

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
Remote or geographically isolated workers are isolated from other people's assistance because of the location, time, or nature of their work. Their jobs eliminate wasted commuting time, provide flexible working hours, and increase geographical coverage.1 However, there might be problems concerning the safety and healthcare of the individuals. The potential risks associated with performing work activities increase significantly when performed in remote or isolated situations. Workers in remote areas also sustain injuries at higher rates than their counterparts living in major cities or in the mainland, besides being susceptible to occupational risks and hazards.234 In isolated situations, mental health problems such as stress have also been reported.5 The major problem of the island workers, along with safety and health problems, is their inaccessibility to proper hospital services in the time of need.2
There are statutes and guidelines for remote workers in Australia. However, in Asian countries and others, the remote workers' risks are not well known.3 Specifically, data on the health problems of workers in geographically isolated places such as islands have not been properly documented. Globally, there are about 730 million people who live in the islands. This constitutes about 10% of the world's population.6 An island is surrounded by sea and is at a certain distance from the land. Therefore, islanders are relatively isolated from the surrounding area and are confined within a certain space. Due to such geographical position, people residing in islands face many natural and social restrictions. Besides, there are numerous safety and health problems.4789 In the restricted environment, isolated workers have excessive responsibility and job stress in situations where it is difficult to get help, which can have a negative impact on mental health.10 Moreover, workers working in the island without their families can have a negative impact on the mental health due to deterioration of social isolation such as loneliness.11 In addition, there are not enough medical facilities in the island, and it is not easy to transport to hospitals, so there is a high risk of unmet medical care.12 In addition, there is a lack of safety and health regulation and protection due to administrative convenience and cost problems in the island, and island workers have a high risk of injury in this environment.4 However, there have been very few studies that have focused on the workers' working environment in such areas and the lives of the workers in general.
This study aimed at analyzing the health status of geographically isolated workers. Among the diverse parameters analyzed, occupational injury, unmet medical needs, psychological status, and lifestyle of the island workers were scrutinized.
METHODS
This study aimed to identify the occupational characteristics and health status of geographically isolated workers. There are 3,952 islands in the Republic of Korea, and it is the country with the fourth-highest number of islands in the world, following Indonesia, the Philippines, and Japan.9 Baekryeong Island, which has the largest population among the outermost islands where geographically isolated workers' characteristics could be identified, was selected as the study area.13 The survey was conducted through five surveyors for about two months between April 1 and May 31, 2020. As of February 29, 2020, the Baekryeong Island's population was 5,241, consisting of five ri (administrative units in South Korea: Bukpo-ri, Jinchon-ri, Gaeur ri, Yeonhwa-ri, and Nampo-ri) (Fig. 1). Since it is an island adjacent to North Korea, military areas are distributed. Most of the population (76.5%) reside in Jinchon-ri and Bukpo-ri, and most of the people work in these two regions. As per the population's distribution, three investigators in downtown Jinchon-ri, where the village office is located, one investigator in the fringe of Jinchon-ri, and one in Bukpo-ri conducted the questionnaire. The number of adult workers who completed the questionnaire was 110.

The questionnaire consisted of four categories: demographic characteristics, occupational characteristics, lifestyle, and health status. Demographic characteristics included age group, gender, education, and household income. Household income was presented in quartiles, which were divided using the household income quartile standard of the 2018 Korea National Health and Nutrition Survey.
The occupational characteristics included working hours, shift work, and the Korean standard classification of occupations (KSCO).14 As per the KSCO, ‘managers,’ ‘professionals and related workers,’ ‘clerks,’ ‘service workers,’ and ‘sales workers’ were classified as non-manual workers, and ‘skilled agricultural, forestry and fishery workers,’ ‘craft and related trades workers,’ ‘equipment, machine operating and assembling workers,’ ‘elementary workers,’ ‘armed forces’ were classified as manual workers. Job satisfaction was investigated using a four-point Likert scale. When an individual responded with “very dissatisfied” or “dissatisfied” for job satisfaction, poor job satisfaction was defined as ‘yes,’ and the other answers were defined as ‘no.’
