

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Based on the 2012 revised international Chapel Hill Consensus Conference nomenclature of vasculitides, antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) has currently been defined as the necrotising vasculitis without definite immune-complex deposition. AAV primarily affects small vessels, including small intraparenchymal arteries, arterioles, capillaries and venules and occasionally medium-sized arteries and veins.1 In addition, AAV can be further classified three subtypes based on pathogenesis, histological findings, clinical symptoms and signs and laboratory results such as microscopic polyangiitis (MPA), granulomatosis with polyangiitis (GPA) and eosinophilic GPA (EGPA).12
Each systemic vasculitis has its own typical sex difference in the incidence: for instance, among large vessel vasculitis, giant cell arteritis has the male to female ratio of 1:3, whereas Takayasu arteritis has the male to female ratio of 1:9.3 Moreover, each systemic vasculitis has a sex differences in the clinical features: for instance, with regard to Korean patients with Behcet's disease, female patients exhibited more frequently genital ulcers, peripheral arthritis, and inflammatory low back pain, whereas male patients showed a higher frequency of skin lesions.4 There was a previous study pertaining to the sex difference in AAV patients, which reported that male patients were vulnerable to the progression to end-stage renal disease (ESRD) compared to female patients. However, this study included only ANCA-positive AAV patients with histologically proven pauci-immune necrotising glomerulonephritis. For this reason, the results could not be generalised to all AAV patients.5 Also, given the ethnic and geographical differences affecting both the clinical manifestation and the poor outcomes of AAV, a need for a study investigating the sex difference in Korean patients with AAV is still raised but there has been no study on it to date. Hence, in this study, we investigated and compared the initial clinical features at diagnosis and the poor outcomes during follow-up in Korean patients with AAV based on sex.
METHODS
Patients
The medical records of 223 immunosuppressive drug-naïve patients with AAV were reviewed. They had been initially diagnosed or reclassified as AAV at the Division of Rheumatology, the Department of Internal Medicine, Yonsei University College of Medicine, Severance Hospital, from October 2000 to March 2020. All patients met the 2007 European medicines Agency algorithm for polyarteritis nodosa and AAV as well as the 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides.12 All patients had the medical records well-documented enough to either collect or assess AAV-specific indices including Birmingham vasculitis activity score (BVAS) version 3 and five-factor score (FFS).67 They had the initial results of ANCA by both an indirect immunofluorescence assay (IFA) for perinuclear (P)-ANCA and cytoplasmic (C)-ANCA and an antigen-specific assay for myeloperoxidase (MPO)-ANCA and proteinase 3 (PR3)-ANCA. Patients negative by antigen-specific assay but positive for ANCA by IFA were considered to have MPO-ANCA or PR3-ANCA when AAV was strongly suspected by the clinical and laboratory features.8 Patients, who had serious medical conditions mimicking the clinical features of AAV at diagnosis such as malignancies, infectious diseases and autoimmune diseases other than AAV, were excluded from this study. In addition, patients, who had been received immunosuppressive drugs prior to diagnosis, were also excluded. All patients had been followed up for at least more than 3 months from the time of diagnosis.
Clinical and laboratory data at diagnosis and during follow-up
In terms of variables at diagnosis, sex, age, body mass index (BMI) and smoking history were collected as demographic data. AAV subtypes, ANCA positivity, clinical features based on BVAS items,6 and AAV-specific indices were obtained. As acute-phase reactants, erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were also obtained. In terms of variables during follow-up, all-cause mortality, ESRD, cerebrovascular accident (CVA) and cardiovascular disease (CVD) were assessed as the poor outcomes of AAV. ESRD was defined as the status requiring for renal replacement therapy due to estimated glomerular filtration rate of less than 15 mL/min/1.73m2.5 On the basis of sub-items of cardiovascular and nervous systemic items of BVAS,6 CVA was defined as both ischaemic and haemorrhagic strokes, whereas CVD was defined as loss of pulses, vascular heart disease, pericarditis, ischaemic cardiac pain, cardiomyopathy and congestive cardiac failure. Since all patients were classified as AAV in our institute and most of them have been followed up, we could easily access the medical record in our institute to obtain data on the date of death and the first date of diagnosis of ESRD, CVA and CVD. In addition, information regarding all-cause mortality, ESRD, CVA and CVD in patients, who were not followed up in our institute, could be obtained by the Korean National Health Insurance Service system. The follow-up period based on all-cause mortality was defined as the periods from the time of diagnosis of AAV to the death for deceased patients, and those to the last visit for survived patients. On the other hand, the follow-up periods based on ESRD, CVA and CVD were also defined as the periods from diagnosis to either the first renal-replacement, the first diagnoses of CVA or that of CVD, respectively. We counted the number of patients who received each drug among glucocorticoid and immunosuppressive drugs.
