

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hepatitis B virus (HBV) causes significant human morbidity and mortality worldwide with >240 million people infected.12 Chronic hepatitis B (CHB) is correlated with higher risk of compensated cirrhosis and hepatocellular carcinoma (HCC), with over 20% of patients with CHB progressing to HCC within 10 years.34 Research has shown that the risk of progression to end-stage complications is associated with HBV replication, as assessed with serum HBV DNA levels.5 Thus, suppression of HBV replication with antiviral therapy (AVT) is the primary treatment strategy to prevent poor patient outcomes.26 Oral AVT may prevent disease progression and development of HCC.7 Newer oral AVT agents such as entecavir (ETV) and tenofovir have a high genetic barrier to resistance, making them good candidates for first-line CHB therapy.89 However, the optimal timing for initiating AVT, especially for patients with cirrhosis, is still under debate.10
In 2007, the Korean Association for the Study of the Liver (KASL) published its guideline proposing new initiation criteria for AVT in patients with CHB-related cirrhosis, when both elevated serum HBV DNA (HBV DNA ≥ 2,000 IU/mL) and elevated aspartate aminotransferase (AST) or alanine aminotransferase (ALT) (AST or ALT ≥ 40 IU/L) were identified. Implementation of National Health Insurance Service (NHIS) reimbursement for AVT in these patients started from October 1, 2010. However, it has been argued that liver enzyme levels are not indicative of advanced CHB progression and should not be used as a criterion to determine the initiation of AVT.11 In addition, studies have shown that patients with significant hepatic fibrosis frequently have almost normal AST and ALT levels.1213 Accordingly, this concept has been reflected in various international guidelines for AVT treatment for patients with compensated CHB-related cirrhosis.141516 Therefore, the 2012 KASL clinical practice guidelines have also reflected this concept and recommended initiating AVT for patients with compensated CHB-related cirrhosis with elevated HBV DNA (HBV DNA ≥ 2,000 IU/mL), regardless of AST or ALT levels.12 Medical insurance reimbursement for AVT in those patients was implemented on September 1, 2015. However, no research has shown improved prognosis of earlier AVT initiation for patients with compensated CHB-related cirrhosis.
Therefore, we investigated whether the major change in KASL guidelines, implemented on September 1, 2015, reduced the risk of CHB-related HCC in patients with cirrhosis in South Korea.
METHODS
Treatment-naïve patients with compensated CHB-related cirrhosis who initiated AVT with 0.5 mg/day ETV or 300 mg/day tenofovir disoproxil fumarate (TDF) between July 1, 2014 and August 31, 2015 according to the previous KASL guideline implementation and between September 1, 2015 and October 31, 2016 according to the current KASL guideline implementation from two academic teaching hospitals (Yonsei University Health System [YUHS] and Kyungpook National University Hospital [KNUH]) were considered eligible for study.
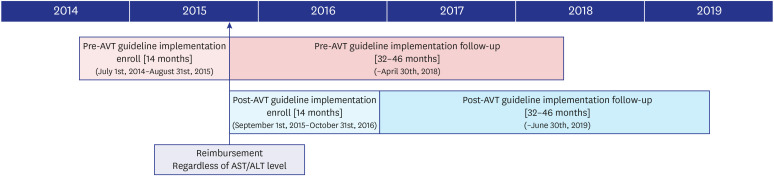
Because the current AVT guideline was implemented through the NHIS reimbursement program on September 1, 2015, the enrollment periods were matched with 14 months before September 1, 2015 as pre-guideline implementation cohort and 14 months after September 1, 2015 as the post-guideline implementation cohort, to ensure a sufficient follow-up period for the post-guideline implementation cohort. Thus, the enrollment period for the pre-guideline implementation and post-guideline implementation cohort was from July 1, 2014 to August 31, 2015 and from September 1, 2015 to October 31, 2016, respectively. Furthermore, to match the follow-up duration between cohorts, the last follow-up date of the pre-guideline implementation cohort and of the post-guideline implementation cohort was April 30, 2018 and June 30, 2019, respectively, resulting in a follow-up duration ranging from 32 to 46 months (Fig. 1). The median follow-up was 36.3 months (interquartile range, IQR 6.9–36.9) and was not significantly different between cohorts (P = 0.882).
