

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cigarette smoking is globally recognized as a risk factor for the development of coronary artery disease (CAD), such as acute myocardial infarction (AMI), and most cancers, including lung cancer.1)2)3)4) Smokers with CAD have increased risk of adverse cardiovascular events and death worldwide.3)5) Cigarette smoking and its detrimental health effects also increase the economic burden globally. Interestingly, despite the detrimental effects of cigarette smoking on cardiovascular health, some studies have suggested that a “smoker's paradox” exists. Smoker's paradox suggests that smokers with CAD, especially AMI, may be the same as or better off than nonsmokers.6)7) However, such reports could have a negative public health impacts. In fact, previous surveys have reported that more than one-third of smokers disagreed that smoking was associated with the occurrence of smoking-related diseases such as lung cancer and CAD.8)9) Previous studies have investigated the effects of smoking on clinical outcomes in patients with CAD.10)11)12)13)14)15) Although some studies have still reported smoker's paradox,14)16) numerous recent studies have shown similar or higher mortality in smokers compared to nonsmokers.10)11)12)13)15) These discrepancies in study results are likely due to differences in study characteristics and covariate selection. It has been reported that smoker's paradox existed only in the thrombolysis era,17)18) but it still remains unclear whether smoker's paradox exists in the percutaneous coronary intervention (PCI) era.
Smoking is involved in the development of most cancers, especially lung cancer, which is the most closely linked to smoking among all smoking-related diseases.4) Unfortunately, the impact of smoking on cancer incidence in patients with AMI has not been reported. Therefore, the present study aimed to investigate the impact of smoking status on 5-year clinical outcomes, especially cancer incidence, in patients with AMI undergoing PCI.
METHODS
Study population
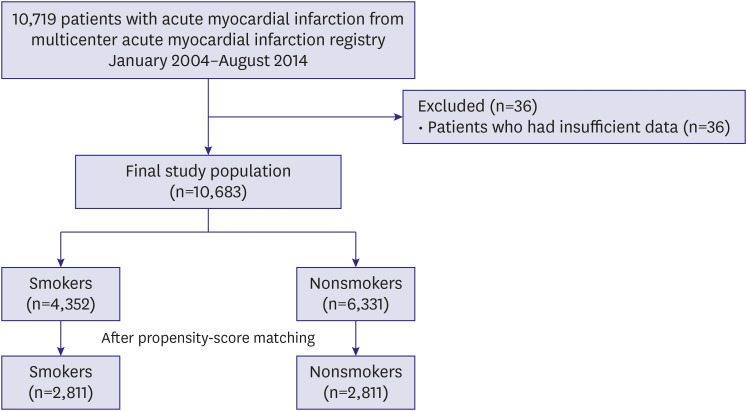
The CardiOvascular Risk and idEntificAtion of potential high-risk population in AMI (COREA-AMI) registry was designed to evaluate the real-world long-term clinical outcomes in all patients with AMI. The COREA-AMI I registry was already reported and included patients with AMI who underwent PCI from January 2004 to December 2009. The COREA-AMI II registry included additional patients from January 2010 to August 2014. The current registry had updated clinical and angiographic parameters and evaluated long-term clinical follow-up data as long as possible by 2019. Included patients were over 20 years old and were treated with PCI. Patients who had insufficient data about smoking status were excluded (Figure 1). The study was conducted in compliance with the Declaration of Helsinki (2013), regarding investigations in humans. The study protocol was approved by the Institutional Review Board at participating centers. This registry has been registered on ClinicalTrials.gov (study ID: NCT02806102).
