

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Endocrine Society guidelines recommend long-term dopamine agonist (DA) treatment as a first-line approach to treating prolactinoma.1 However, despite the high therapeutic effect of DA,234 surgical approaches are preferred for several reasons: 1) potential side effects of long-term DA medication, 2) intolerance of DA, 3) nonresponders to DA. Approximately one-third of patients treated with DA complained of side effects such as nausea, vomiting, headache, and dizziness.5 Recently, the increased risk of cardiac valve disease in patients treated with long-term cabergoline was reported.67 Furthermore, relapse of hyperprolactinemia has been shown in several studies.8910
On the one hand, pituitary surgery reported higher than 80% of long-term remission rates for patients with microprolactinomas.111213 According to this literature, prolactin (PRL) levels return to normal, and gonadal dysfunctions are recovered after complete surgical resection. Additionally, the development of pituitary surgery has markedly improved the clinical outcomes during the last two decades.1415 The surgical morbidity rate for prolactinomas is infrequent and has been reported to be less than 1% in specialized pituitary centers.1213151617 Notably, the microscopic transsphenoidal approach (TSA) for prolactinomas is accepted for a distinct number of indications, namely, nonresponders to medical therapy, those with an intolerance for DA, and those with neurologic deficits, such as rapid loss of vision or cranial nerve palsy due to tumor hemorrhage or apoplexy. We focused on evaluating surgical outcomes in patients with prolactinomas who opted for primary pituitary surgery instead of long-term therapy with DA.
METHODS
Patient selection
Clinical data, such as age and sex, were retrieved from electronic medical records. This retrospective study included a consecutive series of 96 patients who underwent primary pituitary surgery without prior DA treatment for prolactinomas at the Department of Neurosurgery, Seoul National University Hospital, between June 1990 and December 2010. The indication for first-line pituitary surgery for all the patients in this study was a patient's preference for surgery rather than long-term DA therapy. We excluded all cases of residual and/or recurrent prolactinomas. A microprolactinoma was defined as a tumor of 1–10 mm; a macroprolactinoma was a lesion of 10–20 mm in diameter. The preoperative data included history and physical examination, PRL levels, and the results of imaging studies. All operations were performed by TSA while the patients were in a supine position.
Hormonal assessment
PRL measurements were performed at the Department of Laboratory Medicine, Seoul National University Hospital. To check PRL, a radioimmunoassay (RIAKEY Prolactin IRMA Tube; Shin Jin Medics, Goyang, Korea) was used to measure the serum PRL level; normal PRL levels were considered to be 5–20 ng/mL and 5–25 ng/mL for men and women, respectively. Complete remission (CR) was defined as a normalized PRL level below 20 μg/L the morning after surgery. Long-term follow-up PRL levels, which were determined at the discretion of the referring physician, and clinical symptoms of hyperprolactinemia were obtained by the patient's referring physician. We defined a radiologic recurrence as local progression observed on radiologic images and a biologic recurrence as hyperprolactinemia (> 20 μg/L) during the follow-up period.
Assessment of invasion into the cavernous sinus
We have adapted the Knosp grading system to evaluate the cavernous sinus invasion of prolactinomas. The Knosp classification includes five grades: 1) grade 0, no invasion with all of the lesion medial to the cavernous carotid artery; 2) grade 1, invasion extending to, but not past, the medial aspect of the cavernous carotid artery; 3) grade 2, invasion extending to, but not past, the lateral aspect of the cavernous carotid artery; 4) grade 3, invasion past the lateral aspect of the cavernous carotid artery, but not completely filling the cavernous sinus; 5) grade 4, tumor completely filling the cavernous sinus both medial and lateral to the cavernous carotid artery.18
Statistical analysis
Values are expressed as the mean ± standard deviation or median (range). The χ2 test or Fisher's exact test were used to compare categorical data. Cox proportional hazard models were used to analyze the recurrence predictors. Cox proportional hazard models were used to analyze the predictive variables for CR after TSA. The Kaplan-Meier survival curves for remission after surgery are presented based on the selection criteria. SPSS software (version 22.0; SPSS Inc., Chicago, IL, USA) was used for statistical analyses. The cut-off level for significance was set at P < 0.05.
