

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Suicide is one of the leading causes of death worldwide among adolescents and young adults.1 Suicide was the fifth leading cause of death in all age groups and the top cause of death for people aged 10 to 39 in Korea in 2017.2 Like other countries in which suicide is a leading cause of death in soldiers,345 the Ministry of National Defense of Korea reported that suicide has been the leading cause of death among soldiers for the past 10 years, and 65.1% of total deaths (56/86) were attributed to suicide in 2018.2
At a general population level, various factors were identified as predictors of suicidal behaviors. In addition to well-established risk factors such as depression or substance use disorder, sleep disturbance, psychological and physical trauma due to accidents and intoxication may also work as predictors of suicidal behavior.678910 Moreover, physical conditions such as obesity or low body mass index (BMI) were also reported as risk factors for suicide.1112
In the military population, child abuse exposure and insomnia were previously reported to increase suicide behaviors as well as in the general population.1314 In considering unique characteristics of the military, studies have looked into potential risk factors such as male gender, race/ethnicity, junior enlisted rank, recent demotion, current or previous deployment, post-traumatic stress disorder, depression, and previous suicide attempts that are significantly linked with an increased risk of suicidal behavior during the military service.4151617
For protective factors, there have been a few studies identifying potential protective factors of suicidal behaviors such as resilience, and post-deployment social support.1819
Given that suicidal behavior such as suicidal ideation, planning and attempts develop through complex interactions between risk and protective factors of the host and the environment, and soldiers are being exposed to stressful environments such as military training, deployment to remote areas, and combat experience that may affect their mental health, research has been conducted to identify risk factors and protective factors of suicidal behavior in the military population. In Korea, there are cross-sectional studies that have sought to identify risk factors of suicidal ideation in military soldiers. An et al.20 reported that suicidal ideation in soldiers is related to stress, depression, age, and educational level. Other studies have demonstrated potential predictors of suicidal ideation such as depressive symptoms, a low prospect for the future, work-related stress, and low status of general mental health.21 Lee et al.22 reported a significant association of depressive symptoms and stress in military soldiers who have a history of suicide-related behavior. However, those studies have been conducted with small scale surveys that involved a single or number of military bases only. Therefore, the findings from those studies need to be examined with a large-scale survey that is representative.
In 2014, the Ministry of National Defense of Korea directed the Armed Forces Medical School to undertake a military-wide survey to generate representative health data. Using this data, we seek to estimate the prevalence of suicidal ideation in the Korean Armed Forces (KAF). In addition, we also aim to identify potential risk and protective factors of suicidal ideation. In identifying those factors in the study population, we propose the following hypotheses:
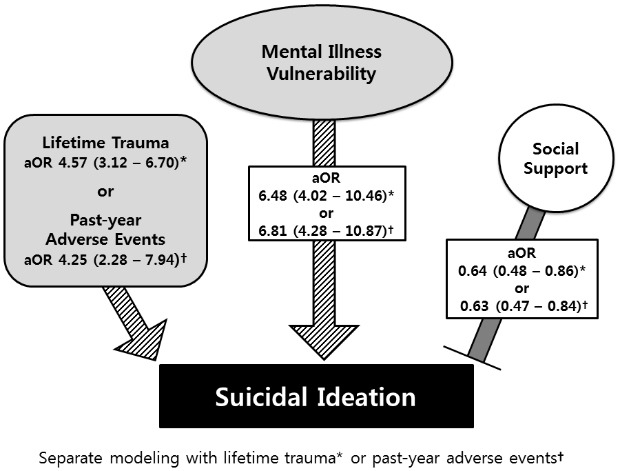
• The likelihood of having had suicidal ideation in the previous year would be higher in military personnel who report past year adverse events (PAE) such as accidents or intoxication; lifetime trauma; and those with vulnerabilities to mental illness.
• The likelihood of having had suicidal ideation in the previous year would be lower in military personnel who report higher perceived social support from family, friends, and peers.
