

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Poisoning is one of the leading causes of morbidity and mortality in the United States.1 According to an annual report by the American Association of Poison Control Centers' National Poison Data System, more than 2.0 million cases of poisoning occurred in 2018 alone, which resulted in approximately 1,300 poisoning-related deaths.2 The in-hospital mortality rate of poisoned patients is approximately 0.5%.3 However, deaths from poisoning reported to the Poison Control Center in the United States accounted for only 5% of the actual deaths.4 In the Republic of Korea, the number of poisoned patients has been gradually increasing; in 2015, more than 32,000 patients visited the emergency room (ER) for poisoning.5 The in-hospital mortality rate of poisoned patients is 1.6–7.9%.567
The identification of the substance causing the poisoning and the time taken to reach the hospital after exposure are related to the patient's prognosis.8 For certain substances, the appropriate treatment such as antidote or decontamination therapy can be important. In addition, even if a substance does not affect treatment, it can help doctors determine the treatment direction for patients with unclear diagnoses.9
It is difficult to determine whether a patient has been poisoned and, if so, what toxins caused the poisoning. This is usually determined by history taking and physical examination. In particular, the diagnosis of herbicide poisoning relies mostly on history taking.10 However, poisoning can present a variety of clinical signs and symptoms, which may be the only clues for diagnosis.8 Therefore, it is often difficult to differentiate poisoning from other diseases based on clinical symptoms alone, and there are various types of toxic substances that may cause similar clinical manifestations. Furthermore, many patients tend to withhold details about the cause of their poisoning. In such cases, additional unnecessary tests may be performed. As a result, patients may not receive timely adequate treatment, and thus may spend a longer time in the ER.
Given the wide variety of toxins in poisoned patients who visit the ER, it is difficult to maintain a toxicology laboratory in a single hospital owing to problems with time, manpower, and cost.11 Although toxicology screening tests have been developed and used to differentiate poisoned patients, their use is limited.
The Intoxication Analysis Service, which was started in June 2017, is a cooperative project between our hospital and the Forensic Toxicology Division of the National Forensic Service, Republic of Korea. This project uses systematic toxicological analysis (STA) to confirm the presence of poisoning and detect the type of toxin. Ultimately, the aim is to improve the quality of treatment for intoxication. In this study, clinical diagnosis and toxicology laboratory results were collected. We also evaluated whether changes occurred in treatments and physician's decisions after the initiation of the Intoxication Analysis Service.
METHODS
Intoxication Analysis Service process
The Intoxication Analysis Service was established in our hospital in cooperation with the National Forensic Service to solve problems arising from the diagnosis of intoxicated patients. If STA is determined to be necessary, the test is performed after providing an explanation to patients and obtaining their consent. Furthermore, the test is performed without charge. A sample of the patient's blood, urine, or gastric lavage or the suspected substance itself is collected in the ER. The emergency physician requests the STA via the social network service (SNS) and shares encrypted patient information, the reason for the analysis request, and information on the toxic substances and patient's condition. Thereafter, the documented patient information and specimens are sent to the National Forensic Service, which is 15 minutes (4.6 km) away from our hospital. The whole blood sample is transferred after injecting it into a vacuum tube, and other samples are transferred into a sealed container. Gas chromatography/mass spectrometry (GC/MS) or liquid chromatography-tandem mass spectrometry (LC-MS/MS) is used to analyze drug or poison components in the blood; if necessary, a quantitative analysis is performed to determine whether the blood concentration is within the toxic range. The STA laboratory provides opinions on causative substances based on the patient's information and analysis results. The results of the analysis are first reported using the SNS. Through the SNS, physicians and the STA laboratory can easily discuss the analysis results. When the cause of the patient's poisoning is determined after discussion, the result is finally reported in a document. Since April 2019, information exchange via the Internet has enabled faster sample requests and receipt of results, and physicians can check the results by visiting the website of the National Emergency Medical Center (www.e-gen.or.kr).
