

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Head and neck cancer (HNC) including cancers of the oral cavity, oropharynx, pharynx, and larynx occurs frequently with over 500,000 new cases diagnosed each year worldwide.1 HNC has a high mortality rate with a five-year survival rates of 50% for tongue, oral cavity and oropharynx cancers.2 The cause of HNC is still unclear; but well-known risk factors are smoking and alcohol abuse,3 and other risk factors are genetic,4 malnutrition,5 radiation,6 poor oral hygiene,7 low socioeconomic status,8 systemic diseases9 such as diabetes, cardiovascular diseases, and viral infections such as human papilloma virus (HPV),10 cytomegalovirus and Epstein-Barr virus.11 Although reports suggested that smoking rate is declining, the morbidity and mortality of HNC squamous cell carcinoma still remain high.12 Although early diagnosis of HNC might improve the prognosis of HNC, still no discrete diagnostic tool is available for detecting HNC at an early stage. Since persistent inflammation and chronic infections could be risk factors of HNC,13 periodontal inflammation could be a risk factor of HNC.
Periodontitis is a chronic inflammation caused by the breakdown of balance between the systemic immunity and the local inflammation in the periodontal tissue.14 This leads to the gradual destruction of periodontium such as gingival, periodontal ligament and alveolar bone that support the teeth. When periodontitis is left untreated, it aggravates pathological changes in periodontal tissue over time which leads to tooth loss ultimately and systemic burden of inflammation which leads to chronic systemic diseases such as atherosclerotic cardiovascular diseases.
The association between cancer and inflammation was first proposed in the 19th century. Lymphoreticular infiltrate found in the sites of chronic inflammation is suggested to be critical in the progression of cancer.15 Periodontitis, a leading infection in the oral cavity, is plausible to increase the risk of developing HNC.16 Progression of cancer is also related to alveolar bone loss (ABL)17 which is a hallmark of periodontitis. Although HNC was associated with chronic periodontitis,18 the association between HNC and periodontitis had a wide range (odds ratio [OR], 1.10–10.9) according to different study designs and target population.
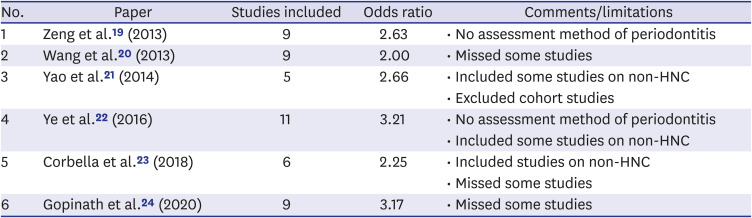
Hitherto, six meta-analyses on the association of periodontal health with oral cancer (OC) or HNC have been published. In 2013, Zeng et al.19 reported the results of meta-analysis using nine articles from 2005 to 2010 with a significant association (OR, 2.63) of periodontal disease with HNC risk, however, it did not evaluate publication bias. In the same year of 2013, Wang et al.20 reported the results of meta-analysis using nine articles for tooth loss and HNC (OR, 2.00). In 2014, Yao et al.21 reported the results of meta-analysis using five articles from 2005–2010 concluding that periodontal disease is an independent risk factor for OC (OR, 2.66). In 2016, Ye et al.22 reported the results of meta-analysis using 11 articles indicating significant correlation between periodontal risk and OC risk (OR, 3.21). Additionally, in 2018, Corbella et al.23 reported a meta-analysis using six articles associating periodontitis encompassing other cancers including esophagus/oropharyngeal cancer pooled together (OR, 2.25). Recently, in 2020, Gopinath et al.24 reported a meta-analysis using nine studies showing significant association between periodontal diseases as a risk factor for HNC (OR, 3.17). Given that the six previous meta-analyses had estimated the association using studies published until that time with some limitations (Table 1), the most recent meta-analysis of Gopinath et al.24 in 2020 had also a lot of limitations. Although they used only nine studies focusing on periodontitis with valid instrument for HNC, they did not consider the quality of study and dropped two studies with valid instrument of periodontal disease: one study7 evaluating tooth loss by oral examination and another study25 evaluating periodontitis by ABL. Hence, more extensive literature search was indispensable to elucidate the association between oral health status related to periodontitis (OHS-P) and HNC after the adjustment of smoking and alcohol drinking and the quality of study. Thus, there is a need for an extensive meta-analysis to clarify the association between OHS-P and HNC after the adjustment of smoking and alcohol drinking.
Table 1
Published meta-analysis papers on the association of periodontal disease with HNC
| No. | Paper | Studies included | Odds ratio | Comments/limitations |
|---|---|---|---|---|
| 1 | Zeng et al.19 (2013) | 9 | 2.63 | • No assessment method of periodontitis |
| 2 | Wang et al.20 (2013) | 9 | 2.00 | • Missed some studies |
| 3 | Yao et al.21 (2014) | 5 | 2.66 | • Included some studies on non-HNC |
| • Excluded cohort studies | ||||
| 4 | Ye et al.22 (2016) | 11 | 3.21 | • No assessment method of periodontitis |
| • Included some studies on non-HNC | ||||
| 5 | Corbella et al.23 (2018) | 6 | 2.25 | • Included studies on non-HNC |
| • Missed some studies | ||||
| 6 | Gopinath et al.24 (2020) | 9 | 3.17 | • Missed some studies |
In this study, we selected 20 original articles published from 1990 until 2020 thoroughly and performed a meta-analysis to estimate the association between periodontitis and the risk of HNC. Our meta-analysis was based on 22 published studies for evaluating the association between OHS-P and HNC. Moreover, we evaluated the publication bias using Egger's regression test and performed subgroup analyses by types of HNC, continents, oral health status and confounders.