Fig. 1
Diagram of cohort enrollment and follow-up period. Patients were enrolled based on AVT start date. The pre- and post-guideline implementation cohort was separated in September 1st, 2015, which is the start date for National Health Insurance Service medical insurance reimbursement for cirrhotic chronic hepatitis B patients with HBV DNA > 2,000 IU/mL, regardless of AST/ALT levels. The enrollment period for the pre-guideline implementation cohort was from July 1st, 2014 to August 31st, 2015 and the post guideline implementation cohort was from September 1st, 2015 to October 31st, 2016 (both 14 months). Follow up periods were matched for both cohorts to a maximum of 45 months, until April 30th, 2018 and June 30th, 2019 for the previous and current AVT guideline cohort, respectively.
AVT = antiviral therapy, AST = aspartate aminotransferase, ALT = alanine aminotransferase, HBV = Hepatitis B virus.
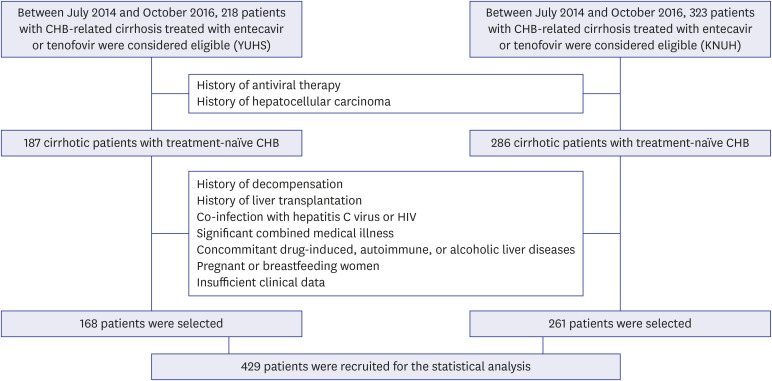
Exclusion criteria included 1) previous AVT; 2) previous HCC; 3) decompensated cirrhosis; 4) previous liver transplantation; 5) co-infection with hepatitis C virus or human immunodeficiency virus (HIV); 6) significant combined medical illness; 7) concomitant drug-induced, autoimmune, or alcoholic liver diseases; 8) pregnant or breastfeeding women; and 9) insufficient clinical information based on prescription records and chart review (Fig. 2). Owing to our homogenous study population, data on race/ethnicity were not collected.
Fig. 2
Flow of study population selection process. A total of 218 patients from YUHS and 323 patients from KNUH with CHB treated with entecavir or tenofovir between July 2014 and October 2016 were considered eligible for participation. After exclusion of 50 and 37 patients from YUHS and KNUH, respectively, according to our exclusion criteria, 168 patients from YUHS and 261 patients from KNUH were ultimately included for statistical analysis.
YUHS = Yonsei University Health System, KNUH = Kyungpook National University Hospital, CHB = chronic hepatitis B, HIV = human immunodeficiency virus.
In the Republic of Korea (ROK), the reimbursement criteria for ETV or TDF were identical during the study period. If histological information was not available, compensated cirrhosis was clinically defined as follows: 1) platelet count < 150,000/μL and ultrasonographic findings suggestive of compensated cirrhosis, including a blunted, nodular liver surface accompanied with splenomegaly (> 12 cm) or 2) esophageal or gastric varices.
Ethics statement
Our study methodology was in accordance with the ethics guidelines of the 1975 Declaration of Helsinki and approved by the Institutional Review Board (IRB) of the two institutes (IRB No. 4-2019-0713). Informed consent was waived due to the retrospective nature of the study.