Statistical analyses
All statistical analyses were conducted using SPSS software (version 23 for Windows; IBM Corp., Armonk, NY, USA). Continuous variables were expressed as a mean ± standard deviation, and categorical variables were expressed as number and the percentage. Significant differences in categorical variables between the two groups were analysed using the χ2 and Fisher's exact tests. Significant differences in continuous variables between the two groups were compared using the Mann-Whitney test. Comparison of the cumulative survivals rates between the two groups was analysed by the Kaplan-Meier survival analysis with the log-rank test. The multivariable Cox hazard model using variables with statistical significance in the univariable Cox hazard model was conducted to appropriately obtain the hazard ratios (HRs) during the considerable follow-up period. P values less than 0.05 were considered statistically significant.
RESULTS
Comparison of variables at diagnosis
The median age was 59.0 years and 74 of 223 AAV patients (64.8%) were men. AAV patients were divided into two groups based on sex and variables at diagnosis were compared between the two groups. Male patients exhibited a higher median BMI than female patients (23.2 vs. 22.0 kg/m2, P = 0.004). Age, smoking history, AAV subtypes, ANCA positivity and the clinical features based on BVAS items did not significantly differ between male and female patients. Also, there were no significant differences in AAV-specific indices and acute-phase reactants between the two groups (Table 1).
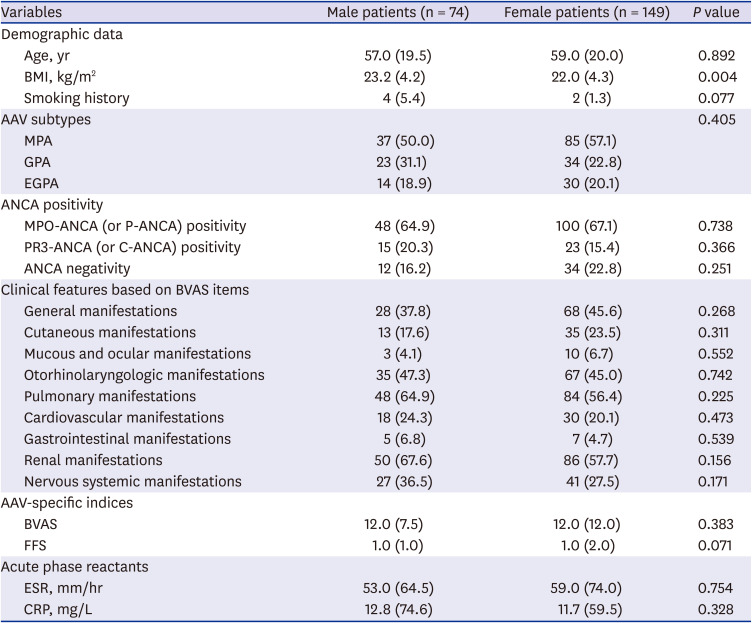
Table 1
Comparison of variables at diagnosis in 223 patients with AAV
Values are expressed as a median (interquartile range) or number (%).
ANCA = antineutrophil cytoplasmic antibody, AAV = ANCA-associated vasculitis, BMI = body mass index, MPA = microscopic polyangiitis, GPA = granulomatosis with polyangiitis, EGPA = eosinophilic granulomatosis with polyangiitis, MPO = myeloperoxidase, P = perinuclear, PR3 = proteinase 3, C = cytoplasmic, BVAS = Birmingham vasculitis activity score, FFS = five-factor score, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein.
![]()
Comparison of variables during follow-up
With regard to the poor outcomes of AAV, there were no significant differences in the frequencies of the poor outcomes of AAV between the two groups. Among glucocorticoid and immunosuppressive drugs administered during follow-up, male patients received cyclophosphamide more frequently compared to female patients (62.2% vs. 44.3%, P = 0.012) (Table 2).
