

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Telemedicine is a kind of health management practice in which medical staff and patients perform remote communication and care.12 For telemedicine for proper health management, medical devices used by patients, platforms in which data is stored and displayed, and medical feedback (service) provided by medical staff to patients must be organically harmonized.12 Due to the coronavirus disease 2019 (COVID-19) outbreak,3 the Ministry of Health and Welfare has temporarily allowed “phone consultation or prescription (PhoneTx).”4 “PhoneTx” is based on remote communication similarly as telemedicine; however, it differs in purpose and method from the existing evidence-based telemedicine.5 Conventional telemedicine aims at lifestyle management, while “PhoneTx” only aims to avoid visiting hospitals.5 Therefore, it would not be reasonable to sustain the legalization of telemedicine in the future based on this experience of telephone consultation.5 In addition, the use of telemedicine for acute diseases like COVID-19 is considered to be quite limited at this time.
The prolonged COVID-19 outbreak has provoked a dire demand for medical staff and patients to use telemedicine (non-face-to-face care). However, notably, the endpoint of the temporary allowance of PhoneTx is not clearly specified.4 As the COVID-19 outbreak prolongs, the endpoint of COVID-19 also grows uncertain.67 Feasibly, this type of telemedicine could be further prolonged and be settled in the medical fields beyond the COVID-19 outbreak.
In the face of this prolonged COVID-19 outbreak, medical staff should seriously consider preparing for evidence-based telemedicine, and not just for PhoneTx. PhoneTx could be used not only to avoid visits to the hospital (Table 1) but also as evidence-based telemedicine that is really helpful for the health management of patients.18

Table 1
Differences between phone consultation or prescription and telemedicine
![]()
Unprepared telemedicine can cause serious confusion for the medical staff and patients.2 Although the medical staff does not need to agree or disagree with telemedicine, they need to understand all medical situations and be prepared to adopt telemedicine if necessary. Therefore, assuming that the extensive use of telemedicine will be approved in Korea, in this study, we offer suggestions on how to adequately prepare for the adoption of telemedicine. Although not officially approved, the information hereby provided summarizes the actual needs based on the existing literature. The 10 suggestions provided in this document are intended for consultation purposes only and not for legal advice. The decisions of the medical staff working in the medical field are of utmost importance for situations that can take different directions. Notably, depending on the patient's situation, the medical staff may change or adjust our advice.
Go to : 
REALISTIC CONSIDERATIONS FOR STARTING THE PRACTICE OF TELEMEDICINE (Table 2)
1. Primary priority: Telemedicine cannot replace face-to-face treatment
It is crucial to remember that telemedicine can fully replace face-to-face consultation. Physicians should not forget that the basis of medical care consists of inspection, auscultation, percussion, and palpation.910 Telemedicine is based on health management systems using medical devices and platforms.1211 To this end, it is essential to consider how much medical devices and platforms can complement face-to-face medical care basics (inspection, auscultation, percussion, and palpation). Because of this, information and communications technology (ICT)-based telemedicine could not fully replace face-to-face treatment. Hence, the correct approach is to use telemedicine to supplement health care services provided to patients with certain medical conditions.12
2. Telemedicine could be used in patients who had a face-to-face meeting with the physician at least once
The first thing to know is whether the patient (disease group) is suitable for telemedicine practice.13 In this sense, telemedicine is recommended for patients who have received face-to-face attention for the same condition before.14 For example, in patients with diabetes mellitus (DM), telemedicine is recommended only for matters related to blood sugar control or the evaluation of related complications.1516 If a patient with DM experiences sudden abdominal pain or headache, face-to-face treatment is preferred. In other words, continuity between face-to-face treatment and telemedicine is important. Nevertheless, national emergencies such as COVID-19 can pose exceptional challenges.4
3. Proper consent and education are required for participating patients
If a doctor has determined that patients will be followed up using telemedicine after the first face-to-face consultation, the doctor needs to first obtain the patient's consent before starting telemedicine and document, record, and save this information.1718 To avoid unnecessary misunderstandings with patients regarding the method of telemedicine and the limitations of the technology, it is essential to provide sufficient explanation and obtain consent from the patients.19 Doctors would ideally inform users of any restrictions imposed by treatments provided through telemedicine. In this regard, the patient could be advised on how to prepare for follow-up treatment. There are still various unexpected problems and liability issues for remote medical attention. Although oral consent is often acceptable,20 it is recommended to obtain written consent from the patients whenever possible. In the case of using the medical platform, it is recommended to obtain an additional “platform-related agreement.”