METHODS
According to the Preferred Reporting Items for Systematic Reviews and Meta Analyses (PRISMA) guidelines, we searched two major databases, PubMed and Cochrane Database. We selected the published articles to seek the association between OHS-P and HNC from 1990 to 2020 by using two major keywords HNC and OHS-P. The detail keywords were as follows: 1) “oral cancer” or “oral cavity cancer” or “head and neck cancer” or “carcinoma” and 2) “oral health” or “periodontal disease” or “periodontitis.” HNC is a cancer in pharynx, larynx, paranasal sinuses and nasal cavity, and salivary glands. OC is a part of HNC and is a collective term of oral cavity cancer that includes the lips, front two-thirds of the tongue, gums, inner cheeks and lips, floor of the mouth, hard palate and retro-molar triangle.
Based on the search using the aforementioned keywords, 795 articles were identified. According to the inclusion criteria, 22 articles were appropriate for the meta-analysis according to the PRISMA guideline. The inclusion criteria were as follows: 1) the articles as original studies including cohort studies, case-control studies, and cross-sectional studies, 2) the articles with freely available full-text without restriction on publication year; the literature without full text, letters to the editor, case-reports, consortium studies and experimental studies were not included, 3) the articles with the studies adjusted for alcohol drinking and smoking as confounders, 4) Information about association such as OR, relative risk (RR), hazard ratio (HR) and 95% confidence interval (CI) and 5) the definitive criteria for OHS-P including periodontitis, periodontal diseases and oral health status. For meta-analysis, 22 studies from 20 articles were included.
We have collected the information of characteristics from each included study. The characteristics of the studies were considered as follows: 1) study design encompassing cohort studies and a case control studies, 2) country where the study was conducted, 3) sample size of cancer cases and normal controls, 4) oral health status and periodontitis assessment method, 5) adjustments for covariates, 6) tumor site, 7) association (OR, HR, RR and 95% CI), and 8) limitations of each study.
To estimate the association from the included studies, OR was used as the main measurement. Since HR and RR were a bit smaller than OR, HR of two cohort studies by Michaud et al.26 and Nwizu et al.27 were transformed into OR using the formula presented on the previous study28: OR = HR × (1−Pcasesınon-exposure)/(1−Pcasesıexposure). The standard error of the resulting OR was determined from 95% CI by using the formula that was previously presented.29
The risk of bias assessment using the Newcastle-Ottawa Scale (NOS, Case Control Studies) was applied to evaluate the quality of nonrandomized studies in meta-analyses.30 Three factors were considered to score the quality of included studies: 1) selection: case definition, case representativeness, community controls, definition of controls; 2) comparability: adjusted for age, other factors; and 3) exposure: exposure ascertainment, same methods of exposure for cases and controls, non-response rate. We rated the quality of the studies (good, fair and poor) by awarding stars in each domain following the guidelines of the Newcastle–Ottawa Scale. A “good” quality score required 3 or 4 stars in selection, 1 or 2 stars in comparability, and 2 or 3 stars in exposures. A “fair” quality score required 2 stars in selection, 1 or 2 stars in comparability, and 2 or 3 stars in outcomes. A “poor” quality score reflected 0 or 1 star(s) in selection, or 0 stars in comparability, or 0 or 1 star(s) in outcomes.
Computation of pooled ORs with 95% CI and heterogeneity of studies were evaluated using the formula of inverse variance method31 installed in Revman manager software (Revman, version 5.4.1 Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). Heterogeneity is the value that refers to the variation between studies. I2 refers to the percent of variation among studies due to the heterogeneity rather than chance. The I2 value of 25%, 50%, 100% indicates low, moderate and high heterogeneity, when P value for I2 is less than 0.05.32 In general, the fixed model is applied in case that I2 value is less than 25% or P value for I2 is more than 0.05. The random model is applied, when I2 value is more than 25% and P value for I2 is less than 0.05. A forest plot was applied to show the results of meta-analysis including ORs and 95% CIs of all studies included in the analysis.
To test for publication bias, funnel plot and Egger's regression test were applied using Comprehensive Meta-Analysis software version 3 (CMA, Biostat Inc., Englewood, NJ, USA). A funnel plot was applied to visualize the distribution of dots (studies). If the distribution of dots is symmetrical, there is no publication bias amongst studies; otherwise, it has publication bias. Egger's regression test evaluates the evidence of publication bias in the meta-analysis. When the P value of Egger's regression test is less than 0.05, there is publication bias.
These previous studies had different assessment method for evaluating OHS-P, which resulted in different associations. To minimize the difference on the association of OHS-P, the first line of choice was the assessment method of periodontitis (ABL, clinical attachment loss [CAL]), and then tooth loss and oral hygiene. For evaluating OR, OHS-P was dichotomized as good and bad according to the classification of studies. Moreover, the association was different across the characteristics of the studies. Hence, we performed subgroup analyses according to the following variables: 1) study design, 2) assessment method of periodontitis, 3) the quality of study: risk of bias assessment, 4) tumor site, and 5) the global region.