Systematic toxicological analysis
Sample preparation and detection are performed based on the chemical structure and properties of the target substance. The following types of substance are used in the classification based on chemical structure and property: lipophilic compounds such as typical antipsychotic drugs and synthetic pyrethroids; hydrophilic or ionic moiety compounds such as paraquat, glyphosate, and glufosinate; and volatile solvents such as methanol, xylene, and toluene. For analyzing lipophilic compounds, 1-mL of a blood or urine samples are collected and introduced into a solid-phase extraction system. The eluted samples are concentrated and injected into the GC/MS and LC-MS/MS systems. For hydrophilic or ionic moiety compound, 0.2 mL of acetonitrile is added to 0.1-mL blood and urine samples, which are then homogenized via sonication and finally centrifuged. The supernatants are then injected into the GC/MS and LC-MS/MS systems. Next, 0.5-mL blood and urine samples required for volatile solvent analysis are directly injected into the GC/MS system using solid-phase microextraction.
Study design and population
To determine the changes in the management of poisoned patients before and after the implementation of the Intoxication Analysis Service, we collected the data of poisoned patients who were admitted to the ER of Wonju Severance Christian Hospital from June 2014 to May 2020, which is a tertiary university hospital. The patients were divided into two groups and compared: before-service group (from June 2014 to May 2017) and after-service group (June 2017 to May 2020).
Patients who (1) were discharged against medical advice, (2) were transferred to another hospital; (3) arrived at the ER in arrest status, (4) were discharged from the ER without hospitalization owing to mild symptoms or low toxicity of toxic substances, or (5) presented to the ER owing to CO poisoning, insect bites, or snake bites that did not require poisoning analysis were excluded.
STA was conducted in patients who visited the hospital between June 2017 and May 2020. The indications for STA were as follows: (1) toxic substances known at the time of arrival in the ER, to confirm the known substance; (2) toxic substances not identified by medical history, to confirm substances suspected by the medical staff after physical examination; (3) symptoms appearing to be due to exposure to unknown substances; and (4) reason for altered mental status not known after laboratory tests, brain evaluation, and spinal tap findings to rule out poisoning.
STA was not used for some patients when the toxins they were exposed to could be analyzed in the hospital; if the patient was clinically diagnosed and conservative treatment was possible because the symptoms caused by a known substance were minor, it was judged that STA would be unnecessary.
Data collection
Patient data were collected retrospectively by a board-certified emergency physician. The patient's age, sex, history, physical examination findings, prognosis, and toxicity analysis results were assessed. The STA results were recorded in electronic medical records. The reason for the analysis, the time taken to report the results, and the STA results were recorded and evaluated. Intoxication analysis results were classified based on the type of toxic substance detected, such as medical drugs, agrochemicals, and other natural poisons such as mushrooms and plant roots.
Statistical analyses
The general characteristics of the participants, laboratory findings, and clinical parameters are presented as mean ± standard deviation or median (interquartile range) for continuous variables and as frequencies (percentages) for categorical variables. The differences between the patients who experienced poisoning before and after implementation of the analysis service were assessed using an independent t-test for continuous variables and χ2 test and Fisher's exact test for categorical variables. All statistical analyses were performed using IBM Statistical Package for the Social Sciences Statistics for Windows version 25.0 (IBM Corp., Armonk, NY, USA), and the significance level was set at 0.05.
