

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
According to the American College of Obstetricians and Gynecology (ACOG), the management of premature rupture of membranes is based on the gestational age at membrane rupture.1 With preterm premature rupture of membrane (PPROM), which is defined as membrane rupture that occurs between 24 and 33 weeks' gestation, conservative management is recommended, including antibiotics and corticosteroid treatment.1 Treatment for previable PPROM, which is defined as membrane rupture that occurs earlier than 24 weeks' gestation, is a combination of conservative management and induction of labor.123 Various outcomes have been reported by studies of infants born to women who received expectant treatment after exposure to previable PPROM.45678910 The probability of neonatal death and morbidity associated with PPROM decreases with a longer latent period from membrane rupture to delivery and with advancing gestational age (GA).10 Regardless of advanced obstetric treatment, delivery occurs within 1 week in at least half of women with PPROM.11 Clinically, intraamniotic infection among pregnant women with PPROM occurs in approximately 15–25%.12 In patients with membrane rupture at an early GA, there was a high incidence of intraamniotic infection,1314 which is associated with a relatively high rate of neonatal mortality and severe long-term neonatal morbidity among surviving infants.15 In particular, persistent oligohydramnios is associated with mortality in infants born to women with previable PPROM.16 Lung hypoplasia, which results from a number of conditions that are associated with fetal lung compression and oligohydramnios, is a serious complication of previable PPROM and mortality from this condition ranges between 50–100%.91718 Due to the contradictory outcomes of extremely preterm infants exposed to previable PPROM, the ACOG suggests that women presenting with previable PPROM should be counseled regarding the risks and benefits of expectant management versus immediate delivery.1 In accordance with the guidelines for the expectant management of women with previable PPROM, a nationwide comparative study of neonatal outcomes over the duration of PPROM exposure is lacking. In the present study, we compared neonatal outcomes according to the latent period from membrane rupture to delivery among extremely preterm infants exposed to maternal PPROM using the Korean Neonatal Network (KNN) database to assess whether PPROM with prolonged latency is an independent risk factor for neonatal outcomes during hospitalization.
METHODS
Patients
The KNN database prospectively registered the clinical information of the very low birth weight infants (VLBWIs, < 1,500 g) admitted to the 67 participating neonatal intensive care units (NICUs), which covered > 80% of VLBWIs in South Korea. Of the 3,305 extremely preterm infants born at 23–27 weeks' gestation between 2014 and 2017 who were registered in the KNN, 1,464 infants were born to pregnant women with PPROM. The dates and times of membrane rupture or the duration from membrane rupture to delivery in each infant were recorded. We calculated the GA at membrane rupture and latent period from membrane rupture to delivery. We excluded 126 infants who did not have a recorded date of PPROM. Then, we excluded 428 infants born to pregnant women whose latent period from membrane rupture to delivery was less than 24 hours, because we do not know whether they were inevitably delivered due to membrane rupture during preterm labor or whether they were selectively delivered as a therapeutic option for previable PPROM. We also excluded 26 outborn infants to avoid the skewed outcomes that may be encountered with resuscitation in the delivery room and the inevitable circumstances that occur during transfer. Considering previous studies on neonatal outcomes in extremely preterm infants exposed to prolonged PPROM,61920 the short latency group was defined as infants delivered after a latent period of < 7 days (n = 450), whereas the prolonged latency group was arbitrarily defined as infants delivered after a latent period of ≥ 7 days (n = 434).
Data on perinatal characteristics were obtained, including the GA at membrane rupture and delivery, sex, multiple births, mode of delivery, latent period from membrane rupture to delivery, maternal diabetes mellitus, maternal hypertension, antenatal corticosteroid use, oligohydramnios, histologic chorioamnionitis, and birth weight, and compared between the two groups.
To assess PPROM with prolonged latency as an independent risk factor for neonatal outcomes during hospitalization in extremely preterm infants exposed to maternal PPROM, we investigated the rates of bronchopulmonary dysplasia (BPD), sepsis, necrotizing enterocolitis (NEC), intraventricular hemorrhage (IVH), periventricular leukomalacia (PVL), and retinopathy of prematurity (ROP), overall mortality, and timing of death.