RESULTS
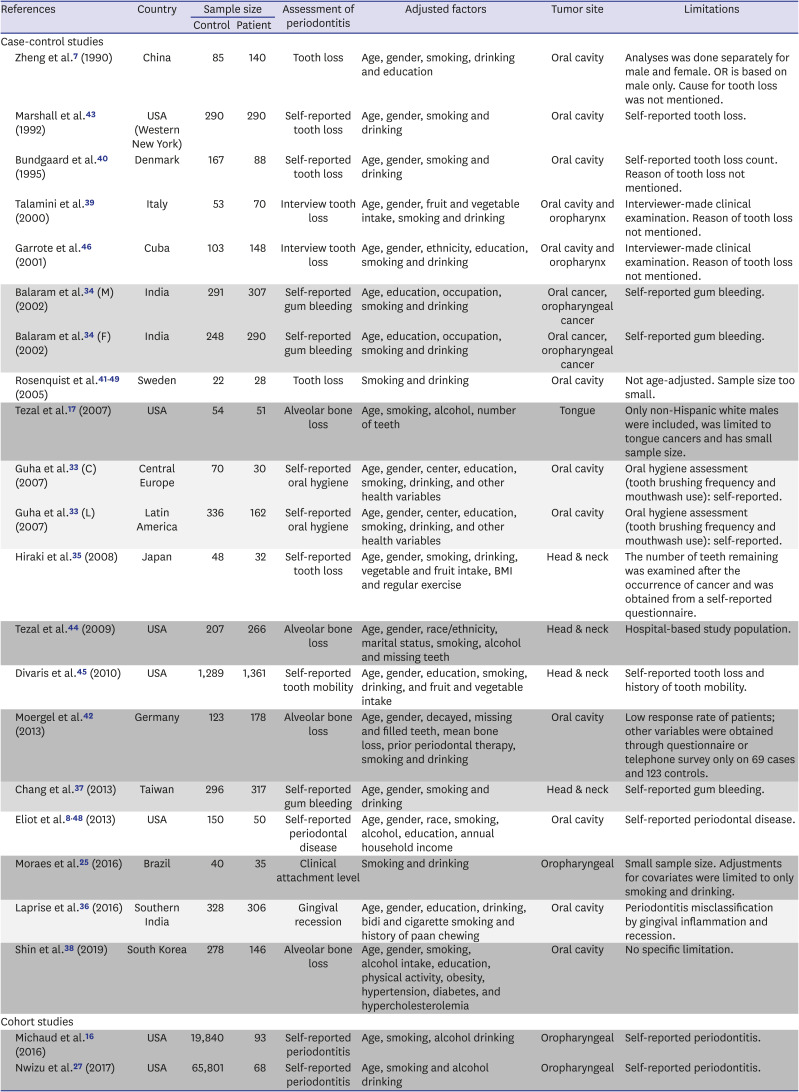
From the initial search of 795 articles, 22 articles satisfied the eligibility criteria for meta-analysis based on PRISMA guideline (Fig. 1). Out of the 22 articles, we selected 20 articles, because 1) Tezal's article of 2005 was part of 2007 and the article of 200717 was selected only and 2) Michaud's articles 2008 was part of 2016 and the articles of 201616 was selected only. Moreover, Guha et al.33 conducted multi-country studies in Central Europe and Latin America, and Balaram et al.34 performed study on male and female. These two articles were counted as two separate studies per each article (Table 2). Finally, 22 studies were included for the analysis.
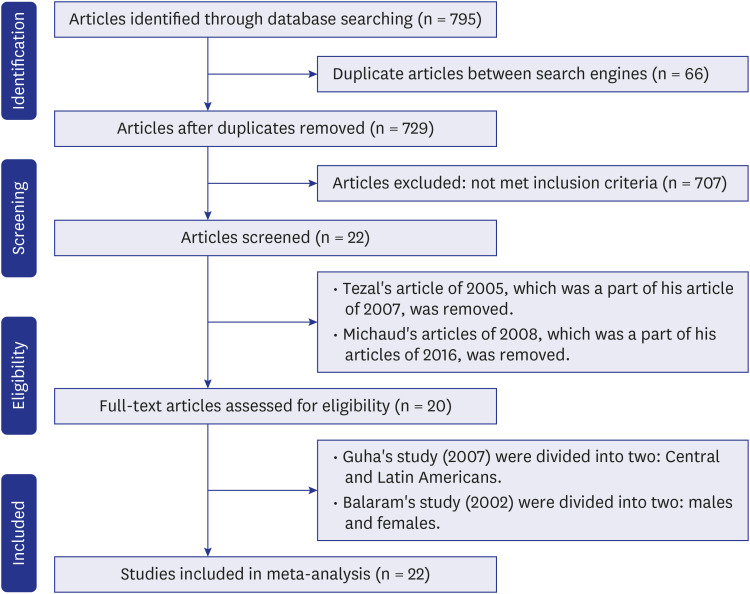
Table 2
Characteristics of studies included
| References | Country | Sample size | Assessment of periodontitis | Adjusted factors | Tumor site | Limitations | ||
|---|---|---|---|---|---|---|---|---|
| Control | Patient | |||||||
| Case-control studies | ||||||||
| Zheng et al.7 (1990) | China | 85 | 140 | Tooth loss | Age, gender, smoking, drinking and education | Oral cavity | Analyses was done separately for male and female. OR is based on male only. Cause for tooth loss was not mentioned. | |
| Marshall et al.43 (1992) | USA (Western New York) | 290 | 290 | Self-reported tooth loss | Age, gender, smoking and drinking | Oral cavity | Self-reported tooth loss. | |
| Bundgaard et al.40 (1995) | Denmark | 167 | 88 | Self-reported tooth loss | Age, gender, smoking and drinking | Oral cavity | Self-reported tooth loss count. Reason of tooth loss not mentioned. | |
| Talamini et al.39 (2000) | Italy | 53 | 70 | Interview tooth loss | Age, gender, fruit and vegetable intake, smoking and drinking | Oral cavity and oropharynx | Interviewer-made clinical examination. Reason of tooth loss not mentioned. | |
| Garrote et al.46 (2001) | Cuba | 103 | 148 | Interview tooth loss | Age, gender, ethnicity, education, smoking and drinking | Oral cavity and oropharynx | Interviewer-made clinical examination. Reason of tooth loss not mentioned. | |
| Balaram et al.34 (M) (2002) | India | 291 | 307 | Self-reported gum bleeding | Age, education, occupation, smoking and drinking | Oral cancer, oropharyngeal cancer | Self-reported gum bleeding. | |
| Balaram et al.34 (F) (2002) | India | 248 | 290 | Self-reported gum bleeding | Age, education, occupation, smoking and drinking | Oral cancer, oropharyngeal cancer | Self-reported gum bleeding. | |
| Rosenquist et al.4149 (2005) | Sweden | 22 | 28 | Tooth loss | Smoking and drinking | Oral cavity | Not age-adjusted. Sample size too small. | |
| Tezal et al.17 (2007) | USA | 54 | 51 | Alveolar bone loss | Age, smoking, alcohol, number of teeth | Tongue | Only non-Hispanic white males were included, was limited to tongue cancers and has small sample size. | |
| Guha et al.33 (C) (2007) | Central Europe | 70 | 30 | Self-reported oral hygiene | Age, gender, center, education, smoking, drinking, and other health variables | Oral cavity | Oral hygiene assessment (tooth brushing frequency and mouthwash use): self-reported. | |
| Guha et al.33 (L) (2007) | Latin America | 336 | 162 | Self-reported oral hygiene | Age, gender, center, education, smoking, drinking, and other health variables | Oral cavity | Oral hygiene assessment (tooth brushing frequency and mouthwash use): self-reported. | |
| Hiraki et al.35 (2008) | Japan | 48 | 32 | Self-reported tooth loss | Age, gender, smoking, drinking, vegetable and fruit intake, BMI and regular exercise | Head & neck | The number of teeth remaining was examined after the occurrence of cancer and was obtained from a self-reported questionnaire. | |
| Tezal et al.44 (2009) | USA | 207 | 266 | Alveolar bone loss | Age, gender, race/ethnicity, marital status, smoking, alcohol and missing teeth | Head & neck | Hospital-based study population. | |