Study definition
AMI was diagnosed by detecting elevated cardiac biomarkers that were at least 1 value above the 99th percentile upper reference limit with temporal rise and fall and at least 1 of the following indications: symptoms of ischemia, new or presumed new significant ST-segment-T wave changes or new left bundle branch block, development of pathological Q waves in electrocardiography, imaging evidence of new viable myocardium loss or new regional wall motion abnormality, or intracoronary thrombus identified by angiography.19) The clinical presentation was divided into 2 groups according to the electrocardiography findings: ST-segment elevation myocardial infarction (STEMI) and non-STEMI (NSTEMI). Typical ST-segment elevation in 2 contiguous leads and atypical electrocardiographic presentations, such as bundle branch block, isolated posterior wall myocardial infarction (MI), or ST-segment elevation in lead augmented vector right, with appropriate clinical and angiographic findings indicated STEMI, while the other cases were regarded as NSTEMI.
Current smoking status at index admission was used to stratify the patient groups. Smokers were defined as patients who reported having smoked cigarettes within 3 months of index admission.12) Nonsmokers included patients who have never smoked and ex-smokers.
Study endpoints
The primary endpoint was major adverse cardiovascular events (MACE), including cardiac death, nonfatal MI, stroke, and any revascularization during the 5-year follow-up. Secondary endpoints were all-cause death, cardiac death, nonfatal MI, stroke, any revascularization, malignancy, and lung cancer. Patients' follow-up data, including survival data and clinical event data, were collected through March 31, 2019, via hospital chart reviews and telephone interviews of patients that were conducted by trained reviewers who were blinded to the study results. In addition, the mortality data were verified by the database of the National Health Insurance Corporation, Korea, using a unique personal identification number.
Treatment and data collection
Coronary angiography and other interventions were performed according to standard guidelines. Aspirin- or P2Y12 inhibitor-native patients received loading doses of aspirin and a loading dose of clopidogrel, ticagrelor, or prasugrel. The strategy for revascularization, techniques, selection of devices, and adjunctive antithrombotic therapy were determined by the operator.20)21) After the intervention, patients were recommended to receive optimal pharmacological therapy, including statins, beta-blockers, or renin-angiotensin system inhibitors, according to standard guidelines.22)23)
All data were collected on a web-based system after eliminating personal information. Independent reviewers and interventional cardiologists assessed angiographic and procedural data, while independent research personnel collected baseline clinical, laboratory and medication data. Clinical events and outcome data were assessed with electrical medical records and telephone conversations. All adverse clinical events of interest were confirmed centrally by the committee at the Cardiovascular Center of Seoul St. Mary's Hospital, Seoul, Republic of Korea. Validation for mortality was performed on the basis of disqualification from the National Health Insurance Service, which is the single government-managed insurance and covers almost all of the nation's population. The final dataset was handled by independent statisticians of the Clinical Research Coordinating Center and sealed with a code by the Clinical Research Associate.