RESULTS
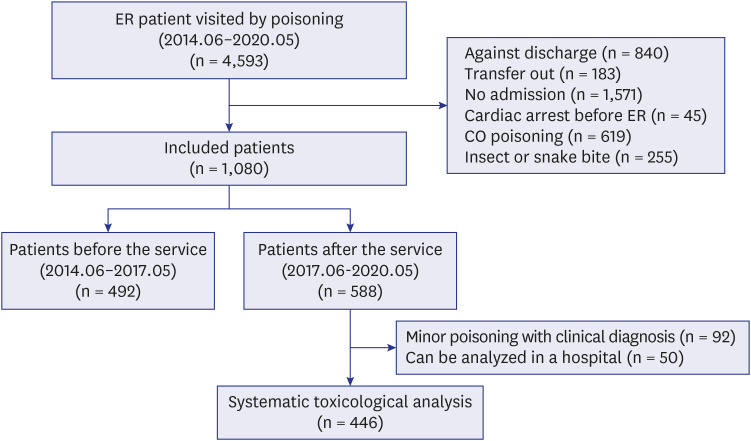
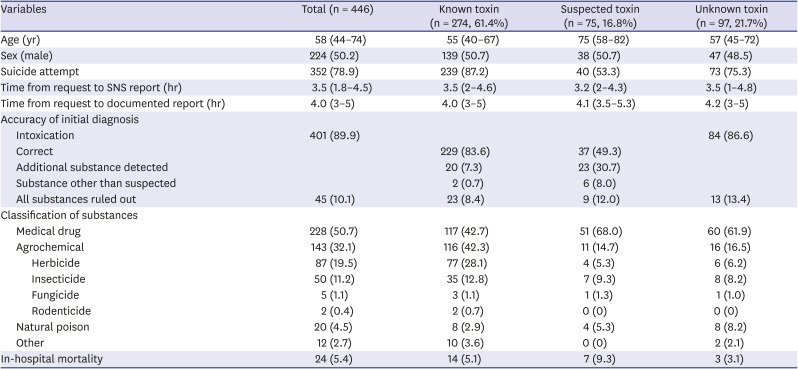
During the study period, 4,593 patients visited the ER for poisoning. A total of 1,080 patients were included in the analysis: 492 patients admitted to the ER within the 3-year period before the start of the service and 588 patients admitted to the ER during the period after the service. Of the 588 patients in the after-service group, 446 (75.9%) were subjected to STA, and 274 of these patients (61.4%) were referred for analysis to confirm their exposure to known toxins via history taking. A total of 75 patients (16.8%) were referred for confirmation of substances suspected owing to symptoms and physical examination findings. STA was performed for 97 patients (21.7%) who visited the ER for poisoning but had no toxic substances identified or suspected (Fig. 1). The other 54 patients visited the ER with altered mental status, and STA was requested when the cause of the decreased mental status was not identified after brain imaging, laboratory tests, and a spinal tap.
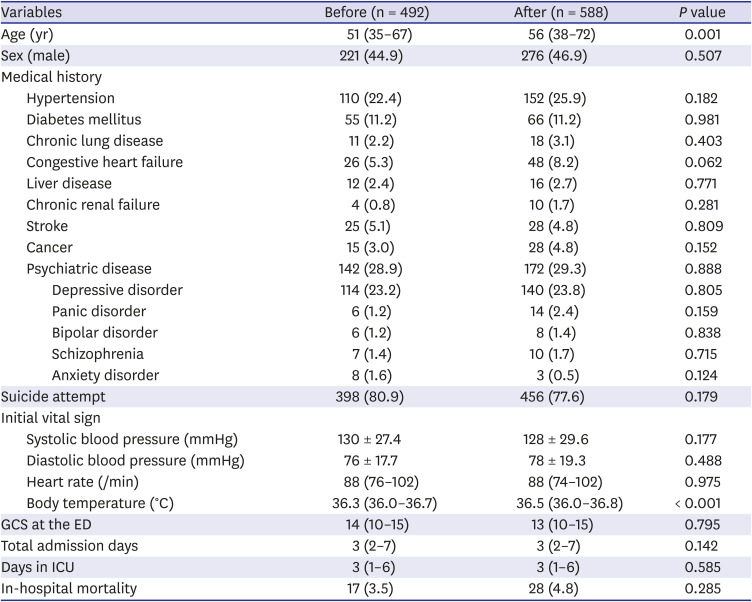
Changes before and after the project were analyzed by comparing the characteristics of patients. Table 1 shows a comparison of patient characteristics and laboratory results. The baseline characteristics of the two groups showed no significant differences, except for median age (before vs. after: 51 vs. 56 years) and body temperature (before vs. after: 36.3°C vs. 36.5°C). Men accounted for 44.9% and 46.9% of the before-service and after-service groups, respectively. Psychiatric diseases (28.9% and 29.3%) were the most common diseases based on the medical history of patients, and depressive diseases accounted for the majority. Intentional poisoning occurred in 80.9% and 77.6% of patients in the before-service and after-service groups, respectively. Finally, 17 and 28 in-hospital deaths occurred in the before-service and after-service periods, respectively. These differences between the groups were not statistically significant.