Go to : 
METHODS
2014 Military health survey (MHS)
The MHS is designed to collect representative health data for the KAF such as general health status, health behavior, trauma and safety, quality of life, morbidity, mental health, social support, and health service utilization across all services (Army, Navy, Air Force, and Marines).23 The survey was carried out in 40 military units selected by stratified random sampling in consideration of the type of service, gender, rank, operation area (frontline or rear), and unit size to adequately represent the active duty KAF.
The first wave of the MHS was conducted in 2013 as a pilot study. For this study, we analyzed data from the second wave in 2014. The survey was carried out by the Armed Forces Medical School in Daejeon, Korea, which was to manage the entire survey processed in the year. The MHS is an anonymous self-administered survey that does not collect personally identifiable information. The survey agency trained survey site coordinators for the distribution of survey questionnaires and to assist responders with any inquiries regarding answering the survey and control for the quality of responses. A total of 7,763 conscripted and professional soldiers participated in the survey with informed consents.
Measures
In order to identify the relationships of PAE of accident or intoxication and accumulated lifetime trauma (ALT) with suicidal ideation, we extracted variables that may have confounding effects on explanatory and dependent variables. Demographic variables such as age, sex, educational level, and marital status were included as they have been repeatedly demonstrated as risk factors for suicide.24 Occupational variables such as military rank, service, work-related and living-related stress were included in the analysis as they have been previously suggested as risk factors to suicide behaviors.417 Physical and mental health-related variables such as subjective health status, health behavior, BMI, smoking history, number of PAE episodes (0, 1, 2, and 3 or more), sleep hours per day, satisfaction with sleep behavior, and number of ALT episodes (0, 1, 2, and 3 or more) were also included since they were reported to influence on suicide behaviors.6891025
As with many other psychiatric illnesses, the pathway leading to suicide is heterogeneous and suicide behaviors involve complex interactions between the hosts and their environment. Therefore, we tried to include as many relevant factors as possible to investigate these complex behaviors comprehensively.
PAE of accident or intoxication
To count the number of PAE episodes, the survey firstly questioned: “During military service, have you experienced any accidents or intoxications in the past year that required medical services from clinics, hospitals, or emergency rooms?” The survey requested detailed information for each PAE event, recording the number of events, the type and location of accident or intoxication, the level of medical services received, whether the event was self-inflicted or not, and the length of absence from duty. After a respondent indicated the number of the episode(s), the total scores were added and categorized into 0, 1, 2, and 3 or more.
ALT
The participants were asked whether they had experienced any of the 17 events listed on the life events checklist, which has been previously translated into Korean and validated.26 The life events checklist has previously been suggested to be especially suitable for the military population.27 Positive responses were additionally probed for the frequency of each event. The total number of events was defined as ALT and categorized into 0, 1, 2, and 3 or more.
Kessler psychological distress scale (K10) for mental health screening
The MHS adopted the K10 to screen for mental health. It was developed to detect serious mental illness, previously defined as “any 12-month DSM-IV disorder, other than a substance use disorder, with a Global Assessment of Functioning score of less than 60.”28 The K10 is a brief 10-item self-measured instrument that outperforms the General Health Questionnaire and the short form of the Composite International Diagnostic Interview, both of which are widely employed for mental health screening.2829 The Korean version of the K10 demonstrates excellent internal consistency with a Cronbach's alpha of 0.924 and a cutoff point of 21 was suggested.30 This cutoff point was used to screen vulnerability to mental illness.
Perceived social support
While low social support has been suggested to increase the risk of suicide attempts,31 good social integration has been demonstrated to be protective against death due to suicide.3233 The MHS assessed the degree of perceived social support using measures adapted from a previously developed instrument for scoring social support using four questions: “I feel loved and cared for,” “I am appraised as needed and worthy,” “When making important decisions, advice and suggestions are given,” and “When I need them, money or materials are provided.” These questions correspond to four subcomponents of social support in terms of emotional, appraisal, informational, and tangible support, respectively.34 Social support was evaluated in the context of five potential support groups (professional soldiers with higher ranks, conscripted soldiers with higher ranks, fellows or lower-ranked comrades, family members, and friends outside the military) for conscripted soldiers and four groups (superiors, fellows, family members, and friends outside the military) for professional soldiers. The participants responded to each question on a 4-point Likert scale of “Strongly disagree,” “Disagree,” “Agree,” and “Strongly agree.” “Strongly disagree” and “Disagree” were treated as 0, while “Agree” and “Strongly agree” were scored as 1. We categorized participants by bisecting the total score of social support with the closest natural numbers to mean value in both groups (low and high). The low social support group included those with scores of 11 or less for conscripted soldiers and 10 or less for professional soldiers. The high social support group included those with scores between 12 and 20 for conscripted soldiers and between 11 and 16 for professional soldiers. These categories may reflect differences in the numbers of potential support groups available to conscripted and professional military members.