Statistical analysis
Continuous variables are expressed as the mean±standard deviation; they were analyzed by an independent sample t-test or the Mann-Whitney U test. Categorical variables are presented as percentages or rates; they were analyzed by the χ2 test or Fisher's exact test. Kaplan-Meier curves were used to analyze the overall survival rate of patients. A comparison of clinical outcomes between groups was performed with the log-rank test. Cox proportional hazard models were applied to analyze the hazard ratio (HR) and 95% confidence interval (CI) for clinical outcomes. To reduce the impact of bias and potential confounding factors in an observational study, a propensity score analysis was also performed to adjust for potential confounders using a logistic regression model. The covariates in the propensity score analysis were as follows: age, sex, body mass index, Killip class, systolic blood pressure, diastolic blood pressure, heart rate, hypertension, diabetes mellitus, dyslipidemia, smoking, chronic kidney disease, stroke, prior PCI, prior MI, prior coronary artery bypass graft, malignancy, chronic obstructive lung disease, clinical presentation (STEMI vs. NSTEMI), left ventricular ejection fraction, total cholesterol, triglyceride, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, hemoglobin, estimated glomerular filtration rate (eGFR), high sensitivity C-reactive protein (hs-CRP), hemoglobin A1c, multivessel disease, culprit lesion, stent generation, restenosis, chronic total occlusion, bifurcation, the use of intravascular imaging number of total stents, mean diameter of stents, total length of stents, aspirin, clopidogrel, potent P2Y12 inhibitors (prasugrel or ticagrelor), statins, beta-blockers, and angiotensin converting enzyme inhibitors/angiotensin receptor blockers. According to the propensity score, patients were selected by 1:1 matching without replacement using the nearest neighbor method. A caliper width of 0.2 standardized differences was used for matching. All analyses were 2-tailed, and p<0.05 was considered statistically significant. All statistical analyses were performed using SPSS 20.0 statistical software (SPSS Inc., Chicago, IL, USA) and R version 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Baseline clinical and procedural characteristics
Among 10,719 patients, a total of 10,683 patients with AMI were included in the final analysis, of whom 4,352 (40.7%) were current smokers and 6,331 (59.3%) were nonsmokers. The mean age of overall patients was 63.7±12.8 years old, and 71.4% of the patients were men. Among them, 5,827 patients (54.5%) presented with STEMI. Baseline clinical and procedural characteristics are listed in Tables 1 and 2. Smokers were younger than nonsmokers. The frequency of females, hypertension, diabetes mellitus, chronic kidney disease, stroke, cancer, and NSTEMI was higher in nonsmokers. Smokers had lower levels of hs-CRP and higher levels of eGFR than nonsmokers. In nonsmokers, multivessel disease, left anterior descending artery as the culprit lesion, and restenosis were more frequent. Nonsmokers had a smaller mean stent diameter and a longer total stent length than smokers. After propensity score matching, there were no differences in baseline clinical and procedural characteristics between the 2 groups (Supplementary Tables 1 and 2).
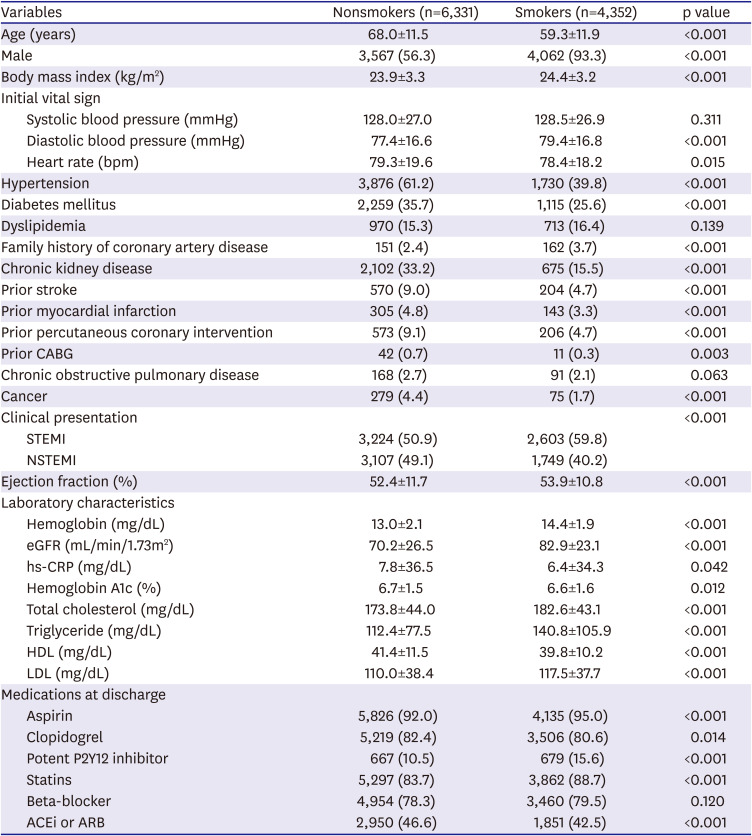
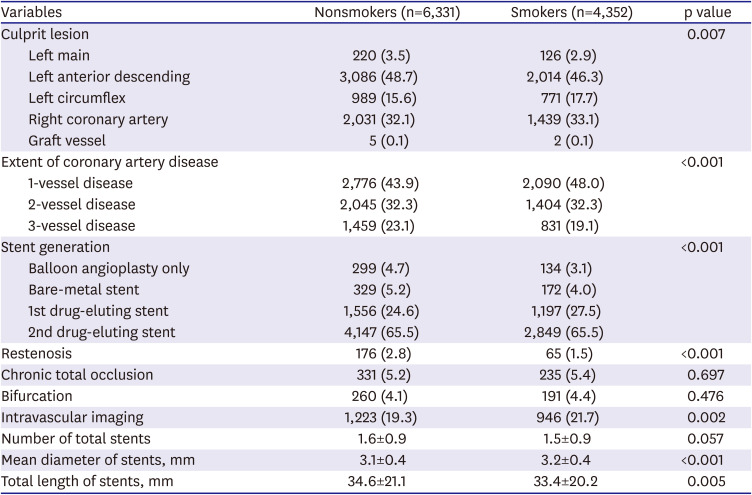
Table 1
Baseline clinical and angiographic characteristics
Data are shown as mean±standard deviation or number (%).