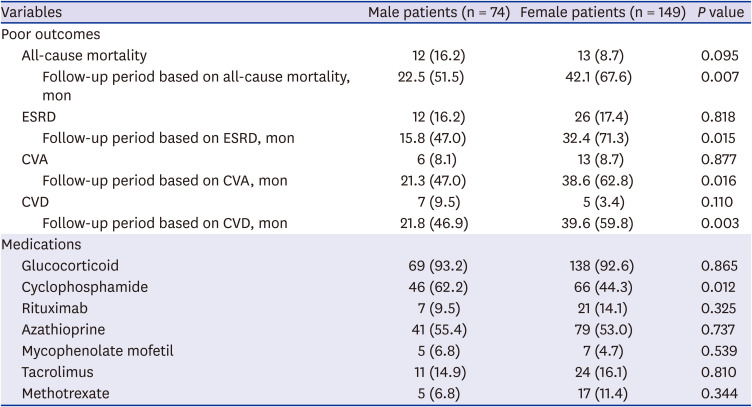
Table 2
Comparison of variables during follow-up in 223 patients with AAV
Values are expressed as amedian (interquartile range) or number (%).
ANCA = antineutrophil cytoplasmic antibody, AAV = ANCA-associated vasculitis, ESRD = end-stage renal disease, CVA = cerebrovascular accident, CVD = cardiovascular disease.
![]()
Comparison of cumulative survival rates
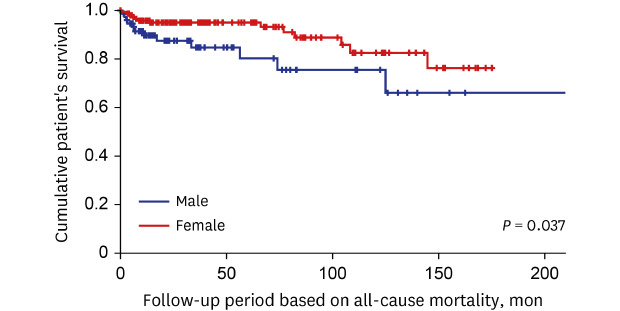
Among the four poor outcomes of AAV, male patients exhibited a significantly lower cumulative patients' survival rate than female patients during the follow-up period based on all-cause mortality (P = 0.037). Meanwhile, male patients tended to have a lower CVD-free survival rate compared to female patients but it did not reach statistical significance (P = 0.057) (Fig. 1).
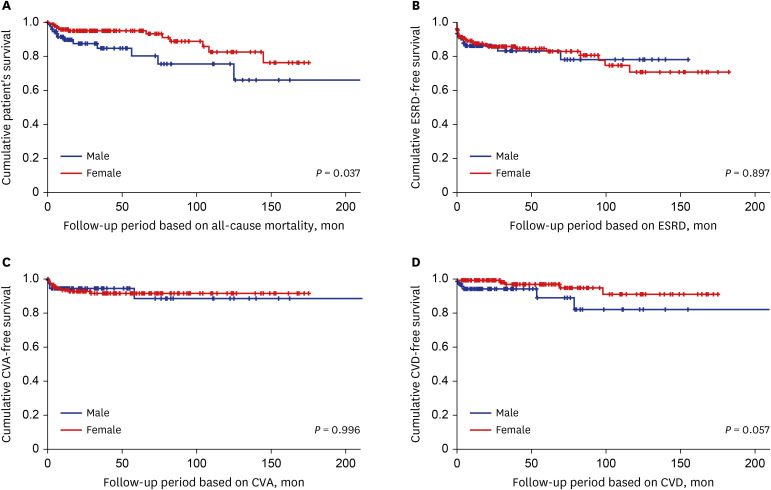
Fig. 1
Comparison of the cumulative survival rates between male and female patients with AAV.
Among all-cause mortality, ESRD, CVA and CVD, only a cumulative patients' survival rate diffed between male and female AAV patients. Male patients exhibited a significantly lower cumulative patients' survival rate than female patients.