Statistical analysis
We analyzed data using χ2 and multivariate logistic regression analyses in SAS version 9.3 (SAS Institute, Cary, NC, USA). A descriptive analysis of relevant variables according to the presence of suicidal ideation was performed using the χ2 test. We used multivariate logistic regression to identify relationships in controlling for other covariates of suicidal ideation such as socioeconomic status, work-related stress factors, physical health, mental health, and health behavior. Statistical significance was set at P < 0.05, and 95% confidence intervals (CIs) were reported as appropriate.
Ethics statement
We obtained ethical clearance from the Institutional Review Board of Uijeongbu St. Mary's Hospital, Catholic University of Korea (UC17EESI0093) for accessing secondary data from MHS to conduct this study and the requirement for informed consent was waived.
Go to :
RESULTS
Among 7,763 survey respondents, 6,377 were eligible for the study. Table 1 shows demographic information for participants, with the proportion of participants reporting suicidal ideation in the previous year. Two hundred twenty-seven men (3.7% of 6,150) and 14 women (6.2% of 227) reported suicidal ideation. The survey also asked whether the study subjects had experienced “suicide plans” and “suicide attempts” in the recent year. Among 6,377 participants, 44 (0.69%) responded suicide plan and only 17 (0.27%) responded suicide attempts. Low military ranks such as trainee, private, and private first class reported higher proportions of suicidal ideation in the past year. Active duty military members with mental illness vulnerabilities were significantly more likely to report suicidal ideation than those without mental illness vulnerabilities (39.5% vs. 3.2%, P < 0.001). ALT and PAE were also associated with suicidal ideation.
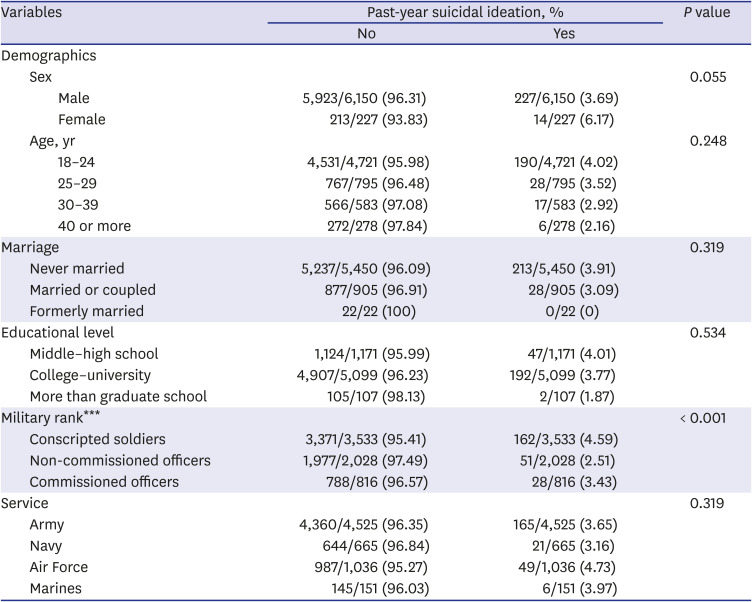
Table 1
Prevalence of suicide ideation in the previous year according to demographic variables (n = 6,377)
![]()
The level of perceived stress also affected suicidal ideation. Suicide ideation was significantly more likely to be displayed by active-duty military members, who experienced high levels of stress from work (8.5% vs. 1.8%, P < 0.001) and in their personal life (13.4% vs. 2.7%, P < 0.001) than in those with lower degrees of perceived stress (Table 2).