4. Determination of target disease, method, and scope for telemedicine
It is necessary to identify the characteristics of the hospitals in which telemedicine is to be conducted and define which diseases will be targeted (DM, hypertension, asthma, etc.), which methods or programs will be used (telephone, online, etc.), and to what extent medical services (repeat medication, medical consultation, etc.) will be provided.13 This means setting strategic goals by considering the hospital's (or doctor's) specialty and financial impact. To achieve this goal, it is good to set a target number of patients to be treated per day using telemedicine. Sufficient consideration is required regarding the duration of each consultation (in fact, phone consultation may take more time than face-to-face treatment), the expected revenue compared with that of face-to-face treatment, and the hospital's capabilities.21
5. Select suitable medical devices and platform
Traditionally, medical devices and platforms are essential for telemedicine for health care.1211 Once physicians have determined the target disease and method for telemedicine, they need to select medical devices and platforms to be used: for example, a glucometer device for people with DM1622 and a blood pressure for people with hypertension.23 If the hospital aims to manage sleep disorders, an appropriate medical device and platform need to be selected.24 It is crucial for physicians to choose a platform (or application) that can record and display the data they upload. Of course, there can be various medical devices of the same type, in which case it is recommended that the medical staff acquire as much experience as possible with medical devices and platforms. Inadequate use of medical devices and platforms may adversely affect patient health management.25 Medical device or platform malfunctions, downtime, slowdowns, etc. may eventually cause the patient to have a negative experience with telemedicine.
6. Organization of medical teams and collaboration with other institutions
Certainly, the number of members in a team will vary depending on the size of the hospital, but it is essential to share roles among members.2627 If there are financial resources, the team could consist of a person in charge of actual health care, a specialist who can help in the management of telemedicine (training users of medical devices or platforms or in charge of continuous updates at the request of users), and an ICT specialist in charge of the medical devices and platforms. The success of telemedicine depends on the appropriate team organization. However, it would be impossible to organize all team members in a local clinic. In the case of a local clinic where it is difficult to organize a team, it is a good idea to reduce the scope of telemedicine or collaborate with a tertiary hospital. In Korea, the “Digital Health Coordinating Center (DHCC)”8162528 would be ideal for this purpose. To ensure the proper use of the medical device and the platform, the patient's ability to access and use these services and technologies may also be considered. This may require ongoing patient education. This role would preferably be played by a tertiary hospital. In this way, the medical staff at the local clinic can focus on providing treatment, while other issues (such as ICT and education) are handled by the tertiary hospital.
7. Guideline and clinical pathway (CP) of telemedicine
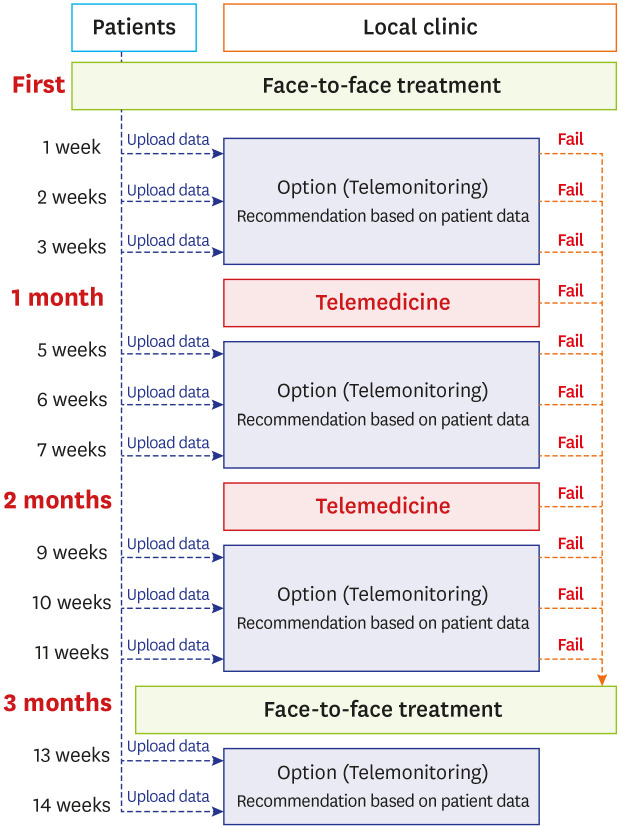
Before starting telemedicine practice, preparing a basic “patient management protocol” is important.2930 In fact, a continuous exchange of information on specific diseases among hospitals is crucial, and it is recommended to use the same “CP” across hospitals (Fig. 1). As mentioned above, the tertiary hospital would be responsible for creating this CP and providing it to the local clinic. The sharing of information on handling methods (i.e., technical know-how) among hospitals that treat patients with the same disease is an important process for improving telemedicine programs. In addition, a large exchange of experiences could allow predicting otherwise unexpected scenarios. Emergency services need to be regularly considered, and a protocol for this needs to be prepared as well.