ANCA = antineutrophil cytoplasmic antibody, AAV = ANCA-associated vasculitis, ESRD = end-stage renal disease, CVA = cerebrovascular accident, CVD = cardiovascular disease.
![]()
Cox hazard model analyses
In the univariable analysis, age (HR, 1.055), male sex (HR, 2.264), smoking history (HR, 6.052), BVAS (HR, 1.096) and FFS (HR, 2.142) at diagnosis were significantly associated with all-cause mortality during follow-up. In the multivariable analysis, both male sex (HR, 2.378; 95% confidence interval [CI], 1.050–5.384) and FFS (HR, 1.693; 95% CI, 1.071–2.676) at diagnosis were significantly and independently associated with all-cause mortality during follow-up (Table 3).
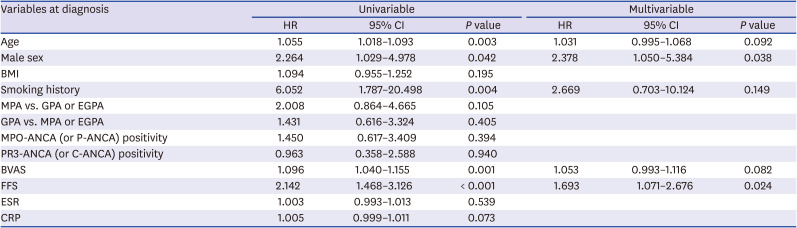
Table 3
Cox hazards model analysis of variables at diagnosis for all-cause mortality during follow-up in 223 patients with AAV
ANCA = antineutrophil cytoplasmic antibody, AAV = ANCA-associated vasculitis, HR = hazard ratio, CI = confidence interval, BMI = body mass index, MPA = microscopic polyangiitis, GPA = granulomatosis with polyangiitis, EGPA = eosinophilic GPA, MPO = myeloperoxidase, P = perinuclear, PR3 = proteinase 3, C = cytoplasmic, BVAS = Birmingham vasculitis activity score, FFS = five-factor score, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein.
![]()
DISCUSSION
In this study comparing the clinical features based on the sex difference in AAV patients, we discovered the following three new findings. First, at the time of diagnosis, the clinical features and laboratory related to AAV, such as AAV subtypes, ANCA positivity, clinical manifestations and AAV-specific indices, did not significantly differ between male and female patients. Second, during the follow-up period, male patients exhibited a significantly lower cumulative patients' survival rate compared to female patients. Third, male sex together with FFS was proved to be an independent predictor of all-cause mortality during the follow-up period in AAV patients.
Only male sex itself does not seem to simply increase the rate of all-cause mortality in this study. A previous study reported introduced dietary risks, tobacco smoking, high BMI, high blood pressure and high fasting plasma glucose as the most common risk factors for mortality. However, male sex itself was not clearly defined as a primary risk factor for mortality.9 Another previous study denied the fact that the life expectancy of men was meaningfully lower than that of women. Instead, it suggested the different clinical features based on the sex difference.10 Meanwhile, although there were no differences in clinical manifestations at diagnosis between male and female AAV patients, in the multivariable Cox analysis, male sex was an independent predictor of all-cause mortality during follow-up. It is difficult to suggest the exact mechanism, but it can be assumed that in a condition with persistent AAV, male patients are more frequently exposed to situations that may increase the rate of all-cause mortality compared to female patients. The result that cyclophosphamide had been administered to male patients more frequently than female patients during the follow-up period may support our assumption.
At diagnosis, male patients showed a higher mean BMI than female patients.
We wondered whether a high BMI in male patients has influenced an increase in all-cause mortality compared to female patients. To get the clue to prove this, we compared BMI between survived and dead patients with AAV and found that there was no significant difference between the two groups (22.1 vs. 23.0 kg/m2, P = 0.292). In addition, in the multivariable Cox analysis, BMI was not significantly associated with all-cause mortality (Table 3). Why did not the high calculated BMI in male patients contribute to an increased all-cause mortality rate in male patients? According to the previous studies, the rate of all-cause mortality showed a U-shape with BMI between 22.5 and 25 kg/m2 as a reference range: the rate of all-cause mortality tended to increase not only in the BMI range of below 22.5 (or 25) kg/m2 but also in BMI range of above 25 kg/m2.1112 However, unlike the previous studies, in this study, the BMI range, where the largest number of AAV patients died (44.0%), was between 22.1 and 25.0 kg/m2. It could be assumed that this discrepancy was derived from the different study-subjects between general people and AAV patients and furthermore, it might offset the high calculated BMI in male patients from contributing to an increased all-cause mortality rate.
