

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Current major guidelines recommend dual antiplatelet therapy (DAPT) for 6 months in stable ischemic heart disease and 12 months in acute coronary syndrome (ACS) after drug-eluting stent (DES) implantation.123 Nevertheless, the optimal duration of DAPT is still under debate. Prolonged DAPT beyond 12 months significantly reduces ischemic events, but increases the risk of bleeding and does not reduce mortality compared with aspirin monotherapy in the previous studies.45 There is a growing interest in P2Y12 inhibitor monotherapy to mitigate both ischemic and bleeding risks and several randomized trials demonstrated that P2Y12 inhibitor monotherapy following shorter duration DAPT was comparable to standard DAPT in terms of preventing ischemic events.67 However, patients undergoing complex percutaneous coronary intervention (PCI) or those at clinically high-risk such as myocardial infarction (MI) or diabetes may have benefit from DAPT longer than 12 months.8910 In the Ticagrelor with Aspirin or Alone in High-Risk Patients after Coronary Intervention (TWILIGHT) trial, ticagrelor monotherapy was associated with a lower incidence of clinically relevant bleeding than ticagrelor plus aspirin, with no higher risk of death, MI, or stroke in high-risk patients.11 Yet, prolonged use of ticagrelor is indicated in highly selected population.5 In real world practice, clopidogrel is the most frequently prescribed P2Y12 inhibitor, especially beyond 1 year after PCI.12 Up to the present, evidences are scanty regarding treatment effects of clopidogrel monotherapy, compared with prolonged DAPT, after PCI for high-risk patients. In the present study, we investigated long-term outcomes of high-risk patients receiving clopidogrel monotherapy versus prolonged DAPT after implantation of second-generation DES.
METHODS
Study population
Consecutive patients who underwent PCI with at least one second-generation DES for stable angina or ACS between April 2006 and December 2010 were enrolled.
Of these, patients at high-risk who were alive and did not have MI, repeat revascularization, stroke, or major bleeding at the 12-month follow-up after the index procedure were included. High-risk patients required at least one of adverse clinical factors or one of angiographic characteristics as described in previous studies.111314 Clinical high-risk criteria were an age of at least 65 years, female sex, ACS, established vascular disease, diabetes mellitus on medication, and chronic kidney disease.13 Angiographic high-risk criteria included multivessel coronary artery disease, a total stent length of more than 30 mm, a thrombotic target lesion, a bifurcation lesion treated with two stents, an obstructive left main or proximal left anterior descending (LAD) lesion, chronic total occlusion, in-stent restenosis and a calcified target lesion treated with atherectomy.81115 Patients were excluded if they received vitamin K antagonist or antiplatelet agents other than aspirin or clopidogrel. Second-generation DESs were defined as the Biomatrix (Biosensors Europe, Morges, Switzerland), Endeavor, Endeavor Resolute, Endeavor Sprint (Medtronic, Minneapolis, MN, USA), Nobori (Terumo Corporation, Tokyo, Japan), Promus, Promus Element (Boston Scientific, Natick, MA, USA), Xience, or Xience Prime (Abbott Vascular, Abbott Park, IL, USA), PICO Elite (AMG vascular product S.R.L, Winsen, Germany).
Data collection
Data in regard to clinical outcome and PCI procedure were collected from the prospective PCI registry of Samsung Medical Center. Patients were routinely followed up at 1, 6, and 12 months after the index procedure and every year afterwards. Additional telephone contact or reviewing medical records were done to determine antiplatelet therapy duration and compliance of antiplatelet therapy, if necessary. Mortality data were confirmed by the National Population Registry of the Korea National Statistical Office.
Treatment group
Patients were categorized into two groups according to anti-platelet treatment status at 24 months after index PCI: the clopidogrel group (aspirin discontinued within 24 months) and the prolonged DAPT group (prolonged DAPT more than 24 months). Decisions on the discontinuation of aspirin after 12 month-DAPT following the index PCI were at the attending physicians' discretion. During this study, clopidogrel was the only P2Y12 inhibitor available in Korea.
Outcomes and definitions
The primary outcome was a major adverse cardiac and cerebrovascular event (MACCE), a composite of all-cause death, non-fatal MI, definite or probable stent thrombosis, or stroke over 24 months after landmark analysis (12–36 months after the index PCI). Secondary outcomes were the individual components of the MACCE, target vessel revascularization (TVR), target lesion revascularization (TLR), major bleeding and the composite of MACCE and major bleeding.