| Divaris et al.45 (2010) | USA | 1,289 | 1,361 | Self-reported tooth mobility | Age, gender, education, smoking, drinking, and fruit and vegetable intake | Head & neck | Self-reported tooth loss and history of tooth mobility. | |
| Moergel et al.42 (2013) | Germany | 123 | 178 | Alveolar bone loss | Age, gender, decayed, missing and filled teeth, mean bone loss, prior periodontal therapy, smoking and drinking | Oral cavity | Low response rate of patients; other variables were obtained through questionnaire or telephone survey only on 69 cases and 123 controls. | |
| Chang et al.37 (2013) | Taiwan | 296 | 317 | Self-reported gum bleeding | Age, gender, smoking and drinking | Head & neck | Self-reported gum bleeding. | |
| Eliot et al.848 (2013) | USA | 150 | 50 | Self-reported periodontal disease | Age, gender, race, smoking, alcohol, education, annual household income | Oral cavity | Self-reported periodontal disease. | |
| Moraes et al.25 (2016) | Brazil | 40 | 35 | Clinical attachment level | Smoking and drinking | Oropharyngeal | Small sample size. Adjustments for covariates were limited to only smoking and drinking. | |
| Laprise et al.36 (2016) | Southern India | 328 | 306 | Gingival recession | Age, gender, education, drinking, bidi and cigarette smoking and history of paan chewing | Oral cavity | Periodontitis misclassification by gingival inflammation and recession. | |
| Shin et al.38 (2019) | South Korea | 278 | 146 | Alveolar bone loss | Age, gender, smoking, alcohol intake, education, physical activity, obesity, hypertension, diabetes, and hypercholesterolemia | Oral cavity | No specific limitation. | |
| Cohort studies | ||||||||
| Michaud et al.16 (2016) | USA | 19,840 | 93 | Self-reported periodontitis | Age, smoking, alcohol drinking | Oropharyngeal | Self-reported periodontitis. | |
| Nwizu et al.27 (2017) | USA | 65,801 | 68 | Self-reported periodontitis | Age, smoking and alcohol drinking | Oropharyngeal | Self-reported periodontitis. | |
Same color band denotes the same study characteristics for assessment of periodontitis. Balaram's study 2002 were divided into two: males (M) and females (F). Guha, 2007 conducted multi-country analyses in Central Europe (C) and Latin America (L). Both studies are counted as separate dataset. Countries of Russia, Romania and Poland are included in Central Europe (C), and countries of Argentina, Cuba and Brazil are included in Latin America (L).
OR = odds ratio, BMI = body mass index.
Out of 22 studies, 20 studies in Asia,73435363738 Europe,3339404142 USA,817434445 and Latin America253346 were case-control studies. The other two studies were cohort studies in USA: Michaud et al.16 and Nwizu et al.27. Nineteen studies showed significant association of periodontal disease with HNC, while three studies263438 reported non-significant association of periodontal disease with HNC. Five studies evaluated ABL, while other 17 studies did not evaluate periodontal disease by ABL but by tooth loss, oral hygiene, self-report, tooth mobility and gingival inflammation (Table 2). Tezal evaluated ABL for periodontitis among Americans and reported significant association with tongue cancer17 (OR, 5.23; 95% CI, 2.64–10.36) and HNC43 (OR, 4.36; 95% CI, 3.16–6.02). In 2013, Moergel et al.42 evaluated ABL among 301 Germans and reported significant association (OR, 2.40; 95% CI, 1.52–3.80) between periodontitis and oral cavity cancer. In 2016, Morase et al.25 evaluated ABL by using CAL among 75 Brazilians and reported significant association (OR, 10.90; 95% CI, 1.90–62.53) between periodontitis and oropharyngeal cancer. A recently published article by Shin et al.38 in 2019 evaluated ABL among 424 Koreans and reported significant association with oral cavity cancer (OR, 3.66; 95% CI, 1.46–9.23).