Clinical follow-up and outcomes
During the follow-up period, all patients had routine blood chemistry testing, HBV DNA level testing, and viral marker testing every 3–6 months. Patients were also screened for HCC according to alpha-fetoprotein level and ultrasonography every six months. If ultrasonographic assessment for HCC identification was not satisfactory, dynamic imaging studies were performed depending on physicians' decision.
The primary clinical outcome was HCC development, which was diagnosed based on histology or dynamic computed tomography and/or magnetic resonance imaging (nodule size > 1 cm) with increased arterial enhancement followed by decreased enhancement compared with the liver (washout) in the portal/delayed phase.17 The second clinical outcome was mortality. The index date was the date of first AVT prescription, and the follow-up period was estimated from the index date until HCC diagnosis, death, or final follow-up.
To increase the stability of our comparison, follow-up cut-off dates were designed to ensure similar follow-up periods for both cohorts. Since the enrollment start dates for the cohorts were independent, follow up dates were matched to better compare the outcome rates of the two cohorts. Furthermore, unequal follow-up periods could lead to additional bias in our study.18
NHIS data analysis
The NHIS database of South Korea is a nationwide health insurance database organized by the government of Korea that records all forms of health-care utilization, including hospitalization, drug prescriptions, and outpatient care for the entire South Korean population. All information regarding health-care utilization is registered by health facilities in a comprehensive database operated by the Health Insurance and Review Agency (HIRA). The HIRA database is a collection of information on patients such as outpatient and inpatient status, drug prescriptions, procedures, demographics, and diagnoses as organized by the International Classification of Diseases 10th revision (ICD-10) codes.
We selected patients who both had a claims data diagnosis of liver cirrhosis (ICD-10: K74 or B18) and received prescription for either ETV or tenofovir between July 2014 and October 2016 while not being on medication for the year prior to prescription. Patients with a diagnosis for cancer of any type, previous AVT, co-infection with hepatitis C virus or HIV, significant combined medical illness, concomitant drug-induced, autoimmune liver diseases in the two years prior to entercavir or tenoforvir prescription, or with a previous liver transplant, were excluded. Outcome was defined as incidence of HCC (ICD-10: C22 and rare incurable disease code). In order to match the follow-up duration between the pre-guideline implementation cohort and the post-guideline implementation cohort, the final follow-up dates were October 31, 2017 and December 31, 2018 respectively, resulting in a follow-up duration of 26 to 40 months.
Statistical analysis
Continuous variables are expressed as median with IQR, whereas categorical variables are expressed as numbers (%). Differences between baseline characteristics were examined using the χ2 test for categorical values and the Student's t-test for continuous variables. Cumulative risk of HCC and mortality was calculated using the Kaplan-Meier method and compared using the log-rank test. Independent risk factors for HCC and mortality were estimated using multivariate Cox proportional hazard regression analysis. Because all patients had compensated liver function at the time of AVT initiation, the variables of Child-Turcotte-Pugh class were not included in the multivariate analysis. Statistical analyses were performed using SPSS software 25.0 for Windows (SPSS Inc., Chicago, IL, USA), and two-tailed P < 0.05 was considered statistically significant.
For analyzing NHIS data, subdistribution hazard ratios were estimated using a Cox subdistribution regression model while accounting for the competing risks of death and liver transplantation. To control for confounding, we adjusted for variables such as age, gender, and history of diabetes mellitus. Analyses were performed using the SAS Enterprise Guide (SAS Institute, Inc., Cary, NC, USA), and P < 0.05 was considered statistically significant.
Propensity score matching (PSM) was used with a 1:1 ratio and adjusted for age, gender, HBV DNA, and hepatitis B virus e antigen (HBeAg). A caliper of 0.2 standard deviations of the logit of the propensity score was used. An absolute standardized mean difference of < 0.1 was considered negligible imbalance.