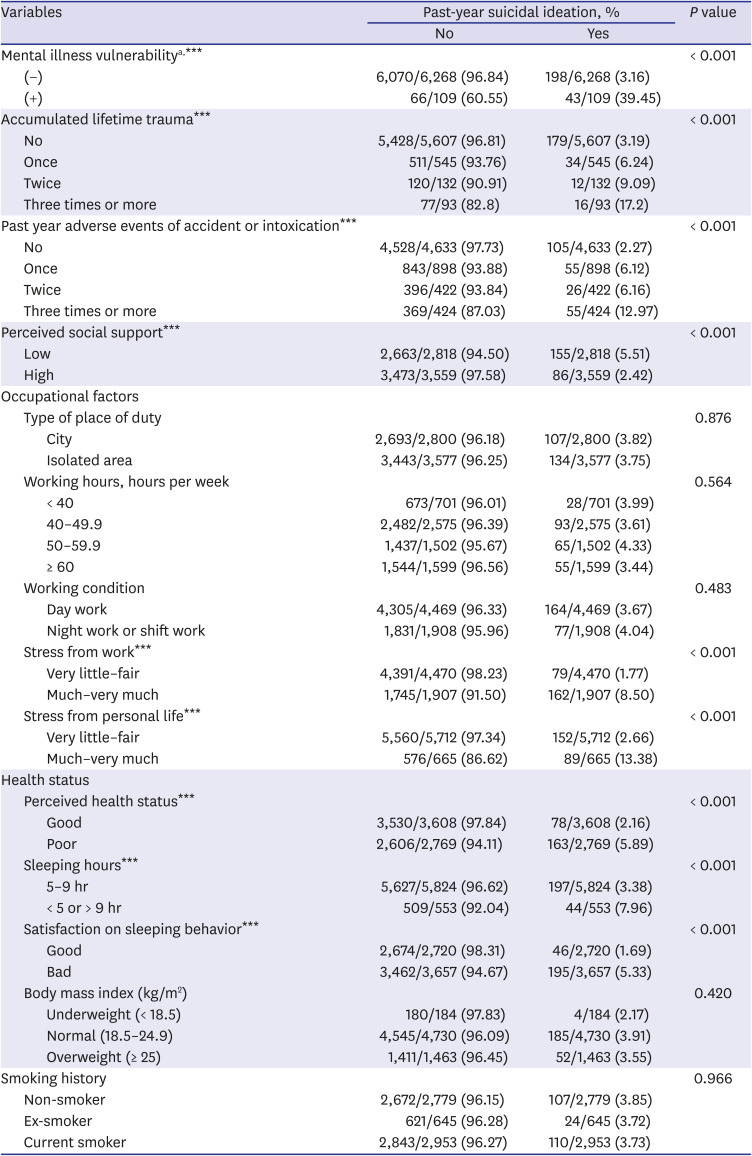
Table 2
Factors related to suicidal ideation
![]()
Regarding general health status, active duty military members reporting poorer perceived health, abnormal sleeping hours (less than 5 hours or more than 9 hours per day), and poor sleeping quality were more likely to report suicidal ideation in the past year. However, high levels of perceived social support were associated with significantly decreased suicidal ideation compared to those with a lower level of perceived social support (2.2% vs. 5.5%, P < 0.001).
To reflect the diverse variables that exerted significant influences on suicidal ideation in the descriptive analysis, 3 analytic models were used to control for covariates. The explanatory variables of mental illness proneness, PAE, ALT, and social support all remained significant in every model.
Participants with mental illness vulnerabilities were significantly more likely to report suicidal ideation in all models and were more than six times more likely to report suicidal ideation in the final model, taking PAE, ALT, and social support into account. In contrast, participants receiving social support were less likely to report suicidal ideation, with adjusted odds ratio (AOR) of 0.63 and 0.64 for PAE and ALT models, respectively (Table 3).