The lifestyle of the individuals included alcohol use disorders, smoking, and physical activity. The Korean version of the Alcohol Use Disorders Identification Test (AUDIT-K) was used, and alcohol use disorder was defined when the score was 12 or higher.15 The physical activity questionnaire was used, and active physical activity was defined as ‘moderate physical activity at least 5 days a week and at least 30 minutes’ or ‘vigorous physical activity at least 3 days a week or and at least 20 minutes,’ and inactive physical activity was defined as other answers.16
Factors related to health status, sleep disorder, depression, perceived health status, unmet medical needs, and occupational injuries were considered. Sleep disorder was defined when the Korean version of the Pittsburgh Sleep Quality Index (PSQI-K) was 8.5 or more.17 For depression, the Korean version of the Patient Health Questionnaire-9 (PHQ-9) was used,18 and the cutoff was defined as 10 points.19 Perceived health status was surveyed using a 5-point Likert scale, and ‘poor perceived health status’ was defined as ‘yes’ when the responses were ‘very poor’ and ‘poor,’ and was defined as ‘no’ when responses were “fair,” “good,” and “excellent.” The unmet medical needs were evaluated through the question “In the last one year, have you required hospital treatment but have not received it?”, and the answers were “Yes,” “No,” and “I have never needed a hospital examination.” Occupational injury was investigated through the questions “Over the last 12 months, did you suffer from any of the following health problems?” “Injuries (hurt by accident)?” and “Due to your job?”.20
This study was conducted to identify the occupational characteristics and health status of geographically isolated workers in Baekryeong Island. In the case of major variables, the study participants were compared with a reference population who participated in a similar survey using the same questionnaire. Major variables included occupational injury, unmet medical needs, lifestyle (alcohol use disorder and inactive physical activity), and psychological factors (depression, poor perceived health status, poor job satisfaction, sleep disorder) (Table 1). As the reference study population, nationally representative data were used, and the data closest to the survey period of this study were used. To compare the main variables of the study participants, and the reference study population, the age-standardized prevalence ratio (aSPR) was calculated through indirect standardization. The 95% confidence intervals (95% CIs) of aSPR were calculated using Byar's approximation.21 This study's participants were workers, so they were compared with workers among the reference population considering the health workers' effects. To consider the characteristics according to sex, the male and female groups were stratified and analyzed. Since the classification of occupations is an important factor in the working environment, aSPR was calculated by dividing participants into non-manual workers and manual groups. Also, Baekryeong Island is close to North Korea, so the proportion of professional soldiers among the workers in Baekryeong Island could be high. Therefore, many of them can be included as manual workers. Since professional soldiers might have different occupational environments from other manual workers, the risk of manual workers excluding soldiers was also calculated. In remote workers, connections with families are an important factor in psychological problems.22 Therefore, analysis was performed according to whether the family resides in the island. Statistical analysis was conducted using SAS version 9.4 (SAS Institute, Cary, NC, USA).
Table 1
The measurement instrument of the main outcome and comparison databases of this study
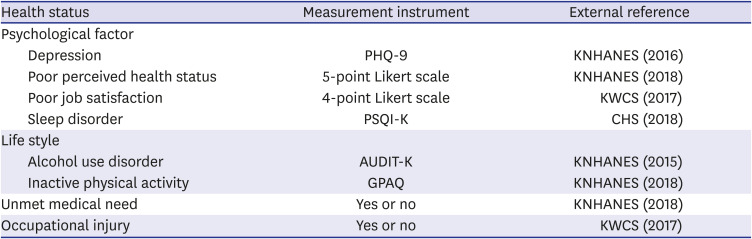
PHQ-9 = Korean Version of the Patient Health Questionnaire-9, PSQI-K = Korean version of the Pittsburgh Sleep Quality Index, AUDIT-K = Korean version of Alcohol Use Disorders Identification Test, GPAQ = Global Physical Activity Questionnaire, KNHANES = Korea National Health and Nutrition Examination Survey, KWCS = Korean Working Conditions Survey, CHS = Community Health Survey.
RESULTS
The characteristics of the participants are shown in Table 2. Among the demographic characteristics, 65.5% of the participants were in the age group 20–39 years, while 34.5% constituted those aged 40 years or older. Regarding the distribution of the subjects based on their gender, 64.5% were male, and 35.5% were female. In the highest level of education attained, high school or below accounted for the majority (70.9%) of the participants. Household income was the highest in the very high quartile (19.1%). Among the occupational characteristics, working hours less than 40 hours accounted for the most (50%), and long working hours (> 60 hours) accounted for 8.18%. The most frequent working schedule was daytime schedule (83.6%), and shift work including evening time, rotating day and night, and irregular working time was 16.4%. The occupation classification resulted in 62.7% of subjects being non-manual workers, while 37.3% were engaged as manual workers. “Dissatisfied” (60%) was the most frequently answered option for job satisfaction. When it comes to lifestyle, alcohol use disorder, and smoking status, 30% responded with an affirmative answer. Physical activity was reported in 43.6% of the population, while 56.4% of individuals reported inactive physical activity. Factors related to health status were sleep disorder (28.2%), depression (6.36%), and occupational injury (8.18%). Regarding perceived health status, the participants responded mostly as fair (42.7%), and poor perceived health status accounted for 9.09%. Unmet medical needs accounted for 48.2% of the patients.