RESULTS
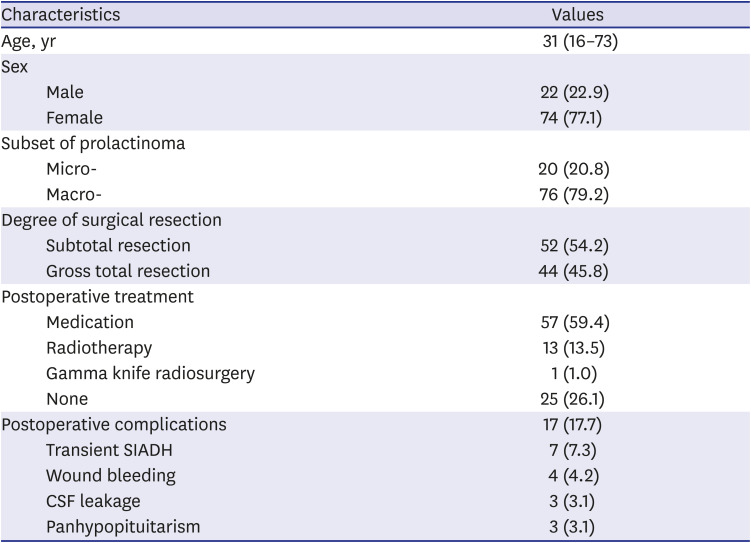
This consecutive series consisted of 74 female and 22 male patients. The median age of the patients was 31 years with a range from 16 to 73 years. The median follow-up period was 139.1 months for all patients (range, 12.2–319.6 months). Twenty patients (20.8%) harbored microprolactinomas, and 76 patients (79.2%) harbored macroprolactinomas. Of these patients, 52 patients underwent subtotal resection and 44 had gross total resection. The median preoperative PRL level was 434.8 ng/mL (range, 24.3–25,000 ng/mL). After TSA, the values of PRL dropped significantly from a median 86.8 ng/mL (range, 1–18,500 ng/mL). All of the patients who underwent TSA achieved surgical reduction as well as a DA dose decrease. There was no need for further treatment of 25 patients after surgery, and 57 patients continued to receive reduced dose of DA, 13 received postoperative radiotherapy, and one received Gamma Knife radiosurgery. There were postoperative complications in 17 patients (17.7%), but none of them had permanent disabilities and there was no mortality. In detail, 7 patients (7.3%) had transient diabetes insipidus lasting up to one week. Postoperative bleeding was recorded in 4 patients (4.2%), cerebrospinal fluid (CSF) leakage in 3 patients (3.1%), and panhypopituitarism in 3 patients (3.1%). Table 1 describes the demographic characteristics of the patients in the study.
Table 1
Patient characteristics and clinical outcomes after microscopic transsphenoidal approach for prolactinomas
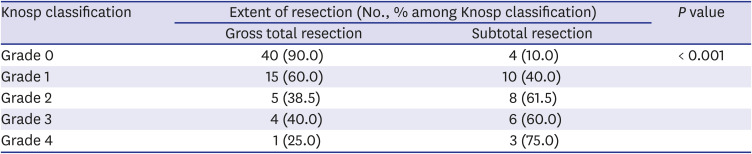
Following surgery, a normalization of the PRL values was achieved in 46 of 96 patients (47.9%). Among them, 25 patients achieve CR after surgery, and the remaining 21 patients achieved CR within six months using reduced dosage DAs. However, 50 patients did not achieve CR during the follow-up. In fact, 21 patients had recurrence during the follow-up period, and the final CR rate was 26% (25/96) at the last follow-up. We compared several factors associated with the outcomes of patients who achieved CR and those who did not (Table 2). CR was not correlated with sex, age, visual symptoms, or postoperative radiotherapy. The PRL level at diagnosis was significantly higher in the no remission group than that in the remission group. Particularly, a PRL level greater than 1,000 ng/mL was statistically associated with no remission after surgery. Although for macroprolactinomas were only able to identify their trends without significant differences, the rate of gross total resection and less frequent invasion of the cavernous sinus were significantly higher in the remission group (P < 0.001, Table 2). Surgical outcomes are given in Table 3. There were statistically significant differences between the extent of resection and the Knosp classification (P < 0.001).