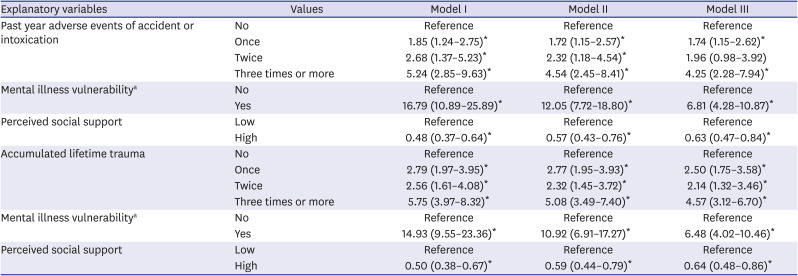
Table 3
Multivariate logistic regression of suicidal ideation, accumulated trauma, past year accidents, and social support
Data are expressed as mean (95% confidence interval) unless otherwise indicated.
Model I = adjusted for age, sex, educational level, marital status, military rank, and type of military service, model II = model I + adjusted for perceived health status, sleeping hours, satisfaction on sleeping behavior, body mass index, and smoking, model III = model II + working hours, working conditions, work-related stress, and personal stress.
aDefined as score ≥ 21 on Kessler psychological distress scale-10.
*P < 0.05.
![]()
In model III, we examined the dose-response relationship of suicidal ideation with both PAE and ALT: 1 PAE episode (AOR, 1.74; 95% CI, 1.15–2.62), 2 PAE episodes (AOR, 1.96; 95% CI, 0.98–3.92), 3 or more PAE episodes (AOR, 4.25; 95% CI, 2.28–7.94), 1 ALT episode (AOR, 2.50; 95% CI, 1.75–3.58), 2 ALT episodes (AOR, 2.14; 95% CI, 1.32–3.46), 3 or more ALT episodes (AOR, 4.57; 95% CI, 3.12–6.70).
Go to :
DISCUSSION
In this study, we examined the relationships between recent or lifetime adversities, and suicidal ideation by analyzing representative health data of the KAF collected in 2014. The rate of suicidal ideation in the study sample was similar to that of the general population for the same age group.35
In addition to PAE and ALT, our descriptive analysis demonstrated that soldiers with lower military ranks, poor perceived health, abnormal sleeping hours, and high stress in both work and personal life experience higher rates of suicidal ideation than others. However, military service members with vulnerabilities to mental illness were at the highest risk for suicidal ideation.
The multivariate logistic analysis demonstrated that both PAE and ALT are significantly related to increased suicidal ideation. Our analytic models also identified a dose-response relationship indicating that the impact of accident and intoxication episode(s) in the past year and of lifetime trauma episode(s) may have a cumulative effect on the likelihood of suicidal ideation. This result is consistent with previous studies.7917 A similar relationship was found in a study that reviewed mental health data from low, middle, and high-income countries and demonstrated that suicidal ideation, planned suicide attempts, and unplanned attempts increase as the number of reported traumatic events increases.7
We suggest that soldiers reporting recent accidents, intoxication, or major adverse events should be evaluated systematically and supported with appropriate interventions. In order to identify soldiers at high risk of suicide, the defense authority should conduct the MHS more widely and on a regular basis to protect mental health and reduce non-combat mortality among service members. When implementing such policy, a cautious approach is needed to avoid stigmatization of those who utilize mental health services in the military.
Suicide is regarded as an end-stage of interactions between environmental and genetic influences on suicidal behavior.36 A growing body of evidence suggests that environmental factors exert greater influence than known genetic factors in terms of negative psychological outcomes such as suicidal behavior and depression.37 Soldiers are exposed to various combat and non-combat related stressors. Therefore, assessment of suicidal behavior among soldiers should include such environmental factors. Social support was identified as a potential modifiable environmental factor to decrease suicidal ideation in both our descriptive analysis and in our multivariate analysis. Our findings are in line with those of previous studies that indicated the protective effects of social support against suicidal ideation.1738 However, to the best of our knowledge, this study is the first to demonstrate the protective role of social support in a large-scale, nationally representative sample of the Korean military. Future studies are needed to consolidate our findings and to develop effective interventions to strengthen social support.