Table 1
Baseline characteristics, medical histories, and clinical parameters of patients with poisoning before and after implementation of the Intoxication Analysis Service
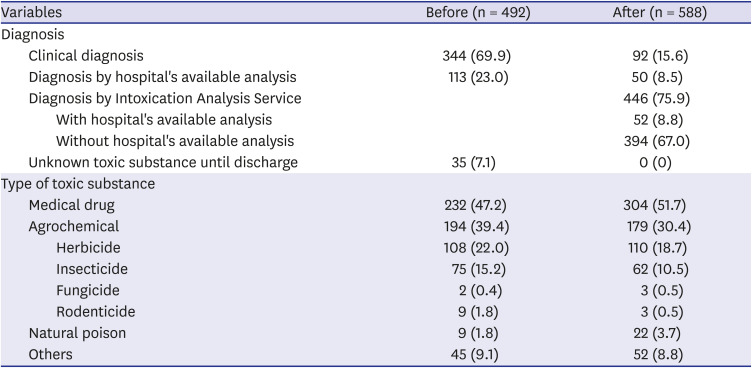
In the before-service group, most of the poisoned patients were clinically diagnosed. A total of 113 cases were diagnosed according to the hospital's available toxicological test. However, most cases of poisoning (69.9%) were caused by toxins that could not be tested using the hospital's available toxicological test; in 35 patients, the causative substance could not be determined until discharge. After the start of the service, 50 patients were diagnosed by only the hospital's available toxicological test, and 446 were diagnosed through STA at the National Forensic Service. Approximately 84.4% of the patients had a confirmed diagnosis. As a result, all of the causative substances were eventually identified. In the before-service group, 47.2% of the patients were poisoned by medical drugs, 39.4% were poisoned by agrochemicals, and 1.8% were poisoned by natural poisons. After the service, the proportions of substances that caused poisoning were as follows: 51.7% medical drugs, 30.4% agrochemicals, and 3.7% natural poisons (Table 2). The detailed classification of the substances shows the changes in the proportion of agrochemicals and natural toxins detected before and after STA. Glufosinates and organophosphates were the most frequent herbicides and insecticides that caused poisoning. Among the natural toxins, veratramines and aconitines were the most common causes of poisoning (Supplementary Tables 1 and 2).
Table 2
Diagnosis results of patients who visited the emergency room owing to poisoning before and after implementation of the Intoxication Analysis Service
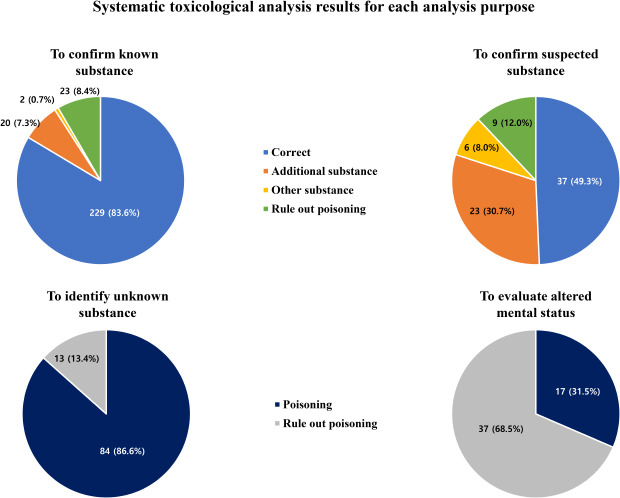
The STA results of the patients who were referred were consistent with the drugs identified in the history taking in 83.6% of patients. In addition, 20 patients (7.3%) were found to have additional toxic substances other than the requested substance, and two patients (1.1%) were found not to be poisoned by the requested substance but were poisoned by a completely different substance. Another 23 patients (8.4%) were not actually poisoned. Most of these patients were poisoned by medical drugs (42.7%) and agrochemicals (42.3%).
In the group that underwent STA to confirm the suspected substances, the accuracy of clinically confirming the suspected substance reached 49.3% compared with the results of the toxicity analysis. In addition to the suspected substance, 30.7% of the patients had additional substances. Furthermore, 8% of patients were found to have other causes of poisoning, whereas 12% showed no toxic substances on STA.