RESULTS
Baseline characteristics
After excluding 50 and 62 patients from the YUHS and KNUH cohorts, respectively, based on our exclusion criteria, 168 patients from YUHS and 261 from KNUH with compensated CHB-related cirrhosis (247 men and 182 women) were included in the final statistical analysis (Fig. 1).
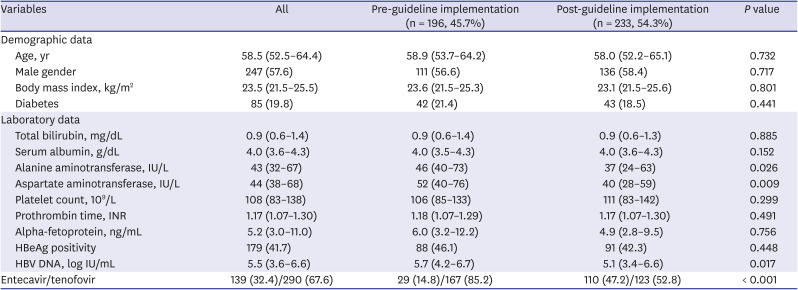
Baseline characteristics of the entire study population are shown in Table 1. Median age of the study population was 58.5 years. Diabetes was identified in 85 (19.8%) patients. The median ALT level was 43 (IQR, 32–67) and HBV DNA was 5.5 log IU/mL (IQR, 3.6–6.6). HBeAg was positive in 179 (41.7%) patients. ETV was initiated in 139 (32.4%) patients, whereas TDF was initiated in 290 (67.6%). Among patients who started AVT after September 2015, 123 patients (52.8%) had normal ALT levels and 114 patients (48.9%) had normal AST levels. Most baseline characteristics were similar between the two institutes (data not shown).
Table 1
Baseline characteristics (n = 429)
Comparison of baseline characteristics according to AVT guideline implementation at treatment initiation
Although most characteristics were statistically similar, patients with AVT initiation before the guideline implementation (n = 196, 45.7%) had significantly higher AST level (median 52 vs. 40 IU/L), ALT level (median 46 vs. 37 IU/L), higher HBV DNA level (median 5.7 vs. 5.1 log IU/mL), and higher proportion of TDF use (85.2% vs. 52.8%) than those with AVT initiation after the guideline implementation (n = 233, 54.3%) (all P < 0.05) (Table 1).
Comparison between patients who developed HCC and those who did not
Patients who developed HCC (n = 48, 11.2%) had a significantly higher age, higher percentage of male gender, lower serum albumin levels, and higher proportion of AVT initiation before the guideline implementation (all P < 0.05) than those who did not develop HCC (n = 381, 88.8%) (data not shown).
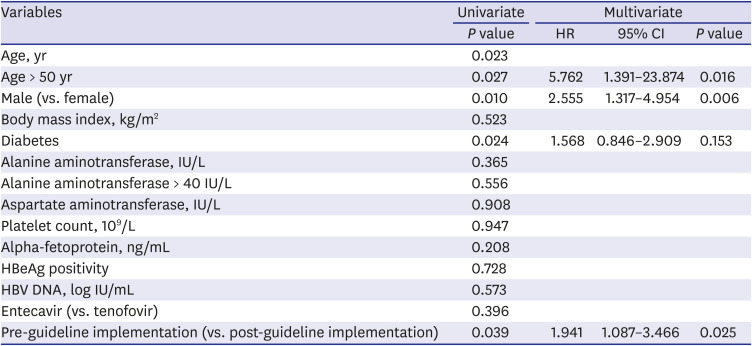
Independent risk factors for HCC development
Univariate analysis showed that age, male gender, and pre-guideline implementation were significant risk factors for HCC development (all P < 0.05). On the subsequent multivariate analysis, together with age greater than 50 years old, higher proportion of male gender, and diabetes, AVT initiation before the guideline implementation was independently associated with a higher risk of HCC development (hazard ratio [HR], 1.941; 95% confidence interval [CI], 1.087–3.466; P = 0.025) (Table 2).