In a Canadian study that compared rates of suicidal ideation in the previous year between the active military population and the general population, suicidal attempts were significantly lower in the active military population, but no difference was shown for suicidal ideation between the two samples.39 Thus far, it remains unclear whether military service members experience suicidal ideation less or more often than the general population. However, our study revealed that a considerable number of military members thought about suicide in the previous year.
The national statistics for Korea indicate that the suicide rate in the military was 60% lower than the suicide rate in the general population in the same age groups in 2016.2 In our data set, only seven responses of self-harm were identified for individuals reporting accident/intoxication. This number might be under-estimated because the survey was conducted by a military unit, and concerns about potential punishment may have contributed to underreporting. This limitation makes it more difficult to analyze how previous instances of self-harm are related to suicidal ideation.
We should note several limitations of the present study. Firstly, we were unable to differentiate between the influences of different types of trauma (child abuse, sexual violence, criminal victims, etc.). A previous study that analyzed the world mental health survey data suggested that the effects of trauma may vary according to the type of inflicted trauma.7 Secondly, in this study, we used a cross-sectional data set that limits our ability to establish causality of factors. This question requires prospective studies to explore the causality of factors suggested by the analytic models. Thirdly, we analyzed suicidal ideation, which is only part of suicidal behavior, due to the scope of the survey. Subjects were asked about self-harm in the mental health section of the survey, but few soldiers responded by describing their previous attempts. Therefore, insufficient evidence about suicidal behavior in Korean military personnel limits our ability to analyze risk factors related to suicidal attempts and planning. In order to avoid under-reporting in the future, a neutral or independent agency should be engaged in conducting the next waves of the survey. Fourth, even though the survey participants were questioned whether they had suicidal ideation in the recent year, it did not further ask the presence of suicidal ideation before joining the military service if their military service had started within one year. Due to this limitation, authors were not able to see how suicidal ideation before joining military service may have an association with suicidal behaviors developed during the service. Fifth, the dataset analyzed in this article used data from a total of 6,377 who responded to all variables required for the analysis. This is to ensure completeness of the dataset to be analyzed but there is potential selection bias that this study may have excluded those who had not provided all required information. Lastly, the data was derived from the paper-pencil survey method. Although the relatively large sample size of this study has an advantage in reducing respondent bias by insincere responses, future studies that deploy objective assessments will overcome our limitation.
In conclusion, this study demonstrated that a similar prevalence of suicidal ideation to those in the general population was found in the KAF. Lower military ranks, abnormal sleeping hours, poor perceived health, and distress from personal/military life were associated with higher suicidal ideation in the active-duty military members. Exposures to recent adversities or lifetime traumatic events demonstrated dose-dependent relationships with suicidal ideation. Mental illness vulnerability contributed the most to suicidal ideation. This study strongly emphasizes the need to detect and treat subjects with mental illness vulnerability to reduce suicidal ideation in active duty servicemen. Social support was associated with a reduced likelihood of suicidal ideation.
The suicide research in military members may provide important insight. Firstly, various factors such as mental disorders, personality, occupation/finance, interpersonal relationships, religions, etc. exert their influence over suicide behaviors either alone or by interaction with each other. These complex phenomena may act as confounders and obscure reality. Since suicidal behavior involves complex interactions of environmental and individual factors, a comprehensive approach is necessary and research in a homogenous population like military serviceman could be useful in suicide research as its members work and live under rather a controlled environment with comparable occupational exposure to suicide risk. Moreover, military members are often under higher distress both in combat and non-combat situations compared to the general population. The major finding of this study is the identification of mental illness vulnerability as the most profound predictor of suicidal ideation in the KAF. Recent adversities or lifetime traumatic events also exerted additional risk while social support significantly reduced the likelihood of suicidal ideation. These findings are in line with study findings from the general population and provide us useful insight to enhance our effort to prevent suicide.6789
Measures to strengthen social support from colleagues, superiors, and family members may act as a protective factor against suicidal ideation. In addition, our findings suggest that suicidal behavior in the military may be reduced by implementing policies to increase utilization of mental health services, and screen those with greater loading of recent and lifetime traumatic experiences. Given the limited ability to determine causality due to our use of cross-sectional data, well-designed longitudinal studies are needed to concretize our findings.
Go to :
 XML Download
XML Download