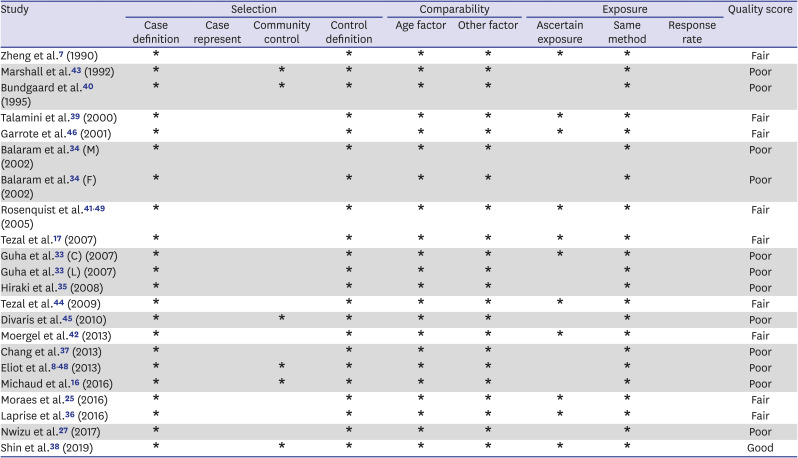
According to the risk of bias assessment using the NOS (Case Control Studies), the most recent one study38 showed good quality and 9 studies were fair, while the other 12 studies were classified as poor (Table 3).
Table 3
Risk of bias assessment (Newcastle-Ottawa Quality Assessment Scale criteria)
| Study | Selection | Comparability | Exposure | Quality score | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Case definition | Case represent | Community control | Control definition | Age factor | Other factor | Ascertain exposure | Same method | Response rate | ||
| Zheng et al.7 (1990) | * | * | * | * | * | * | Fair | |||
| Marshall et al.43 (1992) | * | * | * | * | * | * | Poor | |||
| Bundgaard et al.40 (1995) | * | * | * | * | * | * | Poor | |||
| Talamini et al.39 (2000) | * | * | * | * | * | * | Fair | |||
| Garrote et al.46 (2001) | * | * | * | * | * | * | Fair | |||
| Balaram et al.34 (M) (2002) | * | * | * | * | * | Poor | ||||
| Balaram et al.34 (F) (2002) | * | * | * | * | * | Poor | ||||
| Rosenquist et al.4149 (2005) | * | * | * | * | * | * | Fair | |||
| Tezal et al.17 (2007) | * | * | * | * | * | * | Fair | |||
| Guha et al.33 (C) (2007) | * | * | * | * | * | * | Poor | |||
| Guha et al.33 (L) (2007) | * | * | * | * | * | Poor | ||||
| Hiraki et al.35 (2008) | * | * | * | * | * | Poor | ||||
| Tezal et al.44 (2009) | * | * | * | * | * | * | Fair | |||
| Divaris et al.45 (2010) | * | * | * | * | * | * | Poor | |||
| Moergel et al.42 (2013) | * | * | * | * | * | * | Fair | |||
| Chang et al.37 (2013) | * | * | * | * | * | Poor | ||||
| Eliot et al.848 (2013) | * | * | * | * | * | * | Poor | |||
| Michaud et al.16 (2016) | * | * | * | * | * | * | Poor | |||
| Moraes et al.25 (2016) | * | * | * | * | * | * | Fair | |||
| Laprise et al.36 (2016) | * | * | * | * | * | * | Fair | |||
| Nwizu et al.27 (2017) | * | * | * | * | * | Poor | ||||
| Shin et al.38 (2019) | * | * | * | * | * | * | * | Good | ||
Shaded band denotes the quality of study.
Good quality: 3 or 4 stars (*) in selection domain AND 1 or 2 stars in comparability domain AND 2 or 3 stars in outcome domain; Fair quality: 2 stars in selection domain AND 1 or 2 stars in comparability domain AND 2 or 3 stars in outcome/exposure domain; Poor quality: 0 or 1 star in selection domain OR 0 stars in comparability domain OR 0 or 1 stars in exposure domain.
Balaram's study 2002 were divided into two: males (M) and females (F). Guha, 2007 conducted multi-country analyses in Central Europe (C) and Latin America (L). Both studies are counted as separate dataset. Countries of Russia, Romania and Poland are included in Central Europe (C), and countries of Argentina, Cuba and Brazil are included in Latin America (L).
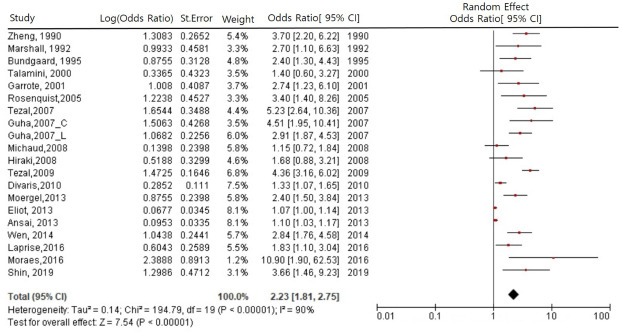
Since heterogeneity of I2 among 22 studies was 88%, which was statistically significant (P < 0.001), we selected the estimate of random effect. For evaluating overall estimates, 22 studies were pooled for random effect. The association of OHS-P with the risk of HNC was significant (OR, 2.42; 95% CI, 1.88–3.13) for random effect model (Fig. 2A). Our results indicate that those with bad OHS-P, compared to those with good OHS-P, were more likely to have the risk of HNC by 2.4 times. The funnel plot, representing each study by dots, showed that the distribution of 22 studies was asymmetrical and suggested publication bias (Fig. 3A). Moreover, the results of Egger's regression test also showed publication bias (Egger's bias = 3.15, P < 0.001). Thus, the significant association of the meta-analysis using 22 studies included publication bias.