Table 2
Comparison of clinical outcome after microscopic transsphenoidal approach
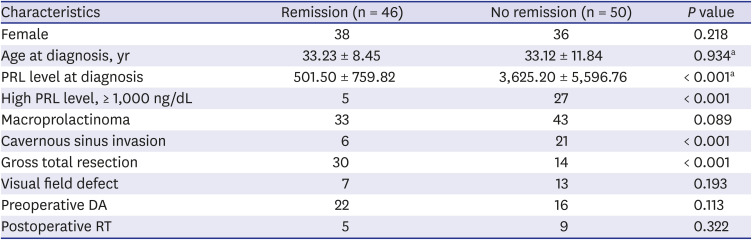
Table 3
Tumor resection according to the Knosp classification
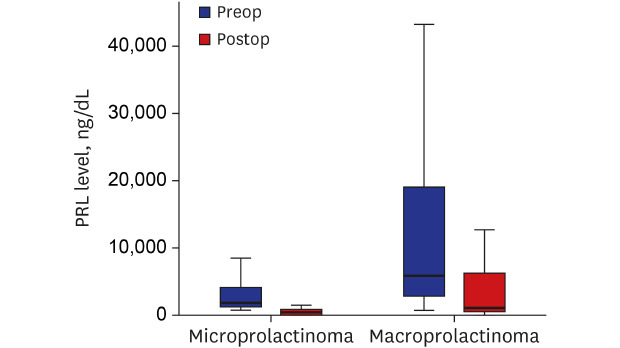
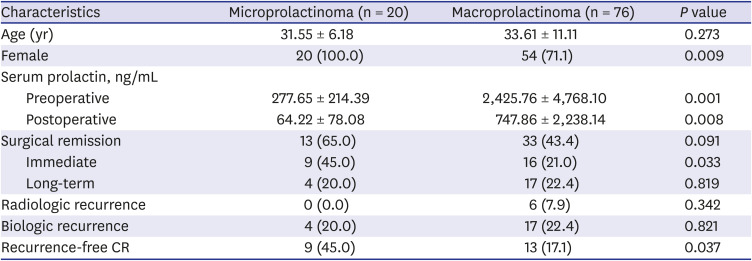
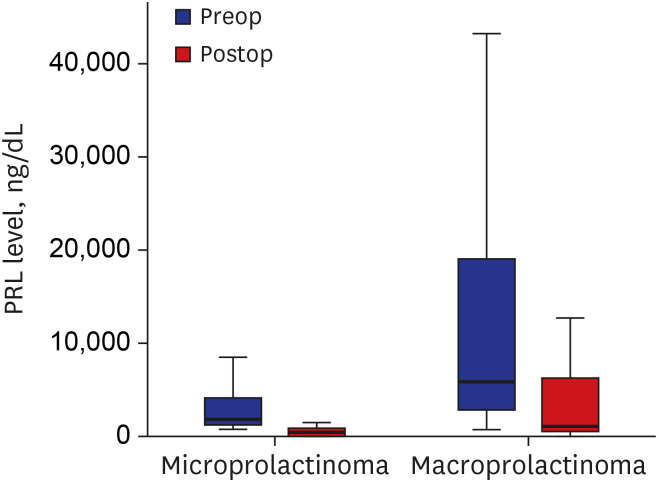
Of the 96 patients who underwent TSA, 76 patients had a macroprolactinoma (79.2%, Table 4). Patients with microprolactinomas had significantly lower pre- and postoperative PRL levels than patients with macroprolactinomas (Fig. 1). However, the PRL reduction rate after TSA showed no statistically significant difference (77.01% in microprolactinoma vs. 70.02% in macroprolactinoma, P = 0.268). In the microprolactinoma group, 13 patients achieved surgical CR (13/20, 65%), nine of whom improved immediately after surgery. Compared to the microprolactinoma group, surgical CR was achieved in 33 patients (33/76, 43.4%), and 16 of them improved immediately after surgery. The remaining 17 patients achieved CR within six months. There were no patients with radiologic recurrences among the microprolactinomas, but six patients with macroprolactinomas had a radiologic recurrence. Of the six macroprolactinoma patients who showed a radiologic recurrence, three patients failed to complete the treatment, and three patients achieved CR and then experienced a recurrence. Biological recurrence was observed in four patients with microprolactinoma and 17 patients with macroprolactinoma. Therefore, the recurrence-free CR rate was 69.2% (9/13) in microprolactinomas and 39.4% (13/33) in macroprolactinomas, which was a statistically significant difference (P = 0.037).