Table 2
Cox regression analysis to identify independent risk factors for HCC
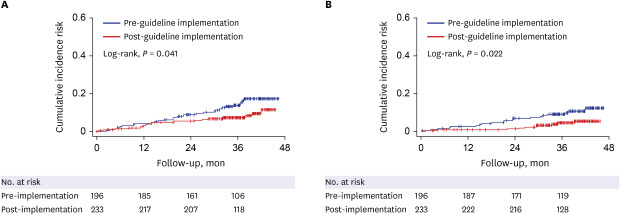
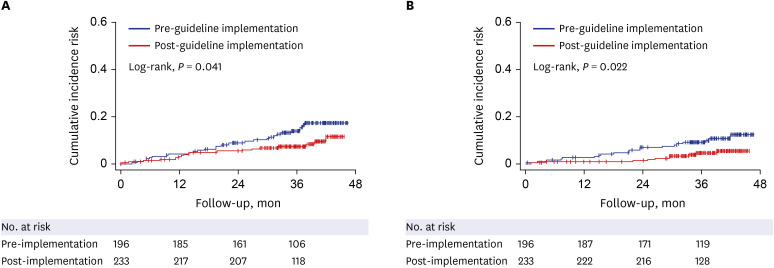
The cumulative incidence rate of HCC in patients with AVT initiation before the guideline implementation was significantly higher than that of patients with AVT initiation after the guideline (P = 0.041, log-rank test) (Fig. 3). The cumulative incidence of HCC for 1, 2, 3 years were 4.1%, 9.3%, and 15.3% for the pre-guideline implementation cohort and 2.6%, 5.4% and 7.9% for the post-guideline implementation cohort, respectively.
Fig. 3
The cumulative incidence rates of HCC (A) and mortality or transplantation (B) according to antiviral therapy guideline implementation. The cumulative incidence risk of HCC and mortality or transplantation of patients in the pre-guideline implementation cohort was significantly higher than that of patients in the post-guideline implementation cohort (P = 0.041 and P = 0.022 respectively, log-rank test).
HCC = hepatocellular carcinoma.
Comparison between patients with or without mortality and liver transplant
Patients with mortality (n = 25, 5.8%) had significantly lower serum albumin levels and lower platelet count (all P < 0.05) than those who survived (n = 404, 94.2%). In addition, patients with liver transplant (n = 5, 1.2%) had significantly lower serum albumin levels and longer prothrombin time, INR (all P < 0.05) than those without liver transplant (n = 424, 98.8%) (data not shown).
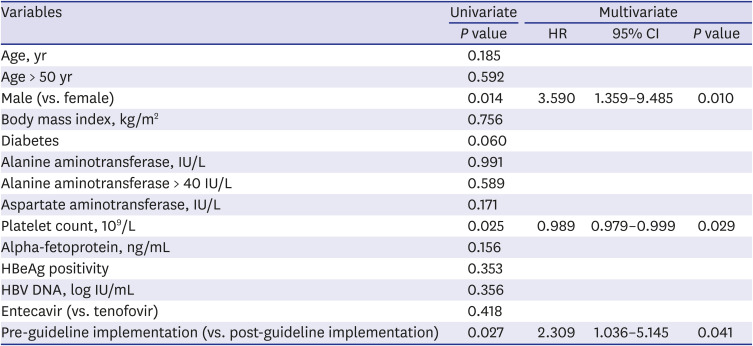
Independent risk factors for mortality or liver transplant
Univariate analysis indicated male gender, platelet count, prothrombin time and pre-guideline implementation as significant risk factors for mortality or liver transplant (all P < 0.05). On the subsequent multivariate analysis, together with higher percentage of male gender and platelet count, pre-guideline implementation was independently associated with higher risk of mortality or liver transplant (HR, 2.400; 95% CI, 1.030–5.591; P = 0.043) (Table 3).
