

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Diabetes mellitus is a metabolic disorder characterized by hyperglycemia with impaired insulin function. The prevalence of diabetes is rapidly increasing worldwide, including Korea.12 Also, the age of developing diabetes is shifting toward a younger population, especially in Asian countries. The prevalence of type 2 diabetes in adolescence is rapidly posing major clinical challenges and public health burden worldwide in the 21st century.3
Previously, type 1 diabetes was known as the most common form of diabetes among young people.4 However, the prevalence of type 2 diabetes is increasing in Asian ethnicity.
Furthermore, diabetes among youth shows an aggressive clinical course and reduced life expectancy. Youth with type 2 diabetes exhibit more rapid deterioration of β-cell function.5 They have an earlier presentation with complications such as chronic kidney disease.678910 They also have greater mortality compared to type 1 diabetes and adults with type 2 diabetes.81112 Thus, monitoring the prevalence of diabetes and pre-diabetes is relevant for public health programs in each country. Obesity is a condition of excess body fat that negatively affects an individual's health. Meanwhile, childhood obesity is linked to immediate and long-term health risks, including impaired fasting glucose (IFG).13 IFG in childhood significantly increases later risk of type 2 diabetes and cardiovascular disease.14
Thus, the objectives of this study were as follows: 1) to update the most recent suspected prevalence of diabetes and pre-diabetes of Korean adolescents aged 10 to 18 years; 2) to examine the changes in prevalence of diabetes and pre-diabetes between 2007 and 2018; and 3) to examine whether the changes of obesity prevalence in these age groups are related.
Go to : 
METHODS
Study population and data collection
This study was performed using data acquired from the Korea National Health and Nutrition Examination Survey (KNHANES) IV to VII.15 KNHANES was a cross-sectional and nationally representative survey with a multistage and stratified sampling design conducted by the Division of Chronic Disease Surveillance, Korea Centers for Disease Control and Prevention. KNHANES have been conducted periodically since 1998 to assess the health and nutritional status of the non-institutionalized civilian population. This study was performed using the KNHANES IV to VII data (2007–2018), which was regularly performed by ordinal 3-year cycles. All subjects and their parents were interviewed at home after informed consent and underwent various examinations, including blood sampling.
A total of 10,735 subjects (5,670 male and 5,065 female) aged 10.00 to 18.99 years were identified as potential subjects for this study. Those with incomplete data for a standardized physical examination and lab test were excluded. Thus, the final analytical sample consisted of 8,718 subjects (81.2%; male = 4,642, female = 4,076).
All anthropometric measurements were performed by well-trained examiners who used a standard protocol for all four KNHANES cycles. Weight was determined to the nearest 0.1 kg on a medical balance (GL-6000-20, CAS, Seoul, Korea); height was measured to the nearest 0.1 cm with a wall-mounted stadiometer (Seca 220, Seca, Hamburg, Germany). Body mass index (BMI) was calculated by dividing the weight (kg) by the height squared (m2). Blood samples were collected in the morning after fasting for at least 8 hours. Fasting plasma glucose was measured by Hitachi Automatic Analyzer 7600 (Hitachi, Tokyo, Japan). Hemoglobin A1c (HbA1c) was measured using a high-performance liquid chromatography method (HLC-723G7; Tosoh, Tokyo, Japan).
Definition of each criterion
Diabetes cases were defined as subjects who had been previously diagnosed by a doctor based on a self-report or based on the survey results; fasting plasma glucose (FPG) levels of ≥ 126 mg/dL (7.0 mmol/L) and/or HbA1c levels of ≥ 6.5%. Pre-diabetes was defined as FPG levels of 100–125 mg/dL (5.6–6.9 mmol/L). Overweight and obesity were defined by BMI using the 2017 Korean CDC growth charts.16 Overweight was defined as age- and sex-specific 85th ≤ BMI < 95th percentile and obesity as BMI ≥ 95th percentile.
Statistical analyses
The prevalence of diabetes and pre-diabetes was calculated using KNHANES-VII data. Wilson method was used to estimate 95% confidence interval (CI) since the prevalence estimates were close to zero.17 The χ2 test and analysis of variance was used to compare the differences for proportions and mean among the KNHANES cycle. To test the trends from KNHANES-IV to VII (2007–2018), logistic regression analyses was used with the KNHANES cycle as a continuous variable predicting diabetes and pre-diabetes prevalence. Nominal variables presented as the number and percentage, and continuous variables presented as mean ± standard deviation (SD). All statistical analyses were performed using SPSS 17.0 for Windows (SPSS Inc., Chicago, IL, USA). P value < 0.05 was considered significant.
Ethics statement
The present study protocol was reviewed and approved by the Research Ethics Committee of the Korea Center for Disease Control (approval No: 2020-06-009). The Institutional Review Board waived informed consent.