Fig. 2
Forest plot of the association of oral health status related to periodontitis with head and neck cancer. (A) Studies pooled with random effect using 22 studies. (B) Studies pooled with fixed effect in 5 studies using alveolar bone loss including clinical attachment loss for periodontitis assessment. Guha (2007) reported multicentric analyses in Central America (C) and Latin America (L), and we divided the literature into two studies, Guha (C) 2007 and Guha (L) 2007. Balaram (2002) conducted studies in male and female, so we consider in two studies, Balaram (M) 2002 and Balaram (F) 2002.
OHS-P = oral health status related to periodontitis, CI = confidence interval, ABL = alveolar bone loss.
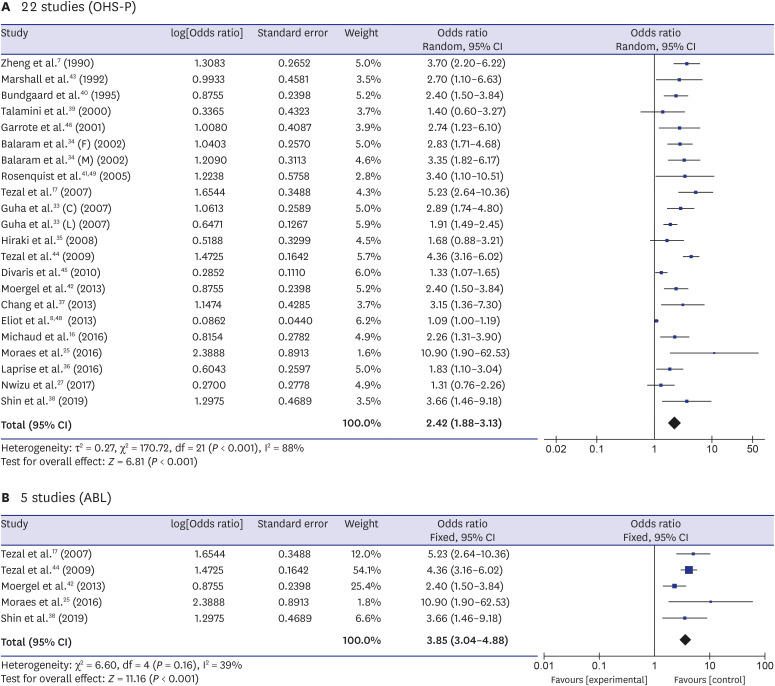
Fig. 3
Funnel plot of studies and Egger's regression for publication bias. (A) 22 studies included in meta-analysis. (B) 5 studies using ABL including clinical attachment loss for periodontitis assessment. A dot represents the result of each study in the funnel plot. When Egger's regression test is significant (P < 0.05), there is a publication bias.
OHS-P = oral health status related to periodontitis, ABL = alveolar bone loss.
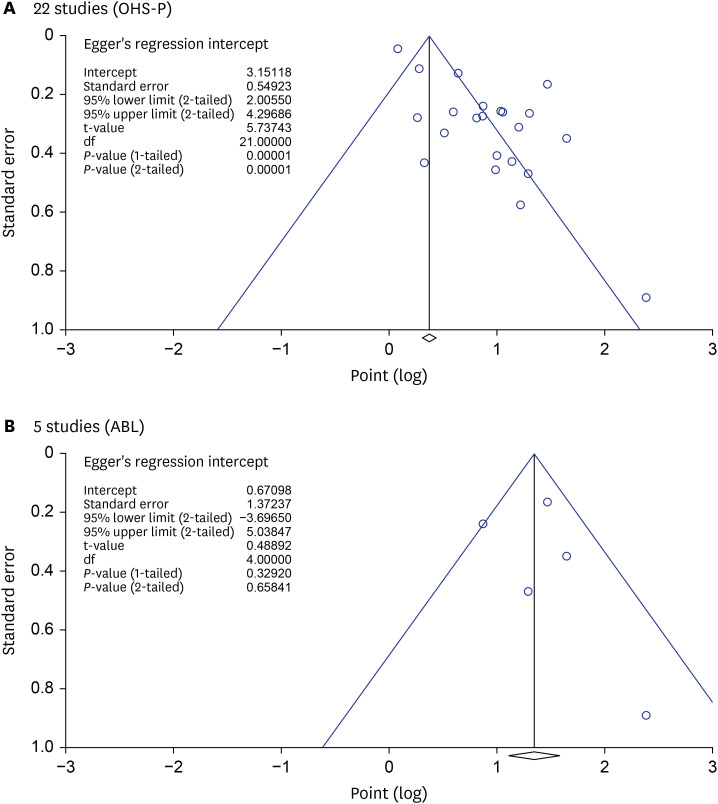
Moreover, five studies using ABL had heterogeneity of I2 = 39%, which was not statistically significant (P = 0.16), we select the estimate of fixed effect. The association of OHS-P with the risk of HNC was increased to OR of 3.85 (95% CI, 3.04–4.88) (Fig. 2B). Additionally, the funnel plot of 5 studies using ABL for periodontitis was symmetrical without publication bias (Egger's bias = 0.67, P = 0.66) (Fig. 3B).