Table 4
Characteristics of patient with micro- and macroprolactinoma
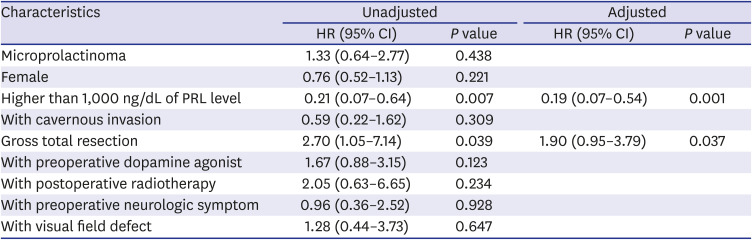
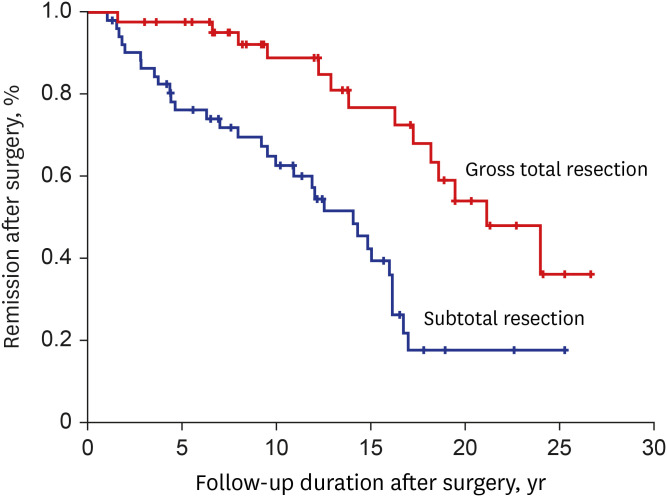
We conducted Cox-proportional hazard model analysis to identify the predictors for remission after surgery (Table 5). We included several variables that had been considered significant in other studies as well as the significant parameters presented in Table 4. Higher PRL levels at diagnosis and the presence of gross total resection were statistically significant as predictors for patients who achieved surgical CR after TSA. The results obtained from the adjusted Cox-proportional hazard model indicate that the initial PRL level at diagnosis was significant (P = 0.001). The patients who had a greater than 1000 ng/dL PRL at diagnosis had 81% less hazard in comparison with the patients who had lower PRL levels (hazard ratio, 0.19; confidence interval, 0.07–0.54). Kaplan-Meier survival curves for CR after endoscopic endonasal transsphenoidal approach showed statistically significant differences according to the extent of surgery (P < 0.001, Fig. 2).
Table 5
Predictors for surgical complete remission after microscopic transsphenoidal approach
DICUSSION
It is beyond doubt that DA treatment is the first-line approach for prolactinomas. However, as the Committee recommended, there are cases in which surgical treatment is needed.1920 Additionally, recent developments in surgery have further reduced the incidence of complications, leading to an era in which a new approach is needed in regard to the usefulness of surgical treatment of prolactinoma. From that point of view, our study provides a basis for reconsidering the use of surgery as a treatment for prolactinoma.
A recent meta-analysis demonstrated that transsphenoidal surgery could be an alternative first-line treatment for patients with prolactinomas, especially microprolactinomas.21 The authors showed that a long-term remission rate was achieved in 88% of the surgery group compared with 52% of the DA group. Particularly, long-term remission after surgery for microprolactinomas was higher than that for macroprolactinomas (91% vs. 77%). Unfortunately, our results were inconsistent, with 47.9% CR rate and a 47.8% recurrence-free CR rate. However, in terms of micro/macroprolactinomas considered separately, the CR rates were 65% and 43.4%, respectively, which are consistent with other studies.2223 These prior reports showed that surgical resection achieved to 63–72% CR rate for microprolactinomas and 32–60% for macroprolactinomas. Even for the macroprolactinomas, since more than half of the 34 patients who achieved CR after surgery achieved long-term CR, this result might support the usefulness of surgery. Furthermore, our findings could serve as a basis for surgical treatment in selective microprolactinom patients, as the recurrence-free CR rate of microprolactinoma has been relatively low compared to those of macroprolactinoma.