Go to :
RESULTS
Characteristics of the study subjects
The characteristics of the study subjects analyzed, stratified according to the KNHANES cycle, are summarized in Table 1. The current age of the study subjects was 13.7 ± 2.5 years. In total subjects, the mean BMI and fasting glucose increased according to the KNHANES cycle. The prevalence of obesity increased according to the KNHANES cycle (P trends < 0.001). Males had higher mean BMI (20.9 ± 3.9 vs. 20.1 ± 3.5, P < 0.001) and higher FPG levels (91.0 ± 7.9 vs. 89.5 ± 8.9 mg/dL, P < 0.001) than female subjects.
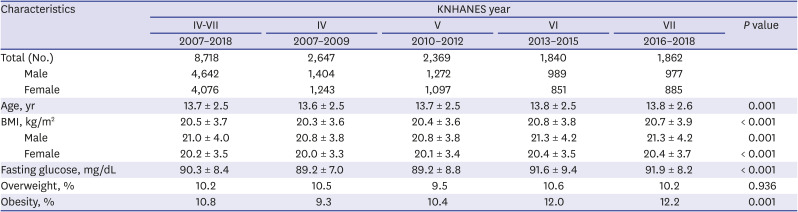
Table 1
The characteristics of the study subjects from 2007 to 2018
![]()
A total of 26 subjects (male; 14) were diagnosed with diabetes; 4 subjects were previously diagnosed by a doctor (diabetes awareness was 15.4%), and 1 subject was treated with insulin (3.8%). Twenty subjects were diagnosed by fasting glucose ≥ 126 mg/dL, and 16 subjects were diagnosed by HbA1c ≥ 6.5%, 10 of these met both criteria. The mean age of diabetic subjects was 13.5 ± 2.4 years, their BMI and fasting glucose level was 23.0 ± 5.9, and 165.5 ± 63.9 mg/dL.
Trends and prevalence of diabetes and pre-diabetes during the KNHANES IV (2007–2009) to VII (2016–2018)
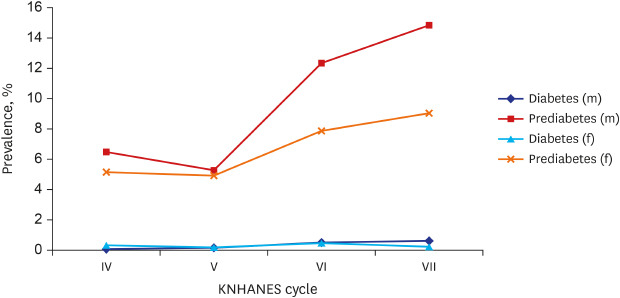
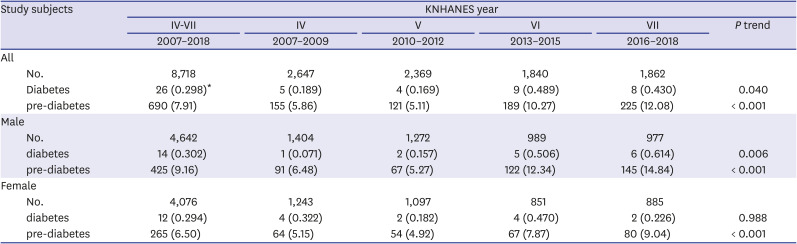
The prevalence of diabetes and pre-diabetes by ordinal 3-year cycles for total, male, and female subjects are presented in Table 2. The overall suspected prevalence of diabetes and pre-diabetes in the KNHANES IV–VII was 0.298% (95% CI, 0.204–0.437) and 7.914% (95% CI, 7.370–8.504). During the KNHANES cycles, a positive linear trend is significant for diabetes (P trends = 0.048) and pre-diabetes (P trends < 0.001) after adjusting age. The trend for diabetes is significant only in male subjects (P trends = 0.006), pre-diabetes is significant in both sexes. The suspected prevalence of diabetes was 0.189%, 0.169%, 0.489%, and 0.430% in KNHANES IV, V, VI, and VII, representing a relative increase of 127%. The suspected prevalence of pre-diabetes was 5.86%, 5.11%, 10.27%, and 12.08%, representing a relative increase of 106%. The overall changes in the prevalence of diabetes and pre-diabetes according to KNHANES cycles by sex are depicted in Fig. 1.