Cause of deaths were assumed to be cardiac unless an explicit non-cardiac cause was found. MI was defined as elevated cardiac enzyme (troponin I or MB fraction of creatine kinase) level, greater than the upper normal limit with ischemic symptoms or electrocardiographic changes suggesting myocardial ischemia or, MI that required hospitalization with a chief diagnosis of MI.16 Stent thrombosis was defined as the Academic Research Consortium (ARC) criteria.17 Stroke was defined as neurological deficit requiring hospitalization with clinically relevant lesions on brain imaging. TVR was defined as any repeat PCI in the target vessel, while TLR was defined as repeat PCI in the previous stent or occurring within 5 mm of the stent.18 Major bleeding was defined as Bleeding ARC (BARC) criteria type 3 or 5 bleeding. Minor bleeding was defined as BARC type 2 bleeding.19
Statistical analysis
Categorical variables were expressed as number and percentage and compared using χ2 test. Normally distributed continuous variables were presented as mean and standard deviation and compared using unpaired t-test. Non-normally distributed continuous variables were presented as median and interquartile range (IQR) and compared by Wilcoxon rank sum test. Survival curves were drawn between groups using Kaplan-Meier model, and significant differences were calculated using log-rank tests. The Cox proportional hazard model was used to test whether prolonged DAPT was an independent predictor of clinical outcomes. To reduce treatment-selection bias for DAPT and potential confounding factors, we performed propensity score (PS) matching analysis. PSs were obtained by multiple logistic regression in which the antiplatelet regimen is used as the outcome variable, and the selected covariates as predictors. Co-variates which were used for propensity matching are following: age, sex, diabetes, hypertension, current smoking, chronic kidney disease, dyslipidemia, presentation as ACS on the index procedure, history of previous PCI, history of MI, history of previous stroke, PCI on left main artery or LAD artery, 2 or more target vessels, complex PCI, number of stent used, total stent length, stent diameter, use of statin, beta-blockers, angiotensin converting enzyme inhibitors or angiotensin receptor blockers, and calcium channel blockers. The propensity matching was considered to be adequate when overall balance was achieved, indicated by having a standardized mean difference < 0.2. The clopidogrel group and the DAPT group were matched by 1:1 nearest neighbor algorithm. The matched data set was compared by Cox regression model for clinical outcomes. Subgroup analyses were done to assess the treatment effects of prolonged DAPT on the primary end point, compared with clopidogrel monotherapy. The subgroups were age, ACS, ST-segment elevation MI, diabetes, chronic kidney disease, total stent length 28 mm or longer, 2 or more target vessels, and types of DES.
All P values were two-tailed, and P values < 0.05 were considered significant. All data were analyzed using the SPSS version 25 (IBM, Armonk, NY, USA) and R 3.3.3 (R foundation for Statistical Computing, Vienna, Austria) through SPSS custom dialogue.
Ethics statement
The Samsung Medical Center Institutional Review Board approved this study and waived the requirement for written informed consent for access to an institutional PCI registry (reference number 2013-12-031). The study procedures followed the Declaration of Helsinki and the ethical standards of the responsible committee on human experimentation.