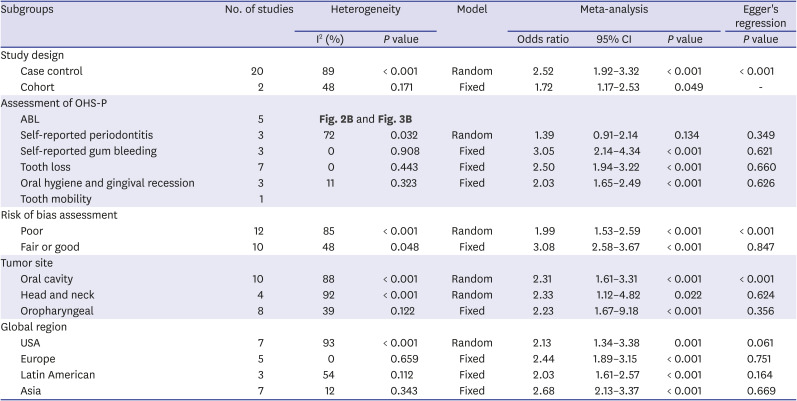
Subgroup meta-analysis according to risk of bias assessment, study design, assessment method of OHS-P and the global region showed that the association was increased dramatically (Table 4). The association was higher and without publication bias in 10 fair or good quality studies (OR, 3.08). Moreover, the association was strongest and without publication bias in seven Asian studies (OR, 2.68), followed by five European studies (OR, 2.44) and seven American studies (OR, 2.13) in order.
Table 4
Association of subgroup analyses
| Subgroups | No. of studies | Heterogeneity | Model | Meta-analysis | Egger's regression | ||||
|---|---|---|---|---|---|---|---|---|---|
| I2 (%) | P value | Odds ratio | 95% CI | P value | P value | ||||
| Study design | |||||||||
| Case control | 20 | 89 | < 0.001 | Random | 2.52 | 1.92–3.32 | < 0.001 | < 0.001 | |
| Cohort | 2 | 48 | 0.171 | Fixed | 1.72 | 1.17–2.53 | 0.049 | - | |
| Assessment of OHS-P | |||||||||
| ABL | 5 | Fig. 2B and Fig. 3B | |||||||
| Self-reported periodontitis | 3 | 72 | 0.032 | Random | 1.39 | 0.91–2.14 | 0.134 | 0.349 | |
| Self-reported gum bleeding | 3 | 0 | 0.908 | Fixed | 3.05 | 2.14–4.34 | < 0.001 | 0.621 | |
| Tooth loss | 7 | 0 | 0.443 | Fixed | 2.50 | 1.94–3.22 | < 0.001 | 0.660 | |
| Oral hygiene and gingival recession | 3 | 11 | 0.323 | Fixed | 2.03 | 1.65–2.49 | < 0.001 | 0.626 | |
| Tooth mobility | 1 | ||||||||
| Risk of bias assessment | |||||||||
| Poor | 12 | 85 | < 0.001 | Random | 1.99 | 1.53–2.59 | < 0.001 | < 0.001 | |
| Fair or good | 10 | 48 | 0.048 | Fixed | 3.08 | 2.58–3.67 | < 0.001 | 0.847 | |
| Tumor site | |||||||||
| Oral cavity | 10 | 88 | < 0.001 | Random | 2.31 | 1.61–3.31 | < 0.001 | < 0.001 | |
| Head and neck | 4 | 92 | < 0.001 | Random | 2.33 | 1.12–4.82 | 0.022 | 0.624 | |
| Oropharyngeal | 8 | 39 | 0.122 | Fixed | 2.23 | 1.67–9.18 | < 0.001 | 0.356 | |
| Global region | |||||||||
| USA | 7 | 93 | < 0.001 | Random | 2.13 | 1.34–3.38 | 0.001 | 0.061 | |
| Europe | 5 | 0 | 0.659 | Fixed | 2.44 | 1.89–3.15 | < 0.001 | 0.751 | |
| Latin American | 3 | 54 | 0.112 | Fixed | 2.03 | 1.61–2.57 | < 0.001 | 0.164 | |
| Asia | 7 | 12 | 0.343 | Fixed | 2.68 | 2.13–3.37 | < 0.001 | 0.669 | |
DISCUSSION
The results of meta-analysis on the association between periodontitis and HNC using 22 studies provide the most current evidence showing that patients with periodontal disease are more likely to have HNC by 2.4 times, which was similar or slightly higher association to Corbella's (OR, 2.3)23 and Wang's (OR, 2.0).20 Our subgroup analysis results using 10 fair or good quality studies (OR, 3.08) showed similar association compared to four previous meta-analyses results such as Gopinath (OR, 3.17),24 Zeng's (OR, 2.6),19 Ye's (OR, 3.2),22 Yao's (OR, 2.7).21
This study has some advantages compared to the previous six meta-analysis studies. Firstly, we included additional published articles, having 20 published articles involving 22 studies in total, while they used only a few articles that published until the analysis time. Secondly, all of studies in meta-analysis were adjusted for smoking and alcohol drinking, which were the most common risk factor for HNC. Thirdly, we performed subgroup analyses according to risk of bias assessment, study design, assessment method of periodontitis, tumor site and global region. Fourthly, we applied the risk of bias assessment using the NOS to evaluate the quality of nonrandomized studies. Finally, we performed Egger's regression test for evaluating publication bias.