A previous study, male sex was significantly associated with ESRD occurrence compared to female sex in AAV patients with histologically proven pauci-immune necrotising glomerulonephritis.5 However, unlike the previous study, no significant difference in the cumulative ESRD-free survival rate between male and female patients in this study. Although not all patients with renal involvement underwent renal biopsy, to reproduce the result of the previous study, we included only AAV patients with renal involvement (50 men and 86 women) and analysed it again. However, we could find no significant difference in the cumulative ESRD-free survival rates between male and female patients during the follow-up period based on ESRD (P = 0.994) (Supplementary Fig. 1). Therefore, although focusing on AAV patients with renal involvement, we conclude that the male sex was turned out to be not a good predictor of ESRD during follow-up.
We wondered whether male sex may differently affect the cumulative patients' survival rates among AAV-subtypes. Therefore, we conducted the Kaplan-Meier survival analysis for comparing the cumulative patients' survival rates between male and female patients in each AAV subtypes. Among MPA patients, male patients exhibited a significantly lower cumulative survival rate than female patients. However, no significant difference in the cumulative survival rates was observed between male and female patients among GPA patients (Supplementary Fig. 2). On the other hand, since all EGPA patients survived during the follow-up period, the analysis regarding the clinical significance of sex for all-cause mortality was not performed in EGPA patients. With these results, we conclude that the male sex could reduce significantly the cumulative patients' survival rates in MPA patients compared to GPA patients. However, in real clinical settings, since there are not a few cases where the differential diagnosis between MPA and GPA may be difficult, we intend to maintain the current title including AAV patients rather than MPA patients.
In this study, variables with P value less than 0.005 in the univariable Cox hazard model analysis were restrictively included in the multivariable analysis. However, since we cannot ignore the variables that were found to be associated with mortality in previous studies, we considered including these variables in multivariate analysis. Since BMI showed a ‘U shape’ contribution to the rate of all-cause mortality, BMI cannot be included in the multivariable analysis. Whereas, ANCA type was reported to be associated with the mortality rate or the infectious cause of death in AAV patients.13 Therefore, we consider including MPO-ANCA (or P-ANCA) and PR3-ANCA (or C-ANCA) in the multivariable Cox hazards model analysis, however, both of them exhibited too low statistical significance in the univariable analysis to be included in the multivariable analysis. On the other hand, CRP tended to be significantly associated with all-cause mortality during the follow-up period (P = 0.073) and furthermore, an index consisting of CRP and other variables was reported to be an independent predictor of all-cause mortality in AAV patients.14 Therefore, we conducted the multivariable Cox hazards model analysis by including CRP. However, similar to the results from Table 3, only male sex and FFS at diagnosis exhibited statically significant HR in the multivariable analysis, despite the addition of CRP. Therefore, we decided to maintain the results of Table 3.
The retrospective design might weaken the power of the clinical implication of the sex difference that our study provided. Also, the number of patients was not large enough to represent all Korean patients with AAV. However, this study might be valuable in that this is the first study which provided information regarding the differences in the clinical features and prognosis in the course of AAV between male and female AAV patients in Korea. Also, the limitation of the monocentric study may paradoxically minimise the inter-centric variation or bias, which could enhance the reliability of our study. Most deaths from septic shock or cancer were more frequent than death from persistent haemoptysis or damage to major organs such as the brain and heart. However, since there were many cases in which it was impossible to accurately classify the cause of their death, this study used the item of all-cause mortality without classifying death by cause, which was an additional limitation of this study. We believe that a prospective future study with a larger number of patients by recruiting the institutes, where the same inclusion criteria can be applied and the electronic medical records can be shared, will provide more reliable and valuable information.
In conclusion, male sex did not affect the clinical features at diagnosis, however, it increased the rate of all-cause mortality during the follow-up of AAV and was proved to be an independent predictor of all-cause mortality in AAV patients.
 XML Download
XML Download