RESULTS
Patient characteristics
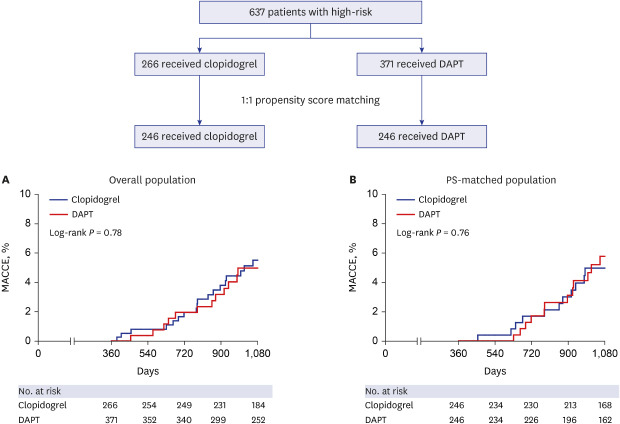
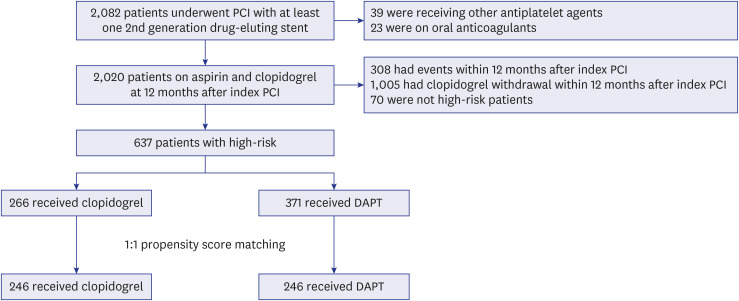
2,082 patients had PCI with at least one second-generation DES during the study period. Of these, 62 were excluded because of receiving vitamin K antagonist or antiplatelet agents other than aspirin or clopidogrel after index PCI. 308 patients with ischemic or bleeding events and 1,005 patients who stopped clopidogrel within 12 months after the index procedure were excluded. Seventy patients who did not meet the criteria for high-risk PCI at the index procedure were excluded. Finally, 637 patients were included in the present study. Patients were divided into the two groups according to antiplatelet regimens: the clopidogrel monotherapy group and the prolonged DAPT group (Fig. 1). Using the PS matching method, we created 246 matched pairs of patients.
Fig. 1
Study design and population.
PCI = percutaneous coronary intervention, DAPT = dual antiplatelet therapy.
Baseline clinical characteristics are presented in Table 1. There was no significant difference in baseline clinical characteristics, except stent type. Zotarolimus eluting stents were more frequently used in the prolonged DAPT group in the overall population. In the PS-matched population, no significant differences were observed in baseline characteristics between the clopidogrel monotherapy group and the prolonged DAPT group. Angiographic and procedural characteristics are presented in Table 2. In the overall population, multivessel PCI was performed more frequently in the clopidogrel monotherapy group compared with the prolonged DAPT group. The number of stents which were used at the index PCI were significantly greater in the clopidogrel monotherapy group. In the PS-matched population, no significant differences were observed in the angiographic or procedural data between the two groups. Median DAPT duration was 14.7 months (IQR, 5.5) in the clopidogrel monotherapy group and 36.0 months (IQR, 7.5) in the prolonged DAPT group (P < 0.0001) (Table 3).
Table 1
Baseline characteristics
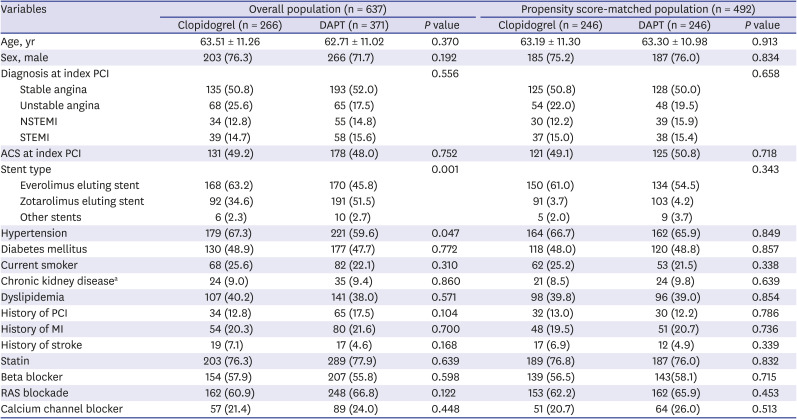
Values are presented as mean ± standard deviation or number of patient (%).
PCI = percutaneous coronary intervention, NSTEMI = non-ST elevation myocardial infarct, STEMI = ST elevation myocardial infarct, ACS = acute coronary syndrome, MI = myocardial infarction, RAS = renin-angiotensin system, DAPT = dual anti-platelet therapy.
aChronic kidney disease was defined if an estimated glomerular filtration rate is below 40 mL/min/1.73 m2 before procedure or a patient was on maintenance dialysis.
Table 2
Angiographic and procedural characteristics

Values are presented as mean ± standard deviation or number of patient (%).