In 97 intoxicated patients whose causative agent was unknown, 13.4% were not actually poisoned and were discharged alive. In 86.6% of patients, the toxic substances could be identified using the STA, as medical drugs, agrochemicals, and natural poisons accounting for 61.9%, 16.5%, and 8.2% of the toxic substances, respectively. Three of these patients died in the hospital. In all patients who underwent STA, a median of 4 hours was required to confirm the results in a document, and the results were obtained in a median of 3.5 hours via the SNS (Table 3).
Table 3
Characteristics of patients who underwent systematic toxicological analysis
After STA, 53 patients were either confirmed to be poisoned by a completely different substance or were not actually poisoned, and their treatment plan was changed (Supplementary Table 3). For patients whose diagnosis was changed because of STA, it was confirmed that 47.8% of these patients were unnecessarily admitted to the intensive care unit (ICU); the others required continuous ICU care for concomitant conditions such as aspiration pneumonia or other severe poisoning. In addition, among patients admitted to the general ward, 63.3% were discharged after undergoing STA, excluding those who were still hospitalized to undertake additional evaluation such as psychiatry management.
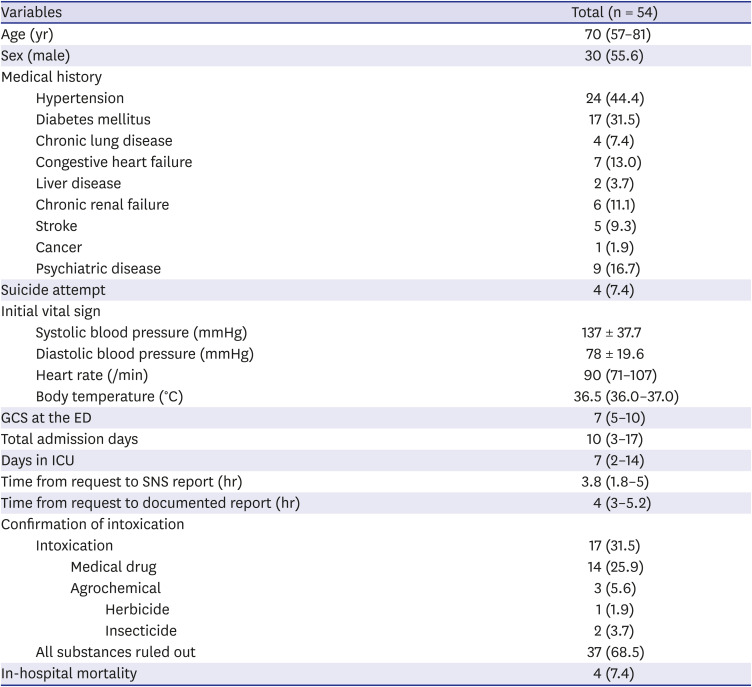
Among 54 patients with altered mental status due to an unknown cause, 17 patients (31.5%) experienced this condition due to poisoning. Among these patients, four revealed that they were intentionally intoxicated after their conscious level improved. Intoxication was ruled out in 37 patients (68.5%), and only four in-hospital deaths occurred. Among the 17 patients in whom altered mental status was associated with poisoning, 14 cases were caused by medical drug intoxication, one was caused by ingestion of herbicides, and two were caused by ingestion of insecticides (Table 4).
Table 4
Characteristics of patients who underwent systematic toxicological analysis to identify the cause of loss of consciousness
DISCUSSION
This project comprises a new system in the Republic of Korea in which hospitals and national institutions participate, allowing a hospital to request toxicity analysis via the SNS and the Internet. Quick and easy information sharing is possible using the SNS, web pages, and documented records. The National Forensic Service, responsible for criminal investigations and autopsies, can conduct toxicological analysis using vast amounts of toxicology data, thus enabling more accurate and wider analysis than the toxicological analysis performed in other laboratories. In particular, it is possible to conduct a toxicological analysis to detect the presence of natural poisons and industrial substances, including various pesticides marketed in the Republic of Korea (Supplementary Tables 1 and 2). Furthermore, the National Forensic Service is able to obtain clinical information of patients by analyzing clinical records of actual patients. By comparing the results of qualitative and quantitative plasma analyses with the patients' information, valuable data on toxic substances were accumulated. Furthermore, this allowed doctors to make quick and accurate treatment decisions and obtain information on poisoning trends in the community.