Definitions
We based our definitions on the KNN database operation manual for patient characteristics. Accordingly, GA was determined from the obstetric history based on the last menstrual period. Maternal steroid use was defined as the administration of any corticosteroid to the mother at any time before delivery to accelerate fetal lung maturity. Chorioamnionitis was confirmed by placental pathology. Oligohydramnios was defined as an amniotic fluid index of < 5 cm.21 Early pulmonary hypertension was defined only when accompanied by medical treatment after diagnosis based on echocardiography within 7 days postnatally. BPD was defined as the use of more than supplemental oxygen at 36 weeks' GA, corresponding to moderate to severe BPD using the severity-based definition of BPD in the National Institutes of Health consensus.22 IVH was defined as grade ≥ 3 according to the classification by Papile et al.23 PVL was defined as cystic PVL, based on either head ultrasound or cranial magnetic resonance imaging performed at ≥ 2 weeks of age.24 NEC was defined as ≥ stage 2b according to the modified Bell criteria.25 Sepsis was defined as a positive blood culture in symptomatic infants suggestive of septicemia and more than 5 days of antibiotic treatment.2627 ROP was defined as any treatment, including anti-vascular endothelial growth factor and/or laser ablative and/or surgical treatment, performed on VLBWIs to prevent visual loss.28
Statistical analysis
Continuous variables were expressed as mean ± standard deviation and categorical variables as numbers and proportions. Comparisons between categorical variables were performed using the χ2 test or Fisher's exact test, and those between continuous variables were performed using the independent t-test. The Kaplan-Meier method was used to describe survival up to discharge from NICU and was compared using the log-rank test. Infants discharged alive were considered to have survived to a postnatal age of 300 days. Multivariable analyses were used to identify factors associated with mortality or morbidities in extremely preterm infants exposed to PPROM with prolonged latency. When evaluating mortality in a multi-institutional NICU case mix, risk adjusters are usually used as perinatal factors.2930 These risk adjusters can be used to predict mortality or morbidity fairly well and are not influenced by physicians in the NICUs being evaluated, unlike postnatal factors. Therefore, we performed multivariate logistic regression analysis that included well-established risk factors for adverse short-term outcomes to assess PPROM with prolonged latency as an independent risk factor for neonatal outcomes in extremely preterm infants exposed to PPROM. We did not include perinatal factors, including Apgar scores, body temperatures at admission, and pH within 1 hour after birth, as covariates in the multivariate analysis to avoid variance inflation, given their strong correlation with neonatal outcomes. A P value of < 0.05 was considered statistically significant. Analyses were performed using SPSS version 25 (IBM Corp., Armonk, NY, USA).
Ethics statement
The KNN registry was approved by the Institutional Review Board at each participating hospital (IRB No. SMC 2013-03-002). Informed consent was obtained from each infant's parents at enrollment by the NICUs participating in the KNN according to the Korean Privacy Act and was waived only in the case of infants who died in the delivery room or early after admission to the NICU before informed consent was obtained.
RESULTS
Fig. 1 shows the latent period from membrane rupture to delivery in extremely preterm infants exposed to PPROM. Of all the infants enrolled in this study, the mean GA at membrane rupture, mean latent period, and median latent period from membrane rupture to delivery were 24.1 ± 2.4 weeks, 12.2 ± 14.3 days, and 6.0 days, respectively.
Fig. 1
Extremely preterm infants exposed to maternal PPROM by latent period from membrane rupture to delivery.
PPROM = preterm premature rupture of membrane.
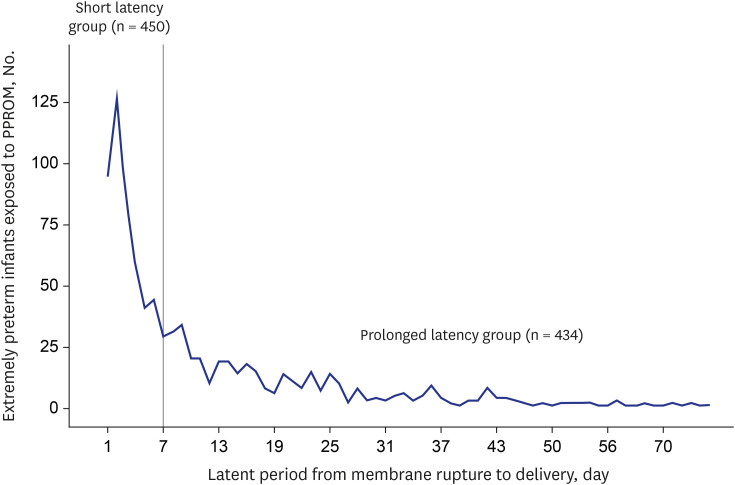
Table 1 shows the comparison of the prenatal characteristics between the prolonged and short latency groups. The mean GA at membrane rupture in the prolonged latency group was significantly lower than that in the short latency group (22.7 ± 2.5 vs. 25.4 ± 1.3 weeks, P < 0.001). Conversely, the mean latent period from membrane rupture to delivery in the prolonged latency group was significantly longer than that in the short latency group (21.8 ± 15.3 vs. 2.9 ± 1.6 days, P < 0.001). Nevertheless, the mean GA at delivery and birth weight were not significantly different between the two groups. The incidences of oligohydramnios and histologic chorioamnionitis in the prolonged latency group was significantly higher than that in the short latency group (38.7 [155/401] vs. 26.1 [105/403], 69.8 [270/384] vs. 61.0 [242/397], respectively, P < 0.05). There were significantly different rates of multiple pregnancy in the prolonged and short latency groups (30.2 [130/434] vs. 17.8 [80/450], P < 0.05), but this was not the case for sex, delivery mode, maternal diabetes, maternal hypertension, or the use of antenatal corticosteroids.