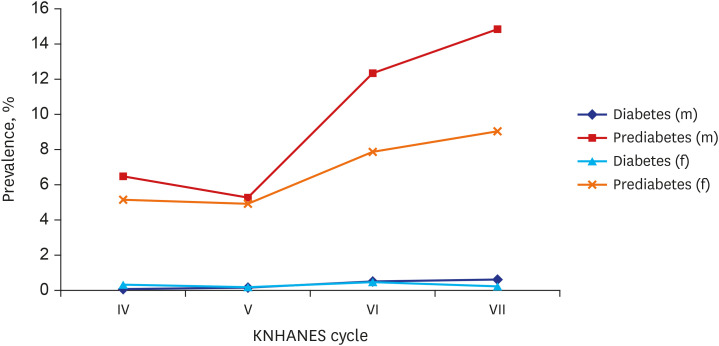 | Fig. 1The prevalence of diabetes and pre-diabetes during the four KNHANES cycles by sex.The trend for diabetes is significant only in male subjects (P trends = 0.006), pre-diabetes is significant in both sexes. The prevalence of diabetes was 0.189%, 0.169%, 0.489%, and 0.430% in KNHANES IV, V, VI, and VII. The prevalence of pre-diabetes was 5.86%, 5.11%, 10.27%, and 12.08%.
KNHANES = Korea National Health and Nutrition Examination Survey.
|
Table 2
The suspected prevalence of diabetes and pre-diabetes from 2007 to 2018 by sex
Values are presented as number of participants (%). The suspected prevalences were age-adjusted to the 2007 KNHANES data.
*The percentage of total diabetes that was undiagnosed. Diabetes was based on having a hemoglobin A1c level of 6.5% or more, FPG level of 126 mg/dL or more. Pre-diabetes was based on FPG level of 100–125 mg/dL.
![]()
Prevalence of diabetes and pre-diabetes according to obesity status
The prevalence of diabetes among normal weight, overweight, and obese were 0.19%, 0.34%, and 1.06%, respectively. The prevalence of pre-diabetes were 6.98%, 11.51%, and 11.50%, respectively. Overweight subjects exhibit a 1.3-fold higher prevalence of diabetes (odds ratios [ORs], 1.283; 95% CI, 0.342–4.818) and a 1.05 fold higher prevalence of pre-diabetes (ORs, 1.048; 95% CI, 0.823–1.335) than non-obese subjects. Obese individuals exhibited a 5.2-fold higher prevalence of diabetes (ORs, 5.223; 95% CI, 2.363–11.542) and a 1.6-fold higher prevalence of pre-diabetes (ORs, 1.607; 95% CI, 1.293–1.997) than non-obese individuals. The overall changes in the prevalence of diabetes and pre-diabetes according to obese status and sex during the four KNHANES cycles are depicted in Fig. 2.
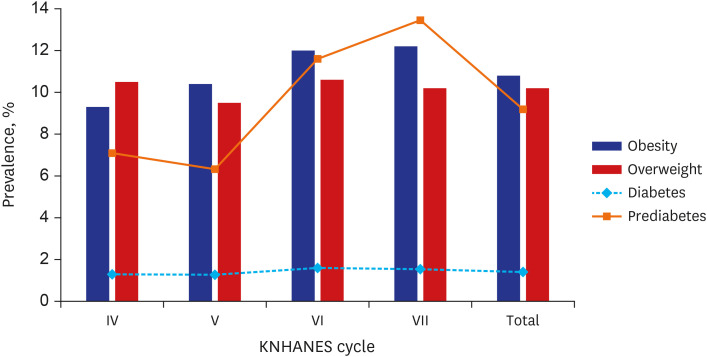 | Fig. 2The prevalence of diabetes and pre-diabetes during the four KNHANES cycles according to obesity status.The prevalence of diabetes among normal weight, overweight, and obese were 0.19%, 0.34%, and 1.06%, respectively. The prevalence of pre-diabetes were 6.98%, 11.51%, and 11.50%, respectively.
KNHANES = Korea National Health and Nutrition Examination Survey.
|
Go to :
DISCUSSION
In this study, we are using data of a national survey conducted in Korean adolescents aged 10–18 years. We found the recent suspected prevalence of diabetes and pre-diabetes or IFG was 0.298% and 7.91%, respectively. We also examined significantly increased trends in the prevalence of diabetes and pre-diabetes during 2007 and 2018. The prevalence of obesity also increased in this age group; it might be partly attributed to the increasing prevalence of diabetes and pre-diabetes.