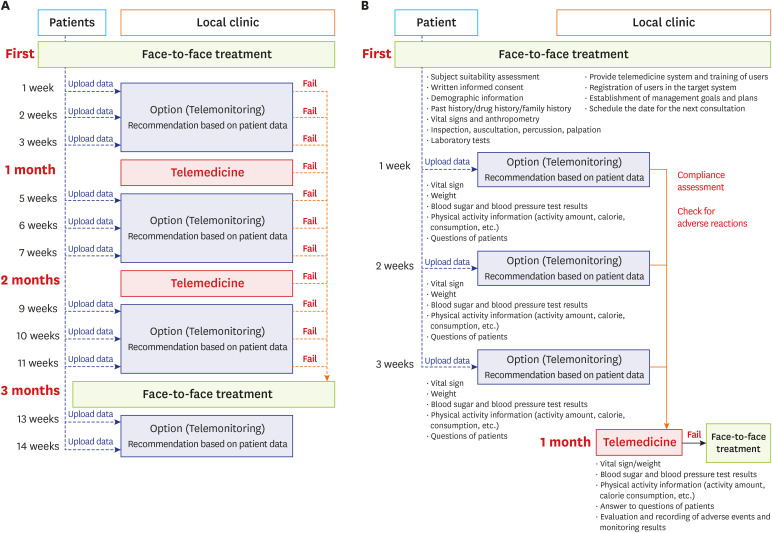 | Fig. 1Examples of critical pathways for telemedicine operation. It is possible to change the target disease at the judgment of the researcher. (A) Long-term plan example. To initiate telemedicine, the patient must first visit the hospital. It is also advisable to schedule regular hospital visits depending on the type of disease (e.g., every 3 months). During periods of non-hospital visits, telemedicine checks the patients condition. (e.g., every month). Telemonitoring checks the patient's condition, and if the condition is unstable, stop telemonitoring at any time and switch to face-to-face treatment. Data uploaded by patients can be evaluated and analyzed weekly according to the patient's condition, not monthly. In all these cases, face-to-face treatment should not be stopped entirely. (B) First month's detailed example. When a patient visits the hospital for the first time, medical staff should perform various tests to see if it is suitable for telemonitoring. After that, the data posted by the patient every week are checked. In this case, there are various details such as vital signs or weight.
|
8. Conduct telemedicine and face-to-face treatment the same way
The basic treatment principle for treating patients with telemedicine is to first follow the treatment guidelines used in face-to-face care. The drugs prescribed in telemedicine are also not different from those prescribed in face-to-face treatment. In both telemedicine and face-to-face consultations, treatments and medications could be prescribed according to the same guidelines. However, it is crucial to pay special attention to the prescription of new drugs, rather than to previous prescriptions, in remote treatment. Preferably, physicians would refrain from prescribing drugs with strong side effects and give detailed explanations to the patient. A face-to-face consultation is recommended for the prescription of treatments and drugs that may cause substance abuse, such as opioids, sleeping pills, antibiotics, and steroids.3132 Of course, there can be exceptions in emergencies, such as in cases of COVID-19. Exceptions can also be made in emergencies that require the careful judgment of the medical staff. If telemedicine is not suitable or if the practice of telemedicine is deemed difficult to maintain, visiting the hospital can be an option. Documenting and recording all this process is crucial.
9. Look beyond the visit: continuity of care
Telemedicine is better for continuous management than for temporary treatment (in fact, this is the key point of continuity of care for telemedicine).3334 In patients using telemedicine for the first time, continuous follow-up care is recommended. We also recommend establishing long-term plans for telemedicine, especially in uncertain situations, such as during the COVID-19 pandemic, whose end is not yet in sight. It is suggested that long-term follow-up care be allowed in telemedicine based on long-term lifestyle management rather than on a single treatment.
