

 PDF
PDF Citation
Citation Print
Print



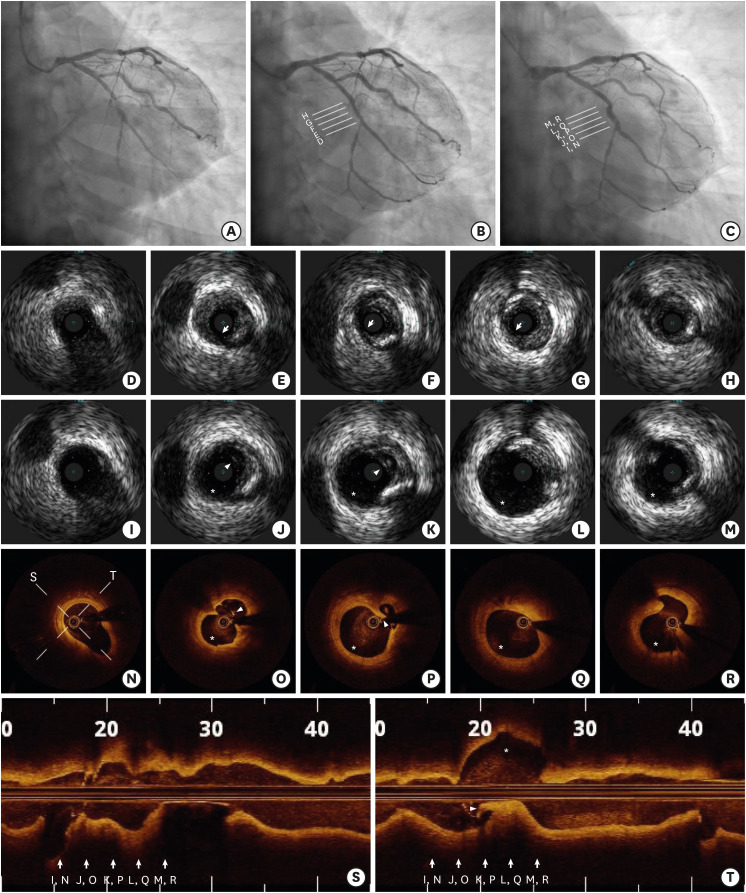
A 58-year-old man with hypertension, hypercholesterolemia and history of smoking was admitted with stable angina. His treadmill exercise test was positive. Coronary angiography showed a sub-total occlusion in the mid left circumflex artery with thrombolysis in myocardial infarction (TIMI) flow grade 2 (Figure 1A). The patient declined stent implantation but agreed to treatment with drug-coated balloon (DCB). The lesion was carefully assessed and informed consent was obtained.
The lesion was pre-dilated with a 1.5 mm balloon, followed by a 2.5 mm scoring balloon, before being treated with a 2.5×26 mm DCB inflated at 10 atm for 60 seconds. The final angiogram showed no residual stenosis and TIMI flow grade 3 (Figure 1B). A follow-up coronary angiogram at 12-month showed positive remodeling and a fusiform aneurysm at the site of the treated lesion with DCB. Intravascular ultrasound (IVUS) imaging showed that the aneurysm was formed (Figure 1, asterisks) at the site of a coronary dissection (Figure 1, arrows) observed immediately after DCB treatment. He remains symptom free during the 13-months after DCB treatment.
Coronary artery aneurysm formation has been reported after percutaneous transluminal coronary angioplasty (PTCA) with a frequency of 4% to 5%.1),2) Although dissection is considered to be one of the causes of aneurysms after PTCA, the mechanism of aneurysm formation after DCB treatment has not yet been identified. We have demonstrated the aneurysm formation through serial IVUS and optical coherence tomography after DCB treatment. More research is needed on the pathophysiology of the occurrence of aneurysms in DCB-only treated lesion, and the relationship between these aneurysms and clinical outcomes through long-term follow-up.
 XML Download
XML Download