Table 1
Prenatal characteristics of the prolonged and short latency groups
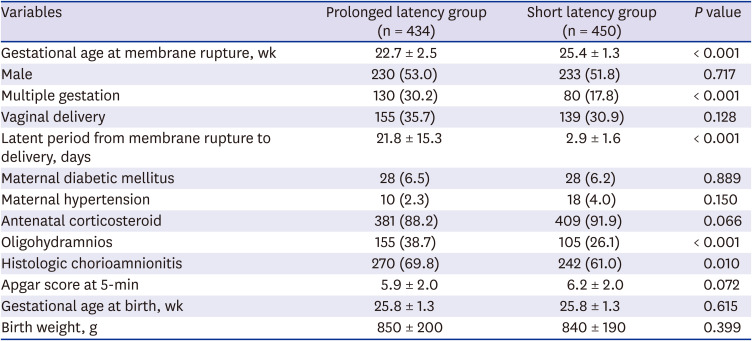
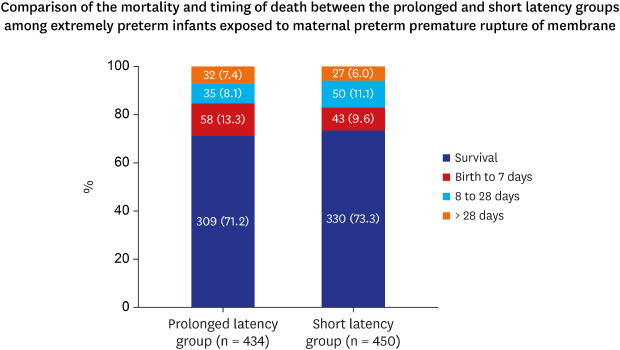
Fig. 2 shows the mortality rates of the two groups. Although the survival rate in the prolonged latency group was higher than that in the short latency group, it was not significant. Regarding the timing of death, mortality within the period between birth and 7 days postnatally was the most common, but there was no significant difference between the two groups. The survival curves of the two groups are shown in Fig. 3. On postnatal days 30 and 60, the probability of survival for an extremely preterm infant in the prolonged and short latency groups was 78.3% and 73.3% and 79.1% and 76.8%, respectively. The mean survival times in the prolonged and short latency groups were estimated at 223.7 ± 9.3 days (range: 205.5–241.9) and 223.4 ± 15.2 days (range: 193.6–253.2), respectively. It was expected that 75% of infants in the prolonged and short latency groups would survive after 90 and 43 days, respectively. However, we did not detect significant heterogeneity in the changes in overall mortality between the two groups.
Fig. 2
Comparison of the mortality and timing of death between the prolonged and short latency groups. The data are presented as number (%).

Fig. 3
Survival curves up to 300 days postnatally for extremely preterm infants exposed to preterm premature rupture of membrane. The time in days of postnatal hospitalization survival was estimated using the Kaplan-Meier method and log-rank test.
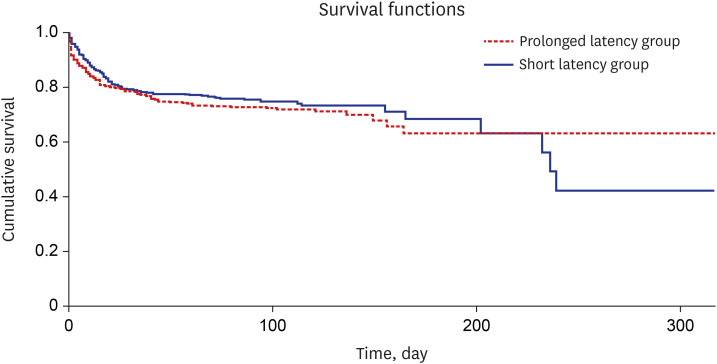
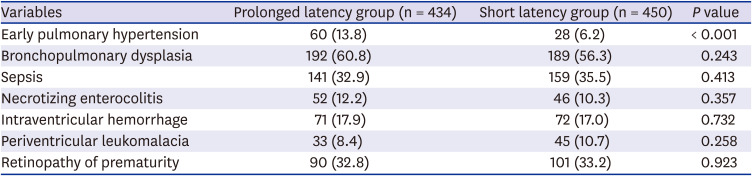
Table 2 presents the comparison of the neonatal outcomes between the two groups. The early pulmonary hypertension rates in the prolonged latency group were significantly higher than those in the short latency group (13.8 [60/434] vs. 6.2 [28/450], P < 0.001). However, the BPD and sepsis rates in the prolonged latency group were not significantly increased. There were no significant differences in the NEC, IVH, PVL, and ROP rates between the two groups.
Table 2
Postnatal morbidities in the prolonged and short latency groups
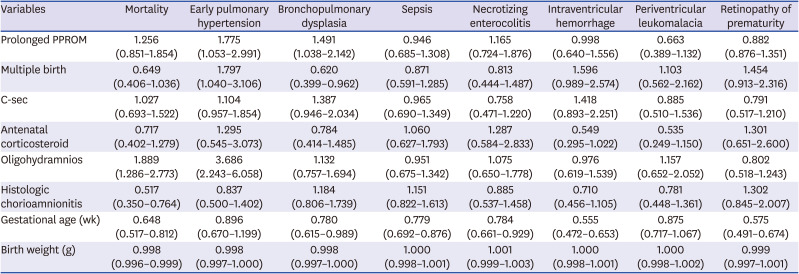
As shown in Table 3, we analyzed the independent effect of PPROM with prolonged latency on the mortality and morbidity adjusted to significant prenatal factors using multivariate models. Although the prolonged latency group was not associated with mortality during hospitalization, the early pulmonary hypertension and BPD rates had increased by 1.8 and 1.5 times, respectively. However, this group was not associated with high NEC, IVH, PVL, and ROP rates. Meanwhile, oligohydramnios, GA at birth, and birth weight were found to be independent risk factors for mortality, early pulmonary hypertension, and BPD in extremely preterm infants exposed to maternal PPROM. Histologic chorioamnionitis showed a mortality reduced by 0.5 times in extremely preterm infants exposed to PPROM.
Table 3
Multivariate logistic regression analysis of the clinical prenatal factors associated with mortality and morbidities
DISCUSSION
In the present study on neonatal outcomes according to the latent period from membrane rupture to delivery among extremely preterm infants exposed to maternal PPROM, prolonged latency of 7 days or more does not affect survival rate but increases the risk of BPD occurrence.
As maternal and fetal complications in women with previable PPROM remains a concern, providing conservative management to maintain pregnancy in women with previable PPROM has been difficult.1 According to previous studies, 40–50% of women with previable PPROM delivered within 1 week.2831 While it is not clear whether all women with PPROM underwent expectant management in the present study, 50% of extremely preterm infants with PPROM were born within 7 days after membrane rupture. However, extremely preterm infants with latent period less than 24 hours were excluded because it was not clear about a therapeutic option in pregnant women with previable PPROM. For a more accurate analysis, an investigation of obstetric treatments in pregnant women with previable PPROM is necessary.
The latent period from membrane rupture to delivery has been shown to be inversely correlated with GA at membrane rupture.1132 In the present study, a correlation coefficient between the latent period from membrane rupture to delivery and GA at membrane rupture was −0.833 (P < 0.001). In general, an absolute correlation coefficient of > 0.7 among two or more predictors indicates the presence of multicollinearity. Considering a potential problem of multicollinearity, GA at membrane rupture was excluded in the multivariate logistic regression analysis of the present study.
Waters et al.2 reported that the neonatal survival rate after conservatively managed PPROM was about 50%. The survival rates were much improved with expectant management following membrane rupture after 22 weeks' gestation compared with membrane rupture before 22 weeks' gestation.2 According to a recent study,7 the expectant management of previable PPROM between 20 to 23 weeks' gestation was associated with a neonatal survival rate of 49%. In another cohort study of infants exposed to PPROM, which occurred before 24 weeks' gestation and who were treated in a modern NICU, the survival-to-discharge rate was 70%.9 In the present study, the survival rate in the prolonged latency group among extremely preterm infants exposed to maternal PPROM was 71.2%, which seems to be similar to the overall survival rate of extremely preterm infants in South Korea.33 Taken together, prolonged latency of 7 days or more did not appear to increase perinatal or overall mortality during hospitalization among extremely preterm infants exposed to maternal PPROM. This finding was consistent with previous studies in which the mortality rates in infants born following maternal PPROM occurring prior to 25 gestational weeks and lasting for 7 days were not significantly higher than those in infants without maternal PPROM.1920
Chorioamnionitis and oligohydramnios following expectantly managed PPROM during the second trimester of pregnancy are known to be major causes of fetal and neonatal morbidity and mortality.79103435 Clinical chorioamnionitis, often referred to as intra-amniotic infection, is an indication for delivery in accordance with recent guidelines, which is conservatively managed in PPROM with no complications.1 The incidence of histologic chorioamnionitis is directly related to the latent period.36 The consequences of chorioamnionitis also affect multiple organ systems in fetuses and neonates, resulting in conditions such as BPD, pulmonary hypertension, cerebral palsy, ROP, and renal injury.36 In the present study, although the histologic chorioamnionitis and oligohydramnios rates in the prolonged latency group were significantly higher than those in the short latency group, histologic chorioamnionitis was not a risk factor for BPD, early pulmonary hypertension, PVL, and ROP in extremely preterm infants exposed to PPROM. Previous other studies have shown that chorioamnionitis negatively affects the short- and long-term outcomes of preterm infants,37 However, in the present study, histologic chorioamnionitis was shown to be a factor reducing mortality in extremely preterm infants exposed to maternal PPROM. The possibility of influencing statistical results due to missing data (11%) for histologic chorioamnionitis as well as the different target study group only confined to PPROM cases in the present study might affect the results. Further additional study is needed for the clarification of this disparity.
Meanwhile, oligohydramnios was shown to be a risk factor for early pulmonary hypertension, BPD, and mortality during hospitalization. Pulmonary hypoplasia, which is associated with fetal lung compression and oligohydramnios, is a serious complication of expectant management following previable PPROM, and mortality from this condition ranges between 50–100%.141516 The factors contributing to the development of pulmonary hypoplasia include the GA at membrane rupture, latent period from membrane rupture to delivery, and residual amniotic fluid volume.1838 In a recent cohort of infants delivered following PPROM, which occurred before 24 weeks' gestation, and treated with modern neonatal intensive care including high-frequency ventilation and nitric oxide, the survival-to-discharge rate was 90%.9 As there was no clinical information regarding pulmonary hypoplasia in the KNN database, we included early pulmonary hypertension in our comparison, which is an important manifestation in cases of pulmonary hypoplasia after birth. According to the multivariate logistic regression analysis adjusted to other prenatal factors that we performed, prolonged latency of 7 days or more was an independent risk factor for early pulmonary hypertension and BPD among extremely preterm infants exposed to maternal PPROM. This is consistent with the findings that early pulmonary hypertension and BPD rates in VLBWIs born following maternal PPROM occurring prior to 25 gestational weeks and lasting for 7 days were significantly higher than those in infants without maternal PPROM.20
Since the association between neonatal sepsis and the duration of membrane rupture was first reported in 1963,39 PPROM with prolonged latency has been considered an independent risk factor for neonatal sepsis. However, studies have found conflicting evidence regarding this association.40414243 In the present study, there was no difference between the two groups in the incidence of blood culture-proven neonatal sepsis during hospitalization.
The strength of this study is that it has a prospective, nationwide, population-based design, which included extremely preterm infants who had received active resuscitation at delivery. However, the lack of available data on the induction of labor and fetal death in women with previable PPROM and comfort care without active resuscitation in the delivery room appears to be a major limitation of this study. Although several hospitals collected all data, including those of mortality in the delivery room, there is a possibility that cases of mortality in the delivery room may have been missed, thereby causing an underestimation of the mortality in the present study. In addition, it was not known whether pregnant women with PPROM underwent immediate delivery or were given expectant management. Although each institution's willingness to use expectant management in women with previable PPROM was not clear, there was no difference in survival rates between the prolonged and short latency groups. On the other hand, PPROM with prolonged latency was shown to be an independent risk factor for early pulmonary hypertension and BPD in extremely preterm infants exposed to maternal PPROM. Although the purpose of the present study is to compare neonatal outcomes between the prolonged and short latency groups among extremely preterm infants exposed to maternal PPROM, a dichotomous variable of the latent period from membrane rupture to delivery may not be suitable. Further studies will be needed to compare neonatal outcomes with a continuous variable not categorical for the latent period.
In conclusion, in accordance with expectant management in women with previable PPROM, prolonged latency of 7 days or more does not affect survival rate but increases the risk of BPD occurrence among extremely preterm infants exposed to maternal PPROM. These findings may be helpful to medical staff preparing to implement more aggressive neonatal intensive care if an extremely preterm infant exposed to maternal PPROM with prolonged latency is delivered quickly.
 XML Download
XML Download