Table 2
Characteristics of the study participants (n = 110)

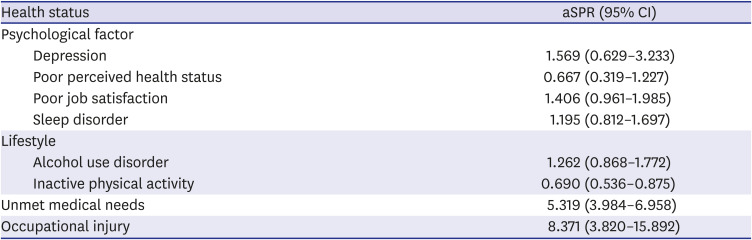
The aSPR was calculated using the study participants' responses and workers' data among the external reference population (Table 3). Compared with the same age structure, there was a significant increase in the risk of unmet medical needs (aSPR, 8.371; 95% CI, 3.820–15.892) and occupational injury (aSPR, 5.319; 95% CI, 3.984–6.958). In contrast, inactive physical activity (aSPR, 0.690; 95% CI, 0.536–0.875) was significantly decreased.
Table 3
aSPR for all workers' psychological factor, lifestyle, unmet medical needs, and occupational injury
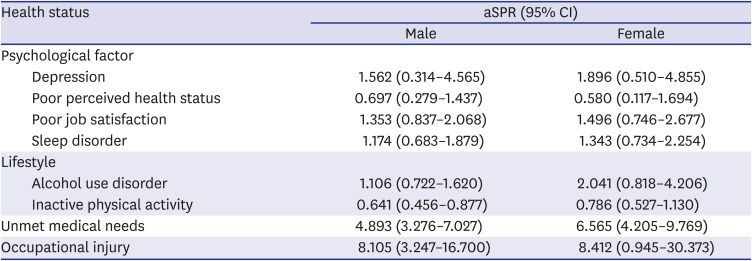
In order to evaluate sex differences, the results for males and females were calculated separately (Table 4). The aSPR for male workers was calculated using the responses of male study participants and male workers' data among the external reference population. The aSPR for female workers was calculated using the responses of female study participants and female workers' data among the external reference population, respectively. Both men and women showed a significant increase in the risk of unmet medical needs (male: 4.893; 95% CI, 3.276–7.027; female: 6.565; 95% CI, 4.205–9.769). Unlike female workers, only male workers showed a significant increase in the risk of occupational injury (male: 8.105; 95% CI, 3.247–16.700; female: 8.414; 95% CI, 0.945–30.373), and showed a significant decrease in the risk of inactive physical activity (male: 0.641; 95% CI, 0.456–0.877; female: 0.786; 95% CI, 0.527–1.130).
Table 4
aSPR for male and female workers' psychological factor, lifestyle, unmet medical needs, and occupational injury
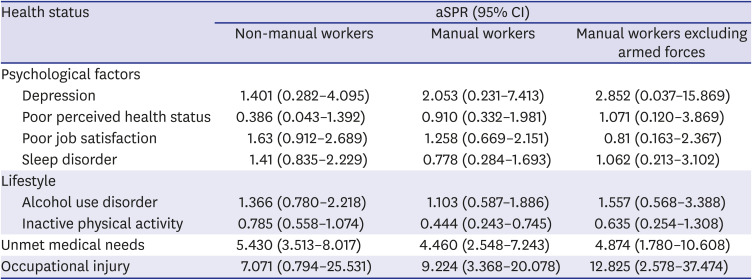
To identify the differences by classification of occupation, the results of non-manual workers and manual workers were measured separately (Table 5). The aSPR for non-manual/manual workers was calculated using the non-manual/manual study participants' responses and non-manual/manual workers' data among the external reference population. Both non-manual and manual workers showed a significant increase in the risk of unmet medical needs (non-manual workers: 5.430; 95% CI, 3.513–8.017; manual workers: 4.460; 95% CI, 2.548–7.243). Unlike non-manual workers, only manual workers showed a significant increase in the risk of occupational injury (non-manual workers: 7.071; 95% CI, 0.794–25.531; manual workers: 9.224; 95% CI, 3.368–20.078). The results for manual workers and manual workers, including armed force, were similar.