10. Improve patient's confidence in the system
Medical professionals need an early approach to increase patient confidence in telemedicine.2 For this reason, it is advisable to prepare a satisfaction survey for patients in the early stages of telemedicine practice.2526 In this relation, it is desirable to also include a questionnaire on the management of the medical team. Moreover, the medical team could focus more on negative feedback than on positive feedback from the patient. In addition to the survey results, doctors could constantly monitor the physical surroundings of the telemedicine room. Continuous communication between medical staff and management staff is of utmost importance. Active promotion of telemedicine, formation of social consensus, and telemedicine business models are also an important part.35 This would be handled as the main axis in the DHCC.
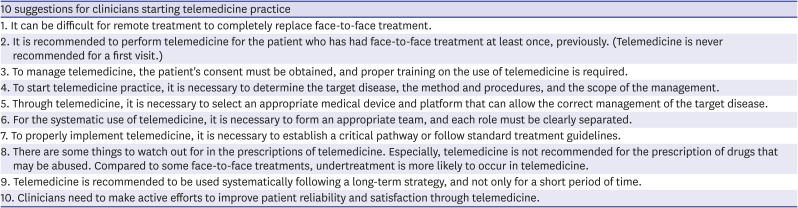
Table 2
Ten suggestions to consider before starting telemedicine
![]()
Go to :
DIGITAL HEALTH COORDINATING CENTER
The 10 suggestions mentioned above are essential rather than optional. In reality, it seems almost impossible to abide by all these 10 suggestions at a local clinic. However, at this point, telemedicine mainly proved and targets chronic diseases, such as diabetes and hypertension, or elderly diseases such as Parkinson disease, dementia, or sleep disorder.111336 Moreover, it would be much better that the management of these diseases be centered on local clinics rather than tertiary hospitals. Therefore, the above 10 recommendations are most necessary to start telemedicine practice in a local clinic with the support of a tertiary hospital (the DHCC in this case).8162528 All types of treatment involved in patient telemedicine are operated by the local clinic, but all the know-how and methods necessary for the telemedicine process, making of CP, and monitoring are managed by the DHCC. This is the reason for recommending the separation of treatments carried out at local clinics and the management of other aspects carried out at the DHCC. This would reduce the cost, labor, and time needed for the management of telemedicine at the local clinic and is a way to strengthen the expertise of the DHCC. The role of tertiary-care hospitals for DHCC will vary, including monitoring the patients' data, sending the patients' summary to the local clinic, training and technical support of local clinics, and supervision of management.5
Go to :
CONCLUSIONS
In the near future, telemedicine will be settled as a part of the medical field. However, the medical staff is not necessarily qualified to handle the process of telemedicine.37 During the COVID-19 outbreak, clinicians accustomed to evidence-based patient management will need to consider in advance how to respond wisely to the social issue of telemedicine.
The possibility, clinical effectiveness, and cost-benefit of telemedicine have already been established through various studies.113 As a next step, medical staff could focus on how to successfully settle telemedicine in the medical field. Although the scientific basis for telemedicine has already been proven, whether its use can be successfully extended in the medical market is a different matter. In practice, telemedicine is likely to be used mainly by some patients who simply do not want to visit the hospital, regardless of other factors (only for repetitive medications). Various side effects and problems can occur. Even if the medical professionals follow appropriate telemedicine recommendations, their “ethical responsibility” remains unchanged. In this regard, various unexpected levels of responsibility can be involved in telemedicine. For this reason, the exchange of information among clinicians and researchers is critical to prevent repeating the same mistakes.
The importance of telemedicine in Korea is indeed relatively lower than in other countries, as Korean patients have good medical access. However, in Korea, many studies have already been conducted on patient management through a combination of ICT and medical fields. ICT and medicine have developed together, and the use of information technology in medicine is now inevitable. Korea is the country with the highest potential for the commercialization of evidence-based telemedicine. In this field, Korea can easily gain global competitiveness, grow rapidly, and differentiate itself from other countries in the medical field.
Currently, clinicians have to adapt to the changing medical trends. Now is the time for medical staff to rely on proper evidence-based judgment. In addition to securing scientific evidence for telemedicine, continuous efforts for commercialization are required. In telemedicine, attention to evidence-based positive outcomes can help improve the patient’s experience, reduce medical costs, and increase patient satisfaction, which points to the importance of active interest and participation of medical staff.
Go to :
 XML Download
XML Download