LM = left main, LAD = left anterior descending, PCI = percutaneous coronary intervention, DAPT = dual anti-platelet therapy.
aComplex PCI: chronic total occlusion, bifurcation, thrombotic occlusion, and in stent restenosis PCI.
**P < 0.05.
Table 3
Adherence to antiplatelet regimen in the study population

Long-term outcomes of the overall and PS-matched populations
In the overall population, the risk of MACCE was not significantly different between the clopidogrel monotherapy and prolonged DAPT groups (4.5% versus 4.6%; adjusted hazard ratio [HR], 0.87; 95% confidence interval [CI], 0.40–1.87; P = 0.714) (Fig. 2A and Table 4). In addition, no significant differences were also observed in all-cause death, cardiovascular death, non-fatal MI, stent thrombosis, stroke. There was no significant difference in terms of major bleeding events between the two groups, either (clopidogrel versus DAPT: 1.1% versus 0.3%, P = 0.353), while minor bleeding (BARC type 2) events were reported more frequently in the clopidogrel group (5.6% versus 1.1%; HR, 0.17; 95% CI, 0.05–0.55; P = 0.003) (Table 4).
Fig. 2
Kaplan-Meier survival curves of the (A) overall population and (B) PS-matched population. Analyses starting 12 months after the index percutaneous coronary intervention show event rates of MACCEs.
MACCE = major adverse cardiac and cerebrovascular event, DAPT = dual antiplatelet therapy, PS = propensity score.
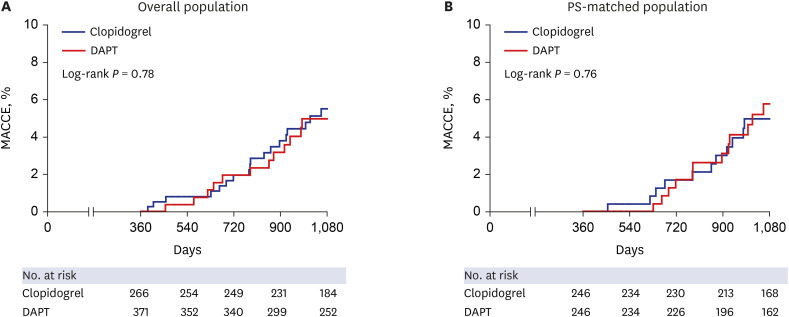
Table 4
Landmark analysis of Cox regression model for survival and risk of clinical outcomes over 3 years after index percutaneous coronary intervention

Values are presented as number of patient (%).
MACCE = major adverse cardiac and cerebrovascular event, MI = myocardial infarction, DAPT = dual anti-platelet therapy, HR = hazard ratio, CI = confidence interval, BARC = Bleeding Academic Research Consortium, TVR = target vessel revascularization, TLR = target lesion revascularization; PCI = percutaneous coronary intervention.
aAdjusted for age, sex, acute coronary syndrome during index admission, hypertension, diabetes, current smoker, chronic kidney disease, dyslipidemia, previous PCI, left main or left anterior descending artery as treated vessel, multi-vessel PCI, complex PCI, total stent numbers, and total stent length; bA composite of all-cause death, non-fatal MI, or stroke.
In the PS-matched population, the risk of MACCE (4.5% versus 4.9%; HR, 1.21; 95% CI, 0.54–2.75; P = 0.643) was not significantly different between the two groups. All-cause mortality, cardiovascular death, non-fatal myocardial infarct, stent thrombosis, stroke, major bleeding, and the composite of MACCE and major bleeding were not significantly different between the two groups, although minor bleeding events were more frequently observed in the clopidogrel group (Fig. 2B and Table 4)
In subgroup analyses, prolonged DAPT did not show significant treatment effect in each subgroup, compared with clopidogrel monotherapy (Supplementary Table 1).
DISCUSSION
In the present study, we investigated the long-term outcomes of patients receiving clopidogrel monotherapy versus prolonged DAPT after PCI. Clopidogrel monotherapy and prolonged DAPT more than 12 months had similar long-term risk of MACCE in patients at high-risk undergoing PCI with second-generation DESs. This result was consistent after PS-matching.