Table 3
Cox regression analysis to identify independent risk factors for mortality or liver transplant
The cumulative incidence rate of mortality or transplantation in patients with AVT initiation before the guideline implementation was significantly higher than that of patients with AVT initiation after the guideline implementation (P = 0.022, log-rank test) (Fig. 3). The cumulative incidence of mortality or liver transplant for 1, 2, 3 years were 2.6%, 6.9%, and 9.7% for the pre-guideline implementation cohort and 0.9%, 1.3% and 4.8% for the post-guideline implementation cohort, respectively.
Subgroup analysis
In a subgroup analysis, 62 patients before the guideline implementation with normal AST and ALT with high HBV DNA not started on AVT and 93 patients after the guideline implementation with normal ALT with high HBV DNA started on AVT were selected. In these two subgroups, there were two and seven cases of HCC, respectively. The cumulative incidence rates of HCC were statistically similar between the two subgroups (P = 0.271 by log-rank test).
NHIS data analysis
Among 48,225 patients with compensated CHB-related cirrhosis, 24,280 were treated before the guideline implementation and 23,975 were treated after the guideline implementation (Supplementary Table 1). Patients treated after the guideline implementation had a significantly higher age (median 48.3 vs. 47.3), lower percentage of male gender (62.8% vs. 63.7%), and lower proportion of TDF use (70.4% vs. 75.2%) than those treated before the guideline implementation (all P < 0.05).
In multivariate analysis, higher age, male gender, and diabetes mellitus were independently associated with a higher risk of HCC development (all P < 0.05), whereas AVT initiation before the guideline implementation showed only a trend of association with increased risk of HCC development (HR, 1.04; 95% CI, 0.96–1.12; P = 0.338) (Supplementary Table 2).
PSM analysis
When age, gender, HBV DNA, and HBeAg positivity were adjusted in the PSM analysis, a total of 344 (172 with pre-guideline implementation vs. 172 with post-guideline implementation) patients were selected for comparison (Supplementary Table 3). In multivariate analysis, AVT initiation before the guideline implementation was independently associated with the increased risk of HCC development, when compared to AVT initiation after the guideline implementation (HR, 2.016; 95% CI, 1.034–3.933; P = 0.040), together with older age (Supplementary Table 4).
Similarly, AVT initiation before the guideline implementation was independently associated with the increased risk of mortality or liver transplant, when compared to AVT initiation after the guideline implementation (HR, 3.411; 95% CI, 1.262–9.388; P = 0.016), together with lower platelet count (Supplementary Table 5).
DISCUSSION
In our study, patients with CHB with AVT initiation before the KASL guideline implementation showed unfavorable outcomes, compared to those treated after the KASL guideline implementation. Specifically, AVT initiation before the guideline implementation was independently associated with an increased risk of HCC development (HR = 1.833), together with older age (HR = 1.041) and male gender (HR = 2.719). In addition, AVT initiation before the guideline implementation independently predicted a higher risk of mortality or liver transplantation (HR = 2.400), together with male gender (HR = 3.056). However, NHIS data analysis showed that patients with AVT initiation before guideline implementation tended to show higher rates of HCC development, mortality, and liver transplantation.
Our study has several clinical implications. It is the first to confirm that the long-term clinical outcomes of CHB-related cirrhotic patients significantly improved after the recent modification of the KASL guideline on AVT treatment and its reimbursement. Despite the retrospective design of our study, our results indicate that appropriate changes in national policy management guidelines may be critical for improvement of treatment outcomes in high risk patients. Although our study focused on the clinical significance of the time point “before and after the revised medical insurance reimbursement for AVT,” we believe that the time point addresses both cohort effects and ALT levels at the beginning of AVT. Since the revised AVT guideline was devised to decrease the barrier to initiation of AVT by removing AST and ALT levels as treatment indications, our data support both the effectiveness of lowering AST and ALT requirements for AVT and the effectiveness of the national policy by showing significant decreases in the risk of HCC and liver transplant or mortality. Several studies have already shown that elevated ALT is not an accurate predictor of disease progression in CHB-related cirrhotic patients, which may explain the clinical significance for lowering AST and ALT requirements for AVT. Lai et al.19 found that 37% of patients with persistently normal ALT had significant fibrosis and inflammation. Similarly, Kumar et al. found that 40.2% of patients with persistently normal ALT levels had a histological fibrosis score ≥ 2.20 These findings support the fact that cirrhotic patients with CHB disease progression may present with normal ALT and that such patients could be overlooked when using older guidelines. Our results suggest that lowering the AVT initiation criteria to include patients with normal ALT and AST levels through public policy could delay disease progression toward clinical endpoints, such as decompensated cirrhosis or HCC, with early intervention.