Table 5
aSPR for non-manual and manual workers' psychological factor, lifestyle, unmet medical needs, and occupational injury
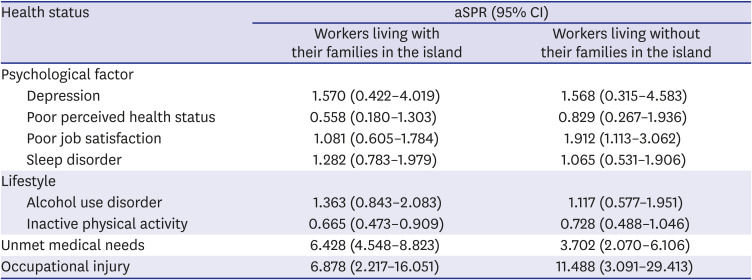
The results were shown by dividing the study participants according to whether their families lived together in the island (Table 6). The aSPR for workers living with /without their families in the island was calculated using the responses of workers living with /without their families in the island and data of workers living with/without their families in the island among the external reference population. Regardless of whether or not family members lived together in the island, both showed significantly increased risk for unmet medical needs (workers living with their families in the island: 6.428; 95% CI, 4.548–8.823; workers living without their families in the island: 3.702; 95% CI, 2.070–6.106) and occupational injury (workers living with their families in the island: 6.878; 95% CI, 2.217–16.051; workers living without their families in the island: 11.488; 95% CI, 3.091–29.413). Only workers living without their families in the island showed a significant increase in the risk of poor job satisfaction (aSPR, 1.912; 95% CI, 1.113–3.062). The protective effect on inactive physical activity was not statistically significant in workers living without their families in the island (aSPR, 0.728; 95% CI, 0.488–1.046), unlike workers living with their families in the island (aSPR, 0.665; 95% CI, 0.473–0.909).
Table 6
aSPR for psychological factor, lifestyle, unmet medical needs, and occupational injury of workers living with and without their families in the island
DISCUSSION
This study showed that workers in Baekryeong Island were at an increased risk of acquiring health and safety problems compared to the general population. Island workers showed a significant increase in the risk of unmet medical care and occupational injury. Workers who did not live in the island with their families reported of their poor job satisfaction.
It is noteworthy that the results reveal the risk of occupational injury in island workers. In particular, male manual workers showed a significant increase in risk compared with the external reference population.2324 The risk of occupational injury for island workers was similar to the study results of workplace injuries performed in Pacific island countries.4 It is necessary to understand the characteristics of the island industry to ascertain the risks of occupational injury. In terms of the workplace's size, it is difficult to have a large number of workers in a geographically isolated location. According to the statistics of Ongjin County, which is constituted by the island region that included the Baekryeong Island, there was one large-scale workplace with 300 or more employees, three medium-sized workplaces with 50 or more employees, and 530 small-scale workplaces (99.25%) with less than 50 employees. Small-scale workplaces also have risk factors associated with occupational injuries.2025 Small-scale workplaces generally have short working periods and high turnover rates.2627 Also, small-scale workplaces are operated only with small assets, thereby making investments in safety and health difficult.2829 Thus, small-scale workplaces are likely to be excluded from industrial safety and health systems.30 The government majorly focuses on large-scale workplaces because of human resources and equipment limitations, and small-scale workplaces are often not covered by national policies and strategies.3132 In Korea, it is difficult to apply for systematic industrial health management because small-scale workplaces are not obliged to appoint health managers according to the Occupational Safety and Health Act.33 Furthermore, even if the placement of safety managers is emphasized in Korea's construction industry, construction in the island area is an exception. Island workplaces that do not employ such health or safety managers can increase the risk of occupational injury due to a relatively low level of knowledge and awareness.30
Through this study, it was important to identify occupational injury risks to island workers. The risk of unmet medical care was identified simultaneously. The important aspect in the care of injured people is timely access to emergency services, including road ambulances and hospital services. However, in remote areas, comprehensive medical services are often unavailable, and injured patients might need to be transported long distances, in emergencies, to avail definitive care in a tertiary hospital.34 It is important to prevent and manage occupational injuries to island workers, leading to fatal health problems.