In the past, the clinical effectiveness of toxicology laboratory analysis has been underestimated for several reasons. First, it was thought that poisoning could be diagnosed by clinical information only. Second, conservative treatment is sufficient for treating intoxication; therefore, even if toxic substances were identified by laboratory analysis, the treatment chosen did not usually change clinically. Third, comprehensive analysis results are reported after the initial critical treatment has already been initiated, and screening tests with short report times have limited confirmatory ability. Finally, the costs associated with equipment, specialists, and training for the STA are high and often overused; therefore, the gain versus loss is not significant.11121314 However, given that many changes have been made in the diagnosis and treatment of poisoning, the perception of STA is also changing.
Medical history documentation in the ER is often inaccurate because of the urgency of the situation, the patient's condition, and the hospital's unfamiliarity with the patient. In particular, the patient's medication history, including cardiac medications, neuropsychiatric agents, analgesics, and hypnotics, is often inaccurate.151617 In addition, a previous study stated that the accuracy of medication history of patients in the ER is 13–36.3%.161718 In several previous studies, drugs other than those identified by medical history were found in the laboratory analyses of 20–25% of poisoned patients, and the drug components stated in the medical history were not detected in 16–23% of patients.1920 Therefore, it is difficult to determine the exact cause of intoxication by taking a medical history or conducting a doctor's examination alone. In the case of multidrug co-ingestion, the effect of one drug may mask that of the other drug. For intoxicated patients, it is possible to obtain accurate information about the toxic substances by conducting a toxicology laboratory analysis rather than by taking a history alone.2021
In the present study, before implementation of the service, 69.9% of intoxicated patients were diagnosed clinically. In addition, the toxic substances in 7.1% of the patients were not identified until discharge. On the contrary, after starting the service, 84.4% of patients were diagnosed by laboratory analysis, and 15.6% did not require STA. There was also a difference between the clinical diagnosis of poisoned patients and the substances identified by comprehensive STA. In 13.4% of patients diagnosed as poisoned with an unknown substance, poisoning was ruled out based on the STA result. It was possible to identify the unknown substances in 86.6% of patients, in whom the toxic substance would have been difficult to detect without STA. In patients whose toxic substance was suspected during the physician's examination but not during the history taking, only 49.3% of the actual analysis results matched. Among these patients, other additional substances were identified in 30.7%, 8% had poisoning caused by completely different substances, and 12% had no identifiable toxic substances. Even in patients in whom toxic substances were identified during the history taking, the actual toxic substances were matched in 83.6% of these patients, other additional substances were detected in 7.3%, completely different substances were confirmed in 0.7%, and the diagnosis of poisoning was excluded in 8.4%. These patients would have been treated for an incorrect clinical diagnosis if the STA had not been performed. The diagnostic usefulness of STA was also compared before and after the implementation of the service at our institution. When comparing these two groups, there were no patients in whom the cause of poisoning could not be identified after starting the service. Additional substances in which the effect may have been masked could be discovered, and the causes of poisoning in patients in which the toxic substance was unknown were also identified. Accurate toxicological analysis will prevent patients in need of an antidote from missing appropriate treatment owing to an incorrect diagnosis. Some antidotes may not be helpful for treating patients if they are used incorrectly and can even be harmful.22 Distinguishing the type of poisoning and determining plasma concentrations of the toxic substance can help clinicians determine whether a patient will need further treatment or observation.920 In a previous study, conducting a toxicological analysis in poisoned patients with uncomplicated, stable, or no specific symptoms reduced the unnecessary hospitalization rate by 21.7% and unnecessary ICU admission rate by 53.3%.23 After the Intoxication Analysis Service was started, the total admission days, days in ICU, and in-hospital mortality did not decrease. However, in the subgroup analysis in which the clinical diagnosis was changed according to the STA results, unnecessary ICU admission was reduced by 47.8% and the unnecessary hospitalization rate was reduced by 63.3% (Supplementary Table 3). Because the present study included patients who required hospitalization, conducting a direct comparison between our results and those of previous studies is difficult. However, STA can reduce unnecessary use of medical resources.