Second, our results are supported by the relatively large sample size from two tertiary, academic institutes with sufficient laboratory and imaging findings (n > 400). In addition, we validated our results using a large sample derived from the NHIS database; however, the NHIS data only showed a trend for an increased risk of poor outcomes for AVT initiation before the guideline implementation. Despite only showing a trend, we believe that such data may be helpful in recruiting subsequent studies with large hospital samples. Because of the selection of high-risk patients, such as patients with cirrhosis, the proportion of patients who developed HCC was relatively high (> 11%), despite of the relatively short follow-up period. In contrast, in our cohort, we were able to identify well-known risk factors for HCC development, such as age and gender as independent predictors, suggesting a lower risk of statistical errors.
Third, we also performed PSM analysis to adjust the clinical and laboratory characteristics between two cohorts. Similar to the main results from hospital cohorts, AVT initiation before the guideline implementation was independently associated with an increased risk of HCC and mortality or liver transplant after PSM, when compared to AVT initiation after the guideline implementation.
We are also aware of several limitations in our study that remain unresolved. First, our study involved a relatively short follow-up period (median 36.3 months). Due to the NHIS reimbursement date for the current AVT guideline being September 1, 2015, with an enrollment period of 14 months, follow-up of the post-guideline implementation guideline cohort was limited to 45 months, which may be inadequate to ensure development of an appropriate number HCC events for analysis. However, the enrollment of high-risk patients with cirrhosis resulted in sufficient event development, which contributed to overcoming the potential statistical limitation due to a short follow-up period. Second, although analyzed together with mortality to achieve stronger statistical power, the incidence of liver transplantation was rare in our data, which may have led to biased analysis of such events. We believe longer term studies with a sufficient number of various liver-related events may be required. Third, we could not effectively compare patients treated before and after the guideline implementation with high HBV DNA and normal AST and ALT levels due to the relatively small sample sizes in each subgroup (n = 62 vs. 93, respectively) and the small number of HCC cases in each group (n = 2 vs. 7, respectively). Due to these reasons, the cumulative incidence rate of HCC was statistically similar between the two cohorts (P = 0.271), although our results might be susceptible to false negative errors. Fourth, study participants were recruited from tertiary, academic institutes. We believe this might be the reason for higher proportions of patients initiated on ETV after the guideline implementation in 2015, as physicians might be more hesitant to initiate tenofovir in older patients at risk of chronic kidney disease or bone issues in tertiary referral institutes.2122 However, because recent studies have shown that the type of AVT agent does not influence the risk of HCC incidence, the main findings of our study might not have been influenced by the type of antiviral agent.823 Additionally, although our study results may not be fully applicable in the primary care setting, the care and follow up of patients with cirrhosis is usually done at tertiary institutes, thus enhancing the clinical significance of our study. Finally, although the NHIS patient data only revealed a trend of an increased risk for poor patient outcomes pre-guideline implementation, the lack of detailed clinical and laboratory information, such as fibrotic burden and liver function, may be pose potential bias.
In conclusion, the prognosis of patients with CHB-related cirrhosis who underwent AVT improved after implementation of the revised KASL guideline.
 XML Download
XML Download