) minutes for phase 4, and −5.3 (−6.5 to −4.2) minutes for phase 5. By subgroup analysis, for severe trauma, the ED LOS decreased by −5.7 (−11.0 to −0.3) minutes in phase 5 compared to phase 3. Compared to phase 3, the ED LOS in phase 5 was increased by 45.8 (21.3 to 70.2) minutes for the patients with AMI, 27.3 (12.4 to 42.2) minutes for acute ischemic stroke, and 28.5 (4.7 to 52.3) minutes for acute hemorrhagic stroke (Table 5).
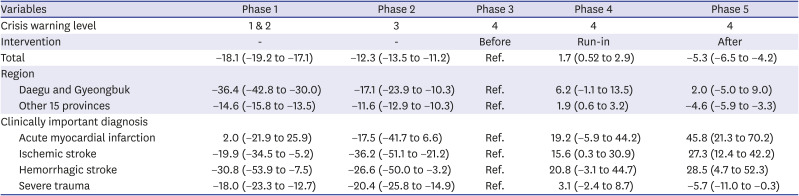
Table 5
Multivariable regression analysis for length of stay in emergency departments (minutes) for the study population
Data are presented as β coefficients (95% CI).
Beta coefficients were adjusted for age and gender.
CI = confidence interval.
![]()
DISCUSSION
Using a nationwide emergency patient database, we investigated the effects of emergency care-related health policies on the safety and clinical outcomes of emergency patients during the COVID-19 pandemic. In Korea, emergency care-related health policies aimed to treat suspected and confirmed COVID-19 patients with severe symptoms appropriately, to protect other uninfected emergency patients from infection and to provide appropriate care based on their severity in disaster situations. The number of ED visits during the study period decreased from 803,160 in phase 1 to 496,619 in phase 5. The in-hospital mortality rate increased from 1.1% in phase 1 to 1.9% in phase 3, as the COVID-19 pandemic progressed, and decreased to 1.5% in phase 5 after policy implementation (adjusted OR [95% CI], 0.77 (0.74–0.79) in phase 5 compared to phase 3). The ED LOS increased while the number of ED visits decreased as the COVID-19 pandemic progressed, and the ED LOS declined after policy implementation (beta coefficient: −5.3 minutes in phase 5 compared to phase 3). Implementing appropriate emergency care policies in the COVID-19 pandemic would have contributed to improving the safety of all emergency patients and reducing in-hospital mortality by preventing excessive deaths for not only for infected patients but also for uninfected patients.
During the COVID-19 pandemic, the number of emergency visits decreased, but the proportion of emergency patients with clinically important diagnoses among ED visits increased significantly. In previous studies, the number of medical visits decreased, but mortality rates in patients with specific diseases, including cancer, increased during the COVID-19 pandemic.1516 These phenomena were explained by several hypotheses; because of the risk and fear of transmission of COVID-19, the patients with acute emergency symptoms would be hesitant to visit the ED, even if the patient needed immediate emergency care, which may have increased the time delay before medical contact and delayed treatment.17 In addition, the lack of medical resources in the ED to treat emergency patients other than COVID-19 would be one of the possibilities. Because the treatment of COVID-19 patients requires more medical resources, in a pandemic disaster situation, there may be insufficient space and resources to provide adequate care to other emergency patients, which can increase in-hospital mortality and threaten safety.18 For this reason, public health policies must be implemented to ensure adequate emergency medical use for severe emergency disease patients, even in the COVID-19 pandemic situation.
In this study, implementation of emergency care-related health policies increased the number of isolation units and ICU beds in SEMC and enabled the web-based real-time sharing of resource information. The in-hospital mortality rates for all emergency patients decreased after policy implementation (phase 5 compared to phase 3), for not only Daegu and Gyeongbuk but also other 15 provinces. However, the effects of health policies varied among subgroups of emergency patients with clinically important diagnoses. Despite the designation of the SEMC, ED LOS increased in patients with AMI and stroke, probably due to the rapid increase in the number of COVID-19 confirmed patients with severe illness leading to a shortage of ICU beds. The mortality rates of emergency patients with clinically important diagnoses increased during the COVID-19 pandemic19202122 and the length of hospital stay for patients with the diseases increased23242526 in several countries with no relevant health policies. The in-hospital mortality rates of AMI and severe trauma, which increased during the early phase of COVID-19 outbreak, could be reduced by implementing the emergency care-related health policies.
During the COVID-19 pandemic, the mortality rates of confirmed cases were different for each country, from over 16% in France to less than 0.3% in Singapore.2728 Such broad variation implies that there are factors, such as government response, other than patient characteristics that determine COVID-19 mortality.29 Effective government policies responded to the COVID-19 pandemic proactively to ensure a sufficient supply of personal protective equipment, provision of good public health services in treating infected patients, and quick implementation of screening programs.3031 In addition, emergency care-related health policies could address not only reduced accessibility to healthcare services but also a shortage of human and economic resources that strain the healthcare system for uninfected emergency patients. Korea was the second-largest country with confirmed COVID-19 patients, which was due to the rapid increase in COVID-19 patients in March 2020, but it is evaluated as one of the countries that is currently successfully carrying out COVID-19 prevention with a strong preemptive response. Since the ED is a place where many patients with various diseases are concentrated, it is necessary to establish a system to respond properly to disaster situations. The emergency care-related health policies, including the designation of 57 SEMC, expansion of isolation units, and real-time sharing of resource information of SEMC on the NEMC portal (portal.nemc.or.kr), would have allowed timely provision of appropriate care and quick determination of ED disposition after acute care for not only for infected patients but also for uninfected patients. As the COVID-19 pandemic is currently underway, it is necessary to analyze further the impact of emergency care-related health policies in the COVID-19 pandemic on the safety of all emergency patients after the end of the pandemic. Our findings have important implications for implementing emergency care policies in the potential risk of chronic COVID-19 pandemics or other communicable disease outbreaks.
The limitations of this study are as follows. First, this is a quasi-experimental study and does not use a randomization controlled trial. Types of selection bias that can occur in quasi-experimental studies include maturation bias and instrumentation bias. These bias effects may have different outcomes by country and circumstance. Second, study subgroups were defined by the Korean Standard Classification of Diseases-7 code. Misclassification bias in subgroups was possibly present in studies. Therefore, it is necessary to conduct detailed studies on changes before and after the COVID-19 outbreak through future research. As the COVID-19 pandemic is currently underway, it is necessary to analyze further the impact of emergency care-related health policies on the safety of patients after the end of the communicable disease pandemic.
During the COVID-19 pandemic, implementing emergency care-related health policies would contribute to improving the safety of all emergency patients and reducing in-hospital mortality by preventing excessive deaths in critically ill patients visiting EDs. Implementing a multidisciplinary approach and evidence-based policy in a disaster situation will be the driving force to protect the safety and lives of the people despite the ongoing threat.
 XML Download
XML Download