ACEi = angiotensin-converting enzyme inhibitors; ARB = angiotensin receptor blocker; CABG = coronary artery bypass graft; eGFR = estimated glomerular filtration rate; HDL = high-density lipoprotein; hs-CRP = high sensitivity C-reactive protein; LDL = low-density lipoprotein; NSTEMI, non-ST-segment elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction.
![]()
Table 2
Baseline angiographic and procedural characteristics
![]()
Clinical outcomes
In the overall patients, smoking was associated with lower in-hospital mortality (3.7% vs. 6.9%; unadjusted HR, 0.580; 95% CI, 0.489–0.689, p<0.001). After propensity-score matching, there was no significant difference of in-hospital mortality between smokers and nonsmokers (propensity-score matched HR, 0.996; 95% CI, 0.766–1.294; p=0.976). During the 5-year follow-up, MACE occurred in 1,795 patients (18.2%), and 1,586 patients (16.1%) died. The clinical outcomes are presented in Table 3. Figure 2 demonstrates the comparison of HRs for long-term clinical outcomes before and after propensity score matching. In the unadjusted model, the incidences of MACE, all-cause death, cardiac death, MI, and stroke were higher in nonsmokers. After propensity score matching, current smoking was associated with higher MACE, all-cause death, and cardiac death. Furthermore, the incidence of lung cancer was significantly higher in smokers (unadjusted HR, 2.496; 95% CI, 1.468–4.242; p<0.001; propensity-score matched adjusted HR, 2.749; 95% CI, 1.416–5.338; p=0.003). Although smoking was associated with lower risk of MI and stroke in the unadjusted model, there was no significant difference statistically in the risk of MI and stroke between smokers and nonsmokers after