Heterogeneity was observed in meta-analysis extensively due to the differences in characteristics of study population, country, study design, assessment of periodontitis, tumor site, and adjustment for covariates. The score of I2 was 88% and random effect was applied for meta-analysis. In subgroup analyses, ethnicity and design of study showed a high heterogeneity. According to the Newcastle-Ottawa Quality Assessment Scale criteria,30 12 studies (54.5%) out of 22 studies showed poor quality, because they used hospital controls and self-reported assessment of exposure. Decrease in heterogeneity indicates the uniform standards in the study design on the relation between HNC and periodontitis. In terms of the standards for study design, we recommend sufficient hospital cases and community cohort controls, which is a requirement of Newcastle-Ottawa Quality Assessment Scale criteria:30 the cancer cases are recruited from the hospitals of cancer surgery and the controls are recruited from the community residents in a health cohort study. Valid assessment of periodontitis should be recommended to apply ABL by panoramic radiograph or CAL by periodontal pocket probing. Adjustment of well-known confounders such as age, sex, smoking and drinking was also recommended to reduce the over-estimation due to the lack of adjustment. For adequate sample size estimation for a main study, a pilot study should be performed to obtain the representative information about OR and 95% CI. The information about OR and 95% CI is indispensable to estimate the sample size.
In spite of modern treatment and technology including surgery, chemotherapy, radiation,7 drug therapy,47 HNC has high mortality and low survival rates. However, early detection of the disease will increase the survival rate dramatically. Unfortunately, early detection and diagnosis of HNC has shown slow improvement compared with other cancers. Studies have reported significant association between poor oral health and HNC.3348 Two studies mentioned that oral squamous cell carcinoma (OSCC) was related to non-steroid anti-inflammatory drug (NSAID). Michaud et al.26 reported that men with fewer teeth were more likely to be taking NSAID. Rosenquist et al.49 reported that NSAID medication was associated with an increased risk of OSCC (OR, 3.5; 95% CI, 1.8–6.7), assuming that cancer patients had self-medication of NSAID due to early symptoms of OC. Therefore, it was not clear that NSAID medication was directly associated with OC. The primary prevention strategy such as improving the oral health status of an individual will decrease the risk of having chronic inflammation and eventually risk of HNC.42 Thus, a new method of prevention and management for both oral health and HNC must be advocated for decreasing the risk of HNC and periodontal disease simultaneously.
In the process of carcinogenesis, involvement of oral bacteria has been suggested.50 Periodontitis is due to the accumulation of bacteria leading to infection such as gram-negative anaerobic bacteria which leads to destruction of the supporting tissue and tooth loss. It has been reported that chronic infection has a direct (toxic effect of microorganisms) and indirect (through inflammation) role in carcinogenesis.17 A study presented six common bacteria significantly higher level in OSCC patients: Prevotella melaninogenica, Capnocytophaga gingivalis, Capnocytophaga ochracea, Eubacterium saburreum, Leptotrichia buccalis and Streptococcus mitis.
50 Various evidence reported that cancers were associated with a specific bacteria such as Helicobacter pylori in gastric carcinoma51 and Streptococcus bovis in intestinal cancer.52 Moreover, Streptococcus anginosus has been frequently seen in oral and esophageal cancer.53 Therefore, further studies are suggested to investigate specific periopathogenic microorganisms in species-level for earlier detection of the risk of HNC.
ABL which does not result in bone gain even after treatment could be a definite marker in the assessment of periodontitis.54 Moreover, CAL, the highly correlated with ABL, is an alternative definite marker for assessment by using periodontal pocket depth, since it is a physiologically irreversible sign of periodontitis.55 Tezal et al.17 suggested the protocol for assessing periodontitis by ABL using panoramic radiographs measuring from the cemento-enamel junction of the tooth to the highest point of the alveolar crest in the mesial and distal sides of tooth. Two thirds of cancer cases were reported to have advanced periodontitis accompanied by probing pocket depth (PPD) of more than 6 mm,56 but PPD cannot justify that patients have periodontitis because PPD can be modified by several factors and it can be reversible after treatment.
Recently, salivary biomarkers have been vastly reported as a diagnostic tool for HNC. Matrix metalloproteinase-9 has been reported to be found in higher levels in patients with periodontitis than with clinically stable condition, and have been associated with cardiovascular disease, cancer, multiple sclerosis, and neuropsychiatric disorder.57 Phenylalanine, valine, and lactic acid are salivary metabolites that could distinguish patients having oral leukoplakia and HNC especially OSCC from healthy controls.58 One study reported that oxidative stress markers such as 8-hydroxy-22-deoxyguanosine, manondialdehyde, and antioxidant enzymes such as glutathione peroxidase and superoxide dismutase have higher levels with the severity of periodontitis in association with HNC.59 Salivary biomarkers for the co-existence for both periodontitis and HNC will be a sensational innovative diagnostic tool. Hence, further studies using salivary biomarkers for HNC should be indicated.
There are several limitations in our study. Firstly, our study was based on published studies controlling for different confounding factors. For estimating more definitive association, all well-known confounders should have been included in all studies and more information about periodontal microbiomes should be addressed. Secondly, the assessment method of periodontal disease varied between studies, which resulted in high heterogeneity. Taking everything into account, these limitations may affect our final conclusions. To overcome these limitations and show more clear evidence on the link, further studies including following items should be indicated: 1) designed as a hospital cancer case – community cohort control study, 2) a pilot study should be done to estimate adequate sample size, 3) alveolar bone level using panoramic radiograph should be used as an assessment method of periodontitis, 4) adjustments of covariates such as age, gender, socio-economic status, smoking, drinking, oral health status such as tooth loss, dental visits, diet, periodontal microbiomes, viral infection such as HPV, pre-cancerous oral mucosal lesions, systemic diseases such as diabetes, hypertension, hypercholesterolemia, obesity, and medication. Notwithstanding these limitations, our meta-analysis using 22 studies was adequate enough to estimate the association of OHS-P with HNC.
In conclusion, our meta-analysis using 22 studies showed that bad OHS-P was associated with the risk of HNC. Periodontitis defined by ABL or CAL showed stronger association. The association was stronger especially in fair or good quality studies and in Asia studies. Thus, physicians and dentists should be aware of the importance of OHS-P on head and neck cancer.
 XML Download
XML Download