The increasing prevalence of diabetes is a health problem that most countries are concerned about. The prevalence varies by race, but overall, it has increased compared to the past. In the USA, the prevalence of diabetes in adolescents aged 12 to 19 years was 0.8%, and the prevalence of pre-diabetes was 17.7% during 2005–2014.18 In particular, the T2DM prevalence of adolescents aged 10–19 years increased by 30.5% in Asian Pacific Islanders and American Indians between 2001 and 2009.19 In the UK, continuing the rise of type 2 diabetes in children and young adults; children of Asian ethnicity had a lower BMI SD score compared with white children but there was a significant increase in incidence over a decade.20 In Japan, the incidence of type 2 diabetes was 2.58/100,000 overall, with 0.80 in primary school students and 6.41 in junior high school students.21 In China, the prevalence of diabetes and IFG was 0.13% and 2.26% of children aged 10–17 years based on secondary school exams during 2013–2014.22 Fu et al.23 reported youth-onset type 2 diabetes increased from 4.1/100,000 (1995–2000) to 10.0/100,000 (2005–2010). The listed studies are difficult to compare because of the study population's different ethnic and age groups. In general, the prevalence of diabetes was higher in the USA and the UK than in Asian countries. The domestic incidence rate is close to that of China, and the increasing trend is similar to that of China. In common, the prevalence of diabetes increased with age, and obesity was also positively correlated. On the other hand, in the West, the prevalence of diabetes was high in girls, and in Asia, it was high in boys, showing a difference.
We are astonished by the results that the suspected prevalence of diabetes in Korean children and adolescents was 0.298% and more recently 0.430%. East Asian countries including Korea were known to have a very low incidence of type 1 diabetes in children and adolescents.24 The recent prevalence of type 1 diabetes in Korean individuals less than 20 years old was 0.021% in the National Health Insurance (NHI) Database.25 Considering our results, the prevalence of diabetes is 14-fold higher than the known type 1 diabetes prevalence. Therefore, it can be assumed that the remaining increased prevalence is due to type 2 diabetes and others. Obesity in East Asian diabetic patients are less common,26 but the incidence of obesity-related diabetes among Koreans is steadily increasing.27 In 2016–2017, the prevalence of diabetes in Korean adults was 0.9% in subjects aged 20–29 years and aged ≥ 30 years was 10.8%,2 a prevalence of 0.298% is reasonable in this age group.
In this study, the suspected prevalence of both diabetes and pre-diabetes significantly increased during 2007 and 2018 in Korean adolescents. In Korean adults, the prevalence of diabetes increased from 8.6% to 11.0% from 2001 to 2013 of adults aged ≥ 30 years,27 the prevalence of pre-diabetes, also increased from 21.5% to 25.0% from 2006 to 2013.28 The exact reason for this phenomenon is elusive. In general, the trend of increasing obesity closely parallels that of increasing diabetes. The prevalence of diabetes and obesity are closely linked: the twin epidemics.29 In our results, the ORs of diabetes and pre-diabetes in obese subjects compared to the non-obese subjects were 5.223 (95% CI, 2.363–11.542) and 1.607 (95% CI, 1.293–1.997). Obese children are hyper-insulinemic and have lower insulin-stimulated glucose metabolism compared with non-obese children. The amount of visceral fat is directly correlated with hyperinsulinemia and inversely correlated with insulin sensitivity.30 Also, “bad lifestyle” such as decreased physical activity and excessive nutrition is associated with diabetes.3132 Another reason may be that exposure to diabetes in utero and endocrine-disrupting chemicals.33 Changes in the awareness of pre-diabetes in youth are important because 25% of IFG were known to develop diabetes within 3–5 years.34 Early detection and management of pre-diabetes in childhood may reduce adult diabetes.
The present study has several limitations. The biggest limitation is that the diabetes prevalence derived in this study is not an actual prevalence but a suspected prevalence. Since the prevalence of diabetes prevalence in adolescents is very low, accuracy can be increased when using large-scale data such as National Health Insurance Service data. Second, we cannot distinguish type 1 from type 2 diabetes, as the KNHANES questionnaire does not make this distinction. Third, only 1 time-measured FPG without oral glucose tolerance test were used to diagnose pre-diabetes and most diabetes. Thus, the prevalence might be overestimated. Vice versa, we missed some subjects with impaired glucose tolerance. Lastly, there might be bias because approximately 18.8% of the subjects were excluded from the analysis due to missing data.
In conclusion, this study provided a recent suspected prevalence of diabetes and pre-diabetes in Korean adolescents. Although the prevalence of diabetes and pre-diabetes was still low compared to USA children and adolescents, there was an approximately 2-fold increase in diabetes and pre-diabetes over short time periods: during 2007–2009 and 2016–2018. The increasing trend of childhood obesity in Asians, including Koreans, might be one explanation. However, while the prevalence of obesity increased by 1.3 times, diabetes and pre-diabetes doubled, so it is predicted that there may be reasons other than obesity. Still, it was not easy to find other reasons through this study. Therefore, social actions, including by the government, are needed to diagnose and treat pre-diabetes/diabetes and to improve glycemic control in this age group. Further studies are also needed to elucidate which environmental factors are involved in the increasing trend in pre-diabetes/diabetes in Korean children and adolescents.
Go to :
 XML Download
XML Download