propensity-score matching. There were no significant differences in any revascularization, stent thrombosis, and malignancy before or after propensity-score matching between the 2 groups. Figure 3 demonstrates the Kaplan-Meier curves for clinical outcomes after propensity score matching.
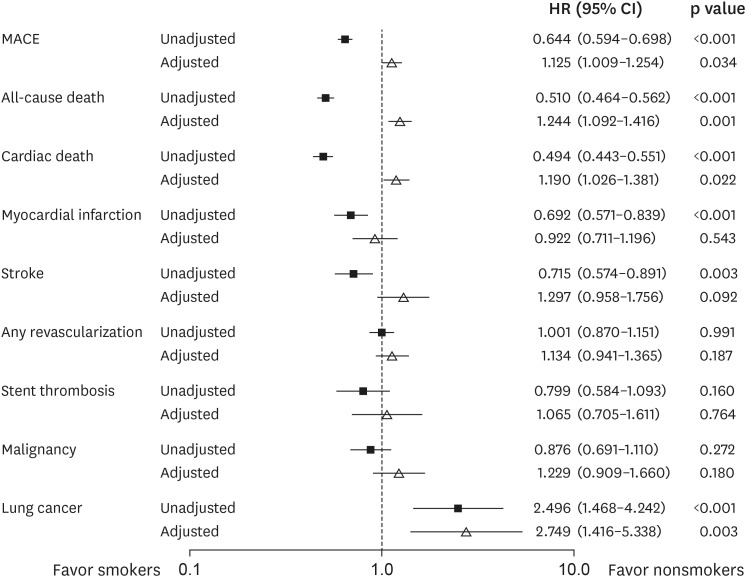
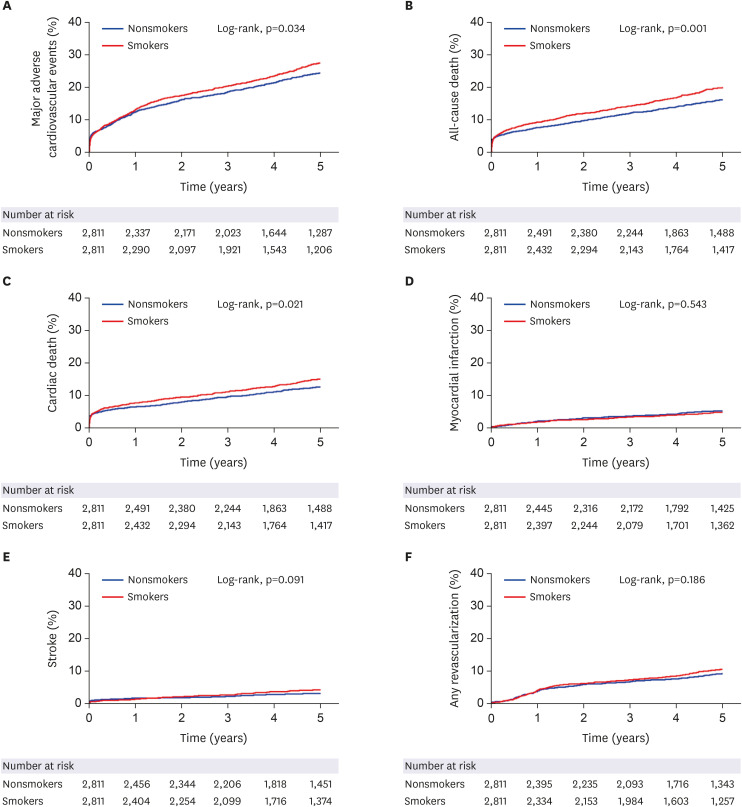
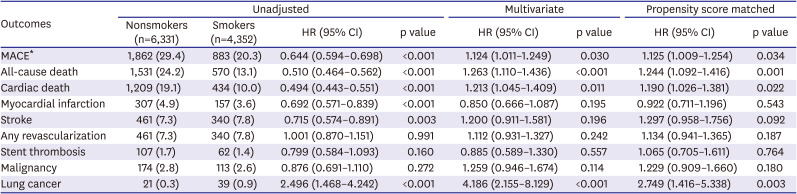
Figure 2
Unadjusted and propensity-score adjusted associations of smoking and long-term clinical outcomes.
CI = confidence interval; HR = hazard ratio; MACE = major adverse cardiovascular events.
![]()
Figure 3
Cumulative incidence rate of (A) major adverse cardiovascular events, (B) all-cause death, (C) cardiac death, (D) myocardial infarction, (E) stroke, and (F) any revascularization among propensity-score matched patients.
![]()
Table 3
Comparison of 5-year clinical outcomes between nonsmokers and smokers
Values are presented as number (%).
CI = confidence interval; HR = hazard ratio; MACE = major adverse cardiovascular events.
*MACE was defined as a composite of cardiac death, myocardial infarction, stroke, and any revascularization.
![]()
Subgroup analysis
For subgroup analyses, we stratified the overall patients by age, sex, and valuable comorbidities. Figure 4 presents a forest plot indicating the MACE as related to various patient or procedural characteristics in the propensity-score matched population. This subgroup analysis revealed an interaction in patients between age (p for interaction=0.034) and diabetes status (p for interaction=0.023). Elderly (HR, 1.250; 95% CI, 1.080–1.446; p=0.003) and nondiabetes (HR, 1.244; 95% CI, 1.084–1.428; p=0.002) had higher rates of MACE in smoker.