Table 4 shows the results of patients with altered mental status in whom the cause could not be determined via blood and imaging tests, and the altered mental status in 31.5% of these patients was found to be caused by poisoning. This finding is similar to that of previous studies showing that 19–31% of patients visited the ER for altered mental status due to poisoning.242526 In this way, if other causes are excluded for patients with altered mental status, STA will facilitate determining the appropriate treatment. STA will also help physicians learn others' opinions while deciding whether a patient should be admitted or discharged and prevent the unnecessary use of medical resources. In addition, identifying the causative agent that caused the altered mental status helps prevent its recurrence. It will provide information on which drug can affect the patients' level of consciousness, and these data will be valuable not only for the medical staff but also for the health authorities.27
There are several methods for conducting drug analysis. However, according to each method, the materials used for the analysis vary and the time to obtain the results differs.28 Among these methods, spot tests, thin layer chromatography, and immunoassays are often used as toxicity screening tests in hospitals. These screening methods are simpler to perform and can obtain quicker results than comprehensive tests, but they have some limitations.2930 Screening is usually aimed at quickly discriminating against a specific type of intoxication that occurs frequently. In other words, extensive testing for unknown poisonous substances is impossible. Intoxication cannot be ruled out even if a negative result is obtained from the screening test. In addition, given that screening is not intended to be a quantitative test, it cannot be confirmed whether the identified substance was at a concentration sufficient to cause the patient's symptoms even if the test was positive.31 A screening test alone can lead to false negatives and false positives when used to diagnose poisoning; therefore, errors may occur during the interpretation of results if confirmatory tests are not performed.30 Furthermore, comprehensive toxicology laboratory analysis is not only useful for diagnosis and treatment but also for developing toxicology screening tests that are applicable to patients with poisoning or altered mental status. Considering that the main causes of poisoning differ depending on the region, it is difficult to apply a uniform screening test. Based on the results of the comprehensive test, data on the major toxins found in the region can be obtained. This could be the basis for developing reliable screening tests that can be used in other hospitals and areas where a comprehensive toxicology analysis is not available.
In general, the results of quantitative serum toxicology tests should be reported within 1 hour.28 Moreover, it is recommended that some antidotes must be administered within 1 hour.32 However, studies on the time of antidote administration are lacking, and some antidotes can still be helpful even after a longer period of time.22 In the analysis of our results, the time from the request of the analysis to the time that the results were obtained via the SNS took a median of 3.5 hours. This period seemed to have increased owing to some extremes, and it may be the reason why no sample analysis was performed on weekends or holidays or at night. This is because the analysis was conducted outside the hospital; hence, it was difficult to perform on holidays or at night unless the sample was specifically requested. Furthermore, it took some time for the sample to be transferred to the analysis center after the request. Hence, we could infer that the time from the analysis request to the documentation of the results was a median of 4 hours. The STA methods performed in this study were liquid chromatography (LC) and gas chromatography (GC), which are relatively complicated and time consuming compared with screening tests.
As mentioned above, if the test is performed in a hospital, the results can be obtained immediately, but there are limitations to maintaining a toxicology laboratory in a hospital. Therefore, national support for the analysis of patients with acute poisoning is required. Furthermore, specialized STA tools for clinical use, such as an analysis center that can readily be used for testing, is needed.
This study has several limitations. First, the study was conducted as a retrospective study using chart review, which may result in errors or missing data. Second, requests for samples to be analyzed by the National Forensic Service were made by various emergency medical doctors according to their schedules. Therefore, there may be inconsistencies in determining which patients would be analyzed using STA. Third, if the patient's symptoms were mild or if the cause of the change in mental status was clear, the test would not be performed. Therefore, the characteristics of the intoxicated patients in our analysis may not represent all intoxicated patients. Fourth, blood and urine samples were analyzed in most cases, but other various types of samples were also used, such as actual substance or lavage fluid samples. Furthermore, the time from poisoning to sample collection differed. This may have had some effect on the STA results. Finally, this study did not compare the screening test results. Further studies in which the screening test and the comprehensive test are performed together will show the pros and cons of each method.
The STA results in some poisoned patients differed from the clinical diagnosis. STA is also helpful in the differential diagnosis of intoxication in patients with altered mental status. Therefore, the proper use of STA by emergency physicians can increase the accuracy of the diagnosis of poisoning and help in making treatment decisions.
 XML Download
XML Download