Several studies reported the benefit of prolonged DAPT with regard to reduction of recurrent ischemic events among patients at high-risk such as those undergoing complex PCI or with ACS or diabetes.910152021 However, the risk reduction of ischemic events was not translated into mortality benefit, and an increased risk of bleeding is observed with prolonged DAPT.451021
To overcome this dilemma, P2Y12 inhibitor monotherapy after short duration of DAPT has recently been considered as a new alternative strategy of antiplatelet therapy after PCI with newer generation DES.6711 Several randomized trials demonstrated that P2Y12 inhibitor monotherapy after shorter DAPT had superior outcomes by means of reducing bleeding complication without increasing ischemic events.7 However, the implication of the SMART-CHOICE and STOPDAPT2 trial for high-risk group is limited, as patients with relatively low risk were included in those studies despite enrollment criteria for broad spectrum of patients.67 Although the TWILIGHT trial demonstrated that the high-risk patients treated with ticagrelor monotherapy had less bleeding events than those treated with ticagrelor and aspirin, with similar adverse ischemic events, long-term outcomes of ticagrelor monotherapy beyond 1 years after the index PCI is lacking.11 Above all, potent P2Y12 inhibitors such as ticagrelor and prasugrel are rarely used beyond 1 year after PCI and clopidogrel is the most frequently prescribed P2Y12 inhibitor in real world practice.12 Therefore, we compared the long-term outcomes of clopidogrel monotherapy with prolonged DAPT for high-risk patients after implantation of second-generation DES. Our study adds valuable information on appropriate long-term antiplatelet strategy for high-risk patients after PCI.
In the present study, clopidogrel monotherapy after standard 12-month DAPT, compared with prolonged DAPT longer than 12 months, did not increase ischemic events among high-risk patients. There are several possible explanations for this observation. First, excellent performance of the second-generation DES might lessen the benefit of prolonged DAPT, even among patients at high-risk. The risk of very late stent thrombosis after implantation of the second-generation DES was remarkably low in patients with ACS during long-term follow-up.22 Therefore, clopidogrel monotherapy might suffice even for high-risk patients. Second, patients who had adverse events within 1 year after the index PCI were excluded in our study. Those who did not have ischemic events during first 12 months after PCI might be good responders to clopidogrel therapy and aspirin might have provided little additional inhibition of platelet aggregation for our patients.23 Third, the anti-ischemic efficacy of clopidogrel might be superior to that of aspirin. Clopidogrel monotherapy was associated with reduced risk of recurrent ischemic events with a similar risk of bleeding when compared with aspirin monotherapy beyond 1 year after the index PCI in an observational study.24
Unexpectedly, reduced bleeding risk by clopidogrel monotherapy compared to prolonged DAPT was not demonstrated in the present study. The two groups had similar major bleeding events, while minor bleeding events were more frequently observed in the clopidogrel group. Our study had limited power due to small sample size, and relatively low event rate. The difference of major bleeding event rate between the two groups might have not reached to statistical significance. Also, patients who had ischemic or bleeding events within 12 months after PCI were excluded in our study. Thus, patients with higher bleeding risk might have been excluded and the bleeding risk of prolonged DAPT might have been underestimated in the present study.
This study had several limitations. First, its design was non-randomized observational study, which might have affected the results because of confounding factors. The duration of DAPT was determined by the discretion of attending physicians and it might have affected outcomes. Despite of adjustment using multivariable and PS matching analysis, the possible confounders might not have been completely excluded. Second, with the relatively small sample size, clinical events rate was too low to guarantee our conclusion. Nonetheless, the population of this study was a part of our prospective PCI registry and all events were tracked prospectively. Low event rate in our study is consistent with the excellent long-term outcomes of PCI from other recent studies.425 Third, only clopidogrel was prescribed as a P2Y12 inhibitor for the DAPT regimen, because P2Y12 receptor inhibitors such as ticagrelor or prasugrel were not available in Korea during the study period. However, ticagrelor and prasugrel are indicated only in patients with ACS and are not frequently prescribed beyond 1 year after PCI.
In our observational study, clopidogrel monotherapy and prolonged DAPT have similar long-term risk of MACCE in patients at high-risk undergoing PCI with second-generation DESs. Our data suggest that long-term maintenance clopidogrel monotherapy, rather than prolonged DAPT, can be a promising alternative antiplatelet strategy after PCI for high-risk patients. Further randomized trials should be performed to confirm our suggestion.
 XML Download
XML Download