Since isolated workers are difficult to supervise and cooperate, they suffer from anxiety, risk of decision errors, and cognitive reactions, and can potentially contract psychological problems.10 Moreover, in geographically isolated workers, there are very few cultural facilities, so there are few opportunities for emotional recovery after work. However, there was no significant difference in the psychological factors of the subjects in this study. Although Baekryeong Island is an island far from the mainland, there are cafes, sports facilities, large marts, and small movie theaters that provide a decent cultural life to its residents. In particular, the subjects displayed a high participation rate in exercise-related activities in Baekryeong Island. Thus, the risk of inactive physical activity was significantly lower in this study. Also, compared to other types of isolated workers, geographically isolated workers do not always work alone, so they can be considered to be at a relatively low psychological risk. However, if the family did not live together in the island, the subjects ran the risk of dissatisfaction with their jobs. Even though Baekryeong Island had a better environment than a general remote area, separation from family could cause emotional problems.35 Another possibility is that working in an environment without a family is likely to be a temporary job, raising the risk of poor job satisfaction.36
The total number of study participants was 110, which was 8.3% of the 1,325 workers in Baekryeong Island. As a general prejudice in Korea, it can be thought that farming and fishing workers constitute the majority of the worker population in the island far from the mainland. Thus, there are more manual workers in the island. However, in this study, non-manual workers were higher than manual workers. There are no statistical data on the classification of occupation of Baekryeong Island. Still the data on the number of workers by industry were in the order of ‘Accommodation and food service activities’ (29.1%), ‘Construction’ (11.1%), ‘Wholesale and retail trade’ (10.6%), ‘Education’ (8.7%), and ‘Manufacturing’ (7.2%). Besides, the number of workers by industry in agriculture, forestry, and fishing was 0.2%. This information indicated a difference from the pre-conceived notions about island occupations, and the distribution of the participants in this study was appropriate. Moreover, statistics by gender of Baekryeong Island workers could not be identified, but the total population consisted of male (59.1%) and female (40.9%) individuals, which was similar to the gender distribution in this data. However, it should be applied and emphasized more strongly because of the risk of the island.
Specifically, it is necessary to check the guidelines protecting workers' health and safety from the risk of geographically isolated working conditions.2 Employers should be aware of the risks to island workers and establish emergency procedures. Workers working in isolated locations must be verified for appropriate working conditions, and must be evaluated for medical suitability. In addition, the island workers should be provided with opportunities for sufficient safety education. Even if there is a problem with the geographic accessibility of the island, the island workers should also have safety and health experts hired by managers and managed by the experts. It is imperative to verify access to which emergency services for accidents can be provided immediately in the island, and to prepare for ‘worst-case scenario,’ especially. The government should not abandon the application of regulations for safety and health due to geographical accessibility. In the case of an accident, the island is difficult to access treatment, so stronger safety management should be requested. Additionally, workers should also pay attention to safety. Island workers must comply with safety guidelines and actively receive safety training. Island workers are encouraged to communicate fully with their employers about work environments where there is a high risk of accidents.
There are limitations to this study. First, this study was conducted on only one Korean island. Although the island is one of the outermost islands, it could show specific characteristics of geographically isolated areas. Nonetheless, there is a limit to generalization due to the characteristics of workers in all island. Moreover, the participants in the current study were younger and higher educated than the general working population. It might have a few limitations to generalize or directly apply to other countries as well. Second, since the results of the current study are easily affected by the number of cases due to the small number of samples, there is a risk of effect estimation. Further research is needed to obtain representative large samples. Third, the safety and health outcomes used are based on self-reporting. Therefore, there is a limitation on the accurate evaluation of these parameters. Fourth, standardization was performed only for age, and adjustment for other confounders was not performed. Fifth, this was a cross-sectional study, and a longitudinal study is needed to confirm the causal relationship in the future.
In conclusion, this study identified the safety and health problems of geographically isolated workers in Baekryeong Island. The risk of occupational injury and unmet medical care could be observed in individuals of the islands. This significantly proves that preventive practices must be implemented to minimize occupational risks in such islands. In the future, greater attention and further studies are needed for island workers in geographically isolated areas.
 XML Download
XML Download