The recurrence of hyperprolactinemia is common, affecting approximately 80% of patients who have stopped DA treatment for prolactinomas.424 Moreover, there is still debate over how long to maintain the DA treatment due to concerns about the side effects and long-term costs of DA. Therefore, minimally invasive surgery such as TSA might be considered to be an alternative treatment for prolactinomas. The most common complication of TSA is CSF leakage (2–16%) and a life-threatening hemorrhage affects less than 1% of patients, while the incidence of panhypopituitarism is variable, approximately 1–14%.252627 Our results showed no fatal complications, and only three patients had panhypopituitarism requiring medication. Thus, surgical approach, such as TSA, as a primary treatment for prolactinomas might be cautiously considered to be a safe strategy.
Although the response rate of DA treatment is above 80% for prolactinomas,1928 DA-resistant prolactinoma is observed in 10–30% of cases.29 Patients resistant to DA treatment and those who received high-dose DA might also profit from surgical resection. Although it is an incomplete resection, several reports have demonstrated that surgical debulking may improve hormonal control with normalization of PRL levels.2330 Our results showed that complete resection may be an important factor in achieving CR after surgery. Furthermore, the surgical benefit became more apparent as some patients with incomplete resection were also observed achieve CR. Therefore, these results are seen as the weak basis for allowing surgical treatment to be selected in microprolactinoma rather than macroprolactinoma. Additionally, understandably, the level of PRL in all patients who underwent surgery decreased immediately. However, the reduction in the PRL level was not related to the prolactinoma size.
Other considerations are the cost-benefit and the socioeconomic burdens. Several studies have focused on cost-effectiveness, comparing medical treatment and surgical resection for prolactinomas.3132 These reports demonstrated that surgical resection may reduce lower economic costs over 10 years. Although Chinese data showed contrasting results, the cost reduction could vary depending on the healthcare system.33 However, the information that prolactinoma can be removed immediately and definitively may offer patients a choice as to a preferred treatment based on their concerns, such as the use of a chronic medication or the long-term use complications of DA.
As reported in this study, the recurrence rate after TSA in 96 patients with prolactinoma was 47.9% during the 132 months of the median follow-up period. The extent of surgical resection and a lower initial PRL level were the predictors of long-term remission. Of the patients who met all the two criteria, 66.7% achieved CR after TSA. Another report also demonstrated that a successful cure rate is correlated with tumor size, invasion of the cavernous sinus, and degree of hyperprolactinemia.11 However, Song et al.34 reported that good prognostic predictors are preoperative tumor growth patterns and the Ki-67 index, not the degree of hyperprolactinemia.
Our study has several limitations. First, this study does not present the whole cohort of patients treated, which raises concerns about selection bias. Second, we did not evaluate the incidence of DA-resistant prolactinoma. Additionally, we did not assess the changes of neurological symptoms after TSA for prolactinoma. Finally, we did not investigate the Ki-67 index. Notwithstanding these limitations, we believe that our results might provide clinical evidence for the use of TSA for prolactinoma as an alternative treatment. Moreover, TSA is expected to be offered to patients because it has potential to provide a complete cure in one operation instead of long-term DA use.
Based on our results, we believe that TSA for selective prolactinoma is a viable therapeutic modality, especially in the case of microprolactinomas. For small-sized microprolactinoma, we cautiously propose to consider TSA for these selective patients, as the possibility of GTR is high after surgery and thus can increase the CR rate and the recurrent-free rate. The complication rate of TSA is low, and technical advances now allow us to consider surgical modalities for the treatment of prolactinoma. This option is also meaningful by allowing patients to choose treatments that can be expected to offer a permanent cure instead of long-term DA use. Despite several limitations, our results might help selected patients who are concerned about the complications of DA or who want to avoid the use of long-term medication.
 XML Download
XML Download