

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Gastric cancer is one of the most important cancers in terms of global incidence and cancer-related deaths.1 In recent years, the overall outcome of gastric cancer has improved owing to increases in early detection by health screening programs and improvements in treatment modalities.2345 The primary treatment for gastric cancer is curative R0 resection, but the clinical outcomes of radical gastrectomy with lymphadenectomy in patients with gastric cancer are occasionally poor due to tumor recurrence.6 As most cases of gastric tumor recurrence arise within 5 years after curative R0 resection,78 timely detection and resection of locoregional recurrences in the remnant gastric mucosa may be helpful in improving oncological outcomes.7910
Regular endoscopic surveillance may be useful for early detection of locoregional recurrence in the remnant gastric mucosa.1112 However, there is no remnant gastric mucosa after total gastrectomy (TG). Also, distant and/or peritoneal recurrences are more common than locoregional recurrence, and the prognosis for recurrent gastric cancer is poor despite treatment.7131415 Thus, it is controversial whether early detection of recurrence significantly prolongs overall survival, and there is no consensus on the strategies of follow-up period and methods, which currently rely on cohort and expert consensus rather than empirical data.1617181920 Specifically, while there is no definite evidence on the clinical benefit of follow-up endoscopic surveillance after TG in terms of oncologic outcomes and detecting postoperative adverse events,1521 annual follow-up endoscopic surveillance is performed in many clinical settings.
Therefore, we investigated the benefit of endoscopic surveillance in oncologic outcomes and detecting postoperative adverse events after TG for gastric cancer.
Go to : 
METHODS
Patients
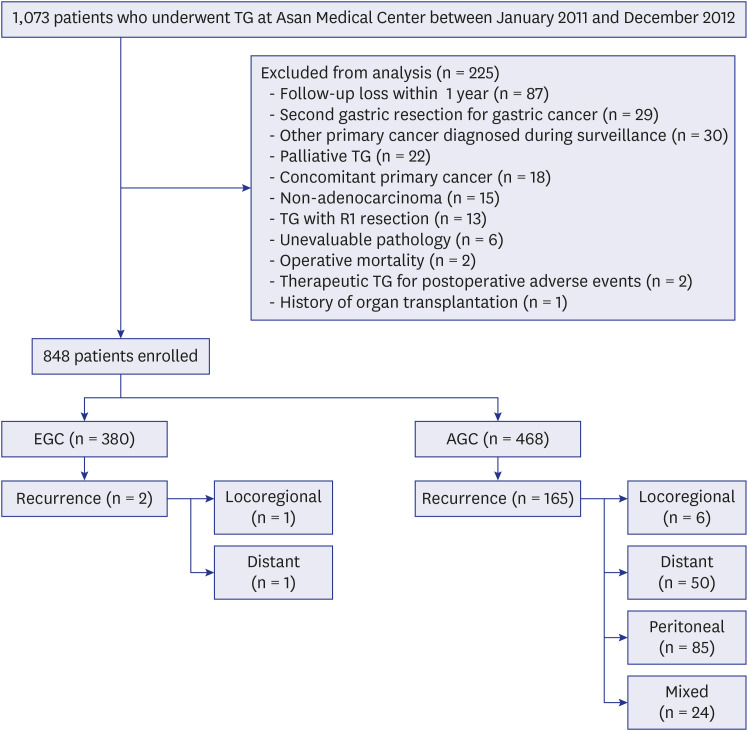
We reviewed the medical records of all patients who underwent TG for gastric cancer between January 2011 and December 2012 at Asan Medical Center (Seoul, Korea). Of them, we analyzed 848 patients who also underwent surveillance every 6–12 months with regular endoscopy and abdominopelvic computed tomography (CT) with contrast after TG with R0 resection. All patients were observed until the detection of tumor recurrence or the last follow-up date of March 31, 2019. Gastric cancers were staged according to the 7th edition of the American Joint Committee on Cancer tumor node metastasis (TMN) classification.22 The tumors were classified into two types based on their histology-differentiated (well or moderately differentiated adenocarcinoma and papillary adenocarcinoma) and undifferentiated (poorly differentiated adenocarcinoma, signet ring cell, and mucinous adenocarcinoma). Patients were excluded according to the following criteria: follow-up loss within 1 year, second gastric resection for gastric cancer, other primary cancer diagnosed during surveillance, palliative TG, concomitant primary cancer, non-adenocarcinoma, TG with R1 resection, unevaluable pathology, operative mortality, therapeutic TG for postoperative adverse events, or history of organ transplantation (Fig. 1).
Patterns of tumor recurrence
The patterns of tumor recurrence were categorized as locoregional, distant, peritoneal, and mixed.1015 Locoregional recurrence included endoscopically accessible tumor recurrence (at the anastomotic site or within an intestinal loop) and endoscopically inaccessible tumor recurrence (dominant masses in the gastric bed or regional gastric lymph nodes). Distant recurrences were in specific organ sites or distant lymph nodes including para-aortic lymph nodes. Peritoneal recurrences included peritoneal seeding nodules on abdominopelvic CT and Krukenberg tumors. Mixed recurrences were defined as multiple recurrent sites at the initial recurrence episode.
Definition of benign stricture on esophagojejunal anastomotic area
We performed an endoscopic study for evaluating benign stricture on esophagojejunal (E-J) anastomotic area and used an endoscope with a maximal outer diameter of 9.8 mm (GIF-H260, Olympus Corp, Tokyo, Japan). We defined benign stricture on E-J anastomotic area as a narrowing without endoscopic passage, or with significant resistance for passage of endoscope, or with impacted food requiring endoscopic intervention in the esophagus.
Statistics
Categorical data were analyzed using the χ2 test or Fisher's exact test as appropriate. Numerical data were analyzed using the Student's t-test. All statistical analyses were performed using the SPSS Statistics for Windows, version 18.0 (SPSS Inc., Chicago, IL, USA). P values < 0.05 were considered statistically significant.
Ethics statement
The Institutional Review Board of Asan Medical Center approved the study (IRB No. 2018-0561). Due to the retrospective study design, written informed consent was not obtained from participants. The IRB of our institution waived the need for informed consent based on the non-invasive and anonymized nature of this study. This study was conducted in accordance with institutional ethical guidelines and the Declaration of Helsinki.
Go to :
RESULTS
Baseline characteristics of patients
The clinicopathological characteristics of the 848 patients are summarized in Table 1. Median age of the patients was 56 years (range, 18–79), and 549 (64.8%) were male. A total of 380 (44.8%) patients had early gastric cancer (EGC) and 468 (55.2%) had advanced gastric cancer (AGC). In 380 patients with EGC, 38 (10.0%) had multiple EGCs and the maximal number of synchronous EGCs in a patient was 6. In 468 patients with AGC, 17 (3.6%) patients had 2 synchronous gastric cancers and 7 (1.5%) patients had 3 synchronous gastric cancers. Eight patients who had gastric cancers in the lower third of the stomach received TG due to adhesion around the upper third of the stomach or severe metaplastic changes in the entire stomach.

Table 1
Baseline characteristics of the 848 patients who received TG for gastric cancer (n = 848)
Data are the number of patients (%) unless otherwise noted.
TG = total gastrectomy, CT = computed tomography.
![]()
Follow-up and patterns of tumor recurrence
The distribution of patients according to the follow-up period and the patterns of tumor recurrence over time are shown in Fig. 2. Median time to follow-up was 58 months for both abdominopelvic CT (range, 1–96) and endoscopy (range, 3–96). In patients without tumor recurrence, 115 was followed up for less than 5 years; among these patients, 67 had EGC and 48 had AGC.
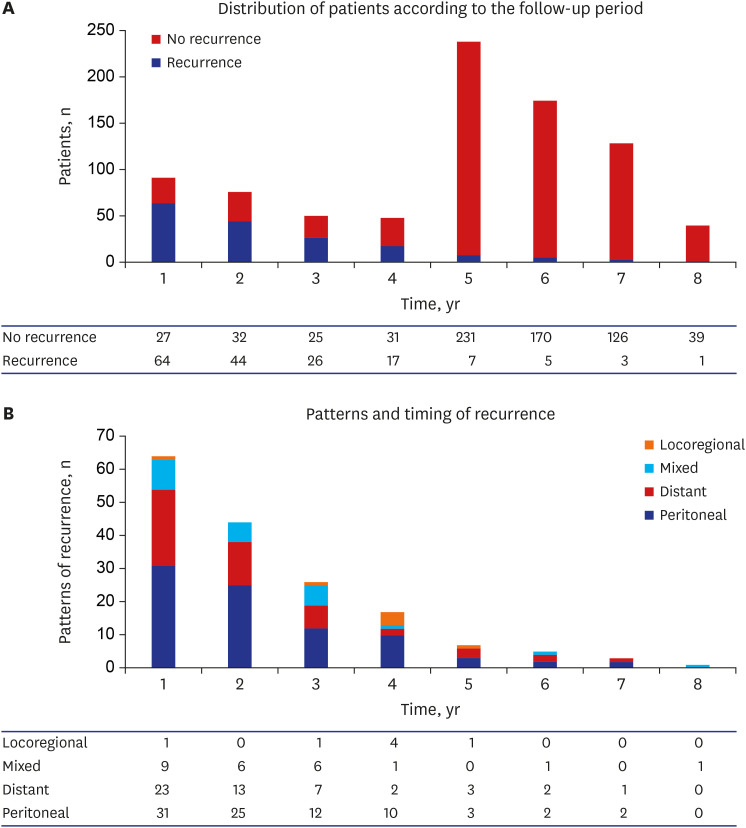
A total of 167 (19.7%) patients showed tumor recurrence. In 167 patients with tumor recurrence, 165 (98.8%) had AGC and only 2 (1.2%) had EGC. In 380 patients with EGC, tumor recurrence was very rare (0.5%). Median time of recurrence was 17 months (range, 1–88). Most (80.2%) of the tumor recurrence was confirmed within 3 years.
Two (1.2%) patients had EGCs: one of them showed locoregional recurrence in the E-J anastomotic area on endoscopy and abdominopelvic CT at 44 months after TG, and the other patient showed multiple bone metastases on abdominopelvic CT at 54 months after TG. The other 165 patients had AGCs, and the most common pattern of recurrence was peritoneal recurrence (n = 85, 51.5%). Distant recurrence, mixed recurrence, and locoregional recurrence occurred in 50 (30.3%), 24 (14.5%), and 6 cases (3.6%), respectively. In the mixed recurrence cases, the majority (n = 19, 79.2%) were both peritoneal and distant recurrence. Twelve (7.2%) of the 167 patients were confirmed to have tumor recurrence after 5 years. All recurrence cases were detected by abdominopelvic CT or other radiologic examinations.
Features of locoregional recurrence and the role of endoscopy
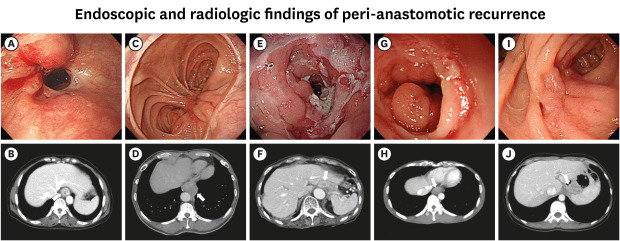
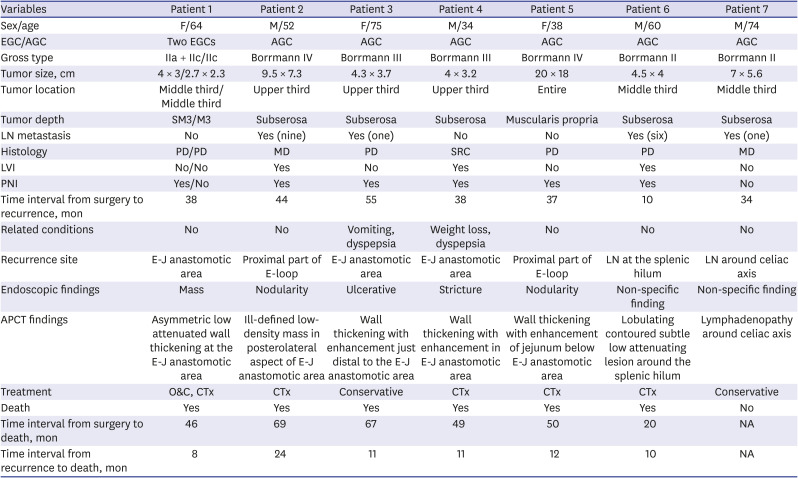
Locoregional recurrence was confirmed in 7 (0.8%) patients (Table 2). Of 7 locoregional recurrences, asymptomatic recurrences were 5 and symptomatic recurrences were 2. TG was performed in one of those patients for two synchronous EGCs and the other six patients for AGCs. Peri-anastomotic recurrence was found in five patients and recurrence in regional gastric lymph nodes in two patients. Importantly, all cases of peri-anastomotic recurrence were detected by both endoscopy and abdominopelvic CT (Fig. 3), and two cases of recurrence in regional lymph nodes were detected only by abdominopelvic CT. One case was considered to be clinically resectable at the initial episode of recurrence, but was found to be unresectable during laparotomy because of diaphragmatic invasion of the recurred tumor. Therefore, all cases of peri-anastomotic recurrence were unresectable in multidisciplinary discussion; the median survival time after recurrence was 12 months (range, 8–24 months). Two patients (patients #3 and #7 in Table 2) received conservative management without chemotherapy due to old age and poor performance status. The median recurrence-free survival time of patients with locoregional recurrence was 38 months (range, 10–55). The median recurrence-free survival time of cases with peri-anastomotic recurrence was longer than that of cases with other patterns of recurrence (38 vs. 16 months, P = 0.087).
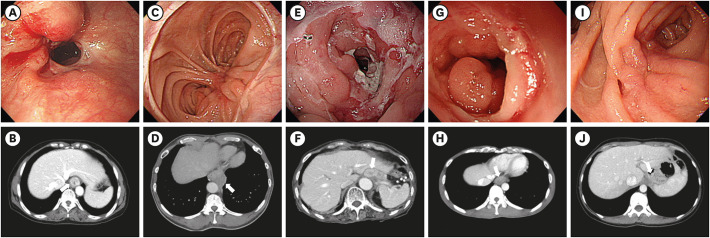 | Fig. 3Endoscopic and contrast abdominopelvic CT findings of peri-anastomotic recurrence. The photos are each from patient #1 through patient #5 (left to right) in Table 2. (A) Mass of irregular shape around the anastomotic site. (B) Asymmetric low attenuated wall thickening at the anastomotic site. (C) Irregular nodularity with hyperemia on proximal part of the efferent loop. (D) Ill-defined low-density mass in the posterolateral aspect of the anastomotic site. (E) Irregular ulcerative lesion with luminal narrowing at the anastomotic site. (F) Wall thickening with enhancement just distal to the E-J anastomotic area. (G) Stricture of the anastomotic site with irregular mucosal nodularity. (H) Wall thickening with enhancement in the anastomotic site. (I) Irregular nodularity with hyperemia on the proximal part of the efferent loop. (J) Wall thickening with an enhancement of jejunum below the anastomotic site.CT = computed tomography, E-J = esophagojejunal.
|
Table 2
Summary of locoregional recurrences
EGC = early gastric cancer, AGC = advanced gastric cancer, SM = submucosa, M = mucosa, LN = lymph node, PD = poorly differentiate, MD = moderate differentiated, SRC = signet ring cell, LVI = lymphovascular invasion, PNI = perineural invasion, E-J = esophagojejunal, E-loop = efferent loop, APCT = abdominopelvic computed tomography, O&C = open and closure, CTx = chemotherapy, NA = not applicable.
![]()
Postoperative adverse events based on endoscopic and radiologic findings
A total of 23 postoperative adverse events were observed in 21 (2.5%) patients (Table 3): 17 events were detected only by radiologic study, 3 were detected only by endoscopic study, and 3 were detected by both endoscopic and radiologic studies. Three cases of benign stricture in the anastomotic site were detected only by endoscopic evaluation. The clinical and endoscopic features are summarized in Table 4. One patient who received surgical repair for anastomotic leakage at 10 days after TG underwent endoscopic removal of impacted food at 70 months after TG. Additional treatments for benign stricture were not recommended. Because even though the anastomotic site was narrow, endoscopic passage through the narrowing anastomotic site was possible and the patient did not complain of dysphagia except for the endoscopic intervention of impacted food in the esophagus. Another patient had the anastomotic site narrowing with endoscopic passage. Interventional treatments were not recommended because of the absence of dysphagia. The other patient had severe anastomotic site narrowing without endoscopic passage and had strangulation in the small bowel. The patient had received surgical treatment for benign stricture and strangulation in the small bowel. Anastomotic leakage and leakage at blind end of the jejunum in three patients were detected by radiologic study and treated by endoscopic closure with a clip. Anastomotic leakage in one patient was detected by radiologic study and treated by surgical repair.
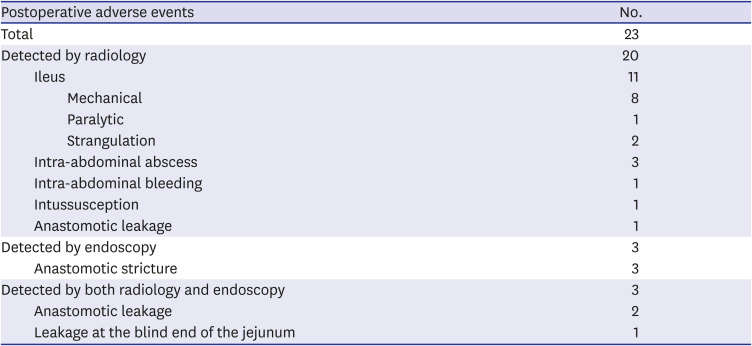
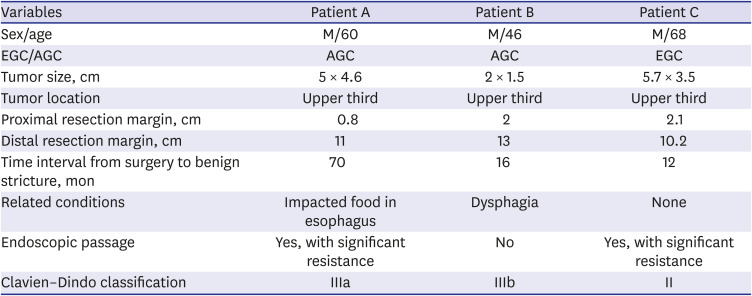
Table 3
Endoscopic and radiologic findings of postoperative adverse events
![]()
Table 4
Clinical and endoscopic features of benign stricture on esophagojejunal anastomotic area
![]()
Go to :
DISCUSSION
In our study, 848 patients received total gastrectomy with R0 resection for gastric cancer and only seven (0.8%) of them had locoregional recurrence. Specifically, five cases (0.5%) of peri-anastomotic recurrence were detected by both endoscopy and abdominopelvic CT, and two cases of recurrence in regional lymph nodes were detected only by abdominopelvic CT. The majority (87%) of the postoperative adverse events were detected by radiologic examinations, and only 3 events of benign strictures were detected only by endoscopy.
Many guidelines for gastric cancer recommended endoscopic surveillance for detecting local recurrence after gastrectomy. In Japanese guidelines, biannual endoscopic surveillance is recommended for detecting recurrence from the first year after gastrectomy.23 Similarly, Chinese guidelines recommend annual endoscopic surveillance after gastrectomy regardless of EGC or AGC.24 In Italian guidelines, a follow-up strategy based on the risk of recurrence is recommended including annual endoscopy except at 48 months.2526 Nevertheless, the guidelines also mention that the recommendation for routine endoscopic surveillance lacks sufficient empirical evidence.232425 The Korean guidelines for gastric cancer do not specifically mention the need for surveillance programs after gastrectomy27; however, survey results from the Korean Gastric Cancer Association showed that physicians perform regular surveillance every 6–12 months and that endoscopy is frequently performed.28
However, many guidelines for gastric cancer recommended endoscopic surveillance after gastrectomy regardless of gastrectomy types including TG and subtotal gastrectomy (STG). It is a need to distinguish between TG and STG, because of the remnant gastric mucosa. Endoscopic surveillance for STG can detect metachronous gastric cancer in remnant gastric mucosa not only locoregional recurrence. Han et al.29 recommended annual endoscopic surveillance for remnant gastric cancer up to 20 years after STG. Also, several studies reported that endoscopic surveillance was significantly helpful in detecting locoregional recurrence including metachronous gastric cancer in remnant gastric mucosa and associated with improvement of oncologic outcome after secondary gastric resection or endoscopic submucosal dissection.91112303132333435 However, there is no remnant gastric mucosa after TG. In our study, peri-anastomotic recurrence were rare (0.5%) and detected by both endoscopy and abdominopelvic CT. Endoscopic surveillance after TG may be considered optional according to the capacities of each clinical setting.
Recent studies reported low incidences (1.6%–1.8%) of locoregional recurrence after TG for gastric cancer due to the absence of remnant gastric mucosa.3637 Also, recurred tumors were frequently unresectable and associated with poor prognosis.153438 In our results, only 7 out of 848 (0.8%) patients who underwent TG with R0 resection for gastric cancer cases were confirmed to have locoregional recurrence. All cases of locoregional recurrence were uncurable due to unresectable or poor performance status.
All seven cases of locoregional recurrence including peri-anastomotic area and regional gastric lymph node were detected by abdominopelvic CT; in contrast, endoscopy could not detect the two cases of recurrence in regional lymph nodes. Also, radiologic examinations including abdominopelvic CT successfully detected all recurrence cases. Collectively speaking, regular endoscopic surveillance had limited benefit over radiologic study for detecting locoregional recurrence after TG for gastric cancer.
Peri-anastomotic recurrence is assumed to occur from submucosal or subserosal lymphatics spread of cancer cells or the implantation of exfoliated cancer cells.394041 Therefore, peri-anastomotic recurrence may be due to tumor invasion from the outer layer of the lumen. Abnormality of the inner layer of the lumen can only be detected by endoscopy. In our results, radiologic findings of peri-anastomotic recurrence were bowel wall thickening or mass. Therefore, endoscopy may be limited in the early detection of peri-anastomotic recurrence.
The other role of regular endoscopic surveillance after TG is to detect postoperative adverse events, especially anastomotic strictures. Lee et al.15 reported that the incidence of benign stricture at anastomosis site was 7% and suggested that routine follow-up endoscopy after TG for gastric cancer was useful in the early detection and treatment for benign strictures. In more recent studies, the incidence of anastomotic stricture after TG for gastric cancer was reported to be as low as 0.9%–2.0%.4243 In our study, only 3 out of 848 (0.4%) patients had anastomotic site narrowing during endoscopy. Only one patient underwent endoscopic removal of food stasis. Because endoscopy passage through the narrowing anastomotic site was possible, no additional endoscopic intervention was necessary. Thus, in our data, the role of regular endoscopic surveillance for postoperative adverse events was also largely inconsequential due to the low incidence and severity.
Some methodological limitations of this study should be noted. First of all, our study design is retrospective and observational in nature. However, it is difficult to conduct a randomized controlled trial on postoperative surveillance programs because of the follow-up period, number of patients, and ethical issues. Therefore, many reviews for surveillance after gastrectomy for gastric cancer were based on retrospective observational studies.444546 To compensate for the innate weakness of such study design, we analyzed a large number of patients who were treated within a relatively recent period and followed for over 5 years. Whereas recent studies on a similar topic1521 each studied a total of 212 and 70 patients, we analyzed a total of 380 EGC patients. The second limitation is the rarity of locoregional recurrence. We tried to determine the risk factors of locoregional recurrence, especially peri-anastomotic recurrence, because such patients may benefit from early detection of peri-anastomotic recurrence and additional surgical treatment. However, locoregional recurrence was rare (0.8%) and statistical analysis was not feasible. The third limitation is the absence of information about adverse events of endoscopy and radiologic study. In many guidelines, regular endoscopic and radiologic surveillance will be performed 3–5 times per patient for 5 years. Major adverse events of endoscopy and radiologic study are rare, but it can be life-threatening.4748 Therefore, the necessity of regular surveillance with endoscopy and radiologic study will be considered with possibilities of endoscopic and radiologic study induced adverse events. Further studies are needed about the clinical benefit and risk of regular surveillance. Finally, we did not consider the types of TG based on open and laparoscopy. Because laparoscopic TG (LTG) was a technical difficulty, especially the reconstruction of the E-J, it is a clinically important concern for surgical and oncologic outcomes. The recent studies reported that the surgical and oncologic outcomes of LTG were feasible and safe compared with open TG.4243 A few meta-analyses for outcomes based on surgical types reported that the short-term outcomes were similar or feasible in LTG compared with open TG.4950 However, the long-term outcomes were inconclusive, because these studies were enrolled in a relatively small number and single-center study. The long-term outcomes including locoregional recurrence and benign stricture in the anastomotic site are important to consider endoscopic surveillance. So, further studies with large, multi-center study are needed for these concerns.
In conclusion, locoregional recurrence and anastomotic strictures after TG were rare, and endoscopic surveillance after TG with R0 resection for gastric cancer did not show a significant benefit over abdominopelvic CT in detecting tumor recurrence or postoperative adverse events. Routine endoscopic surveillance after TG may be considered optional and performed according to the capacities of each clinical setting.
Go to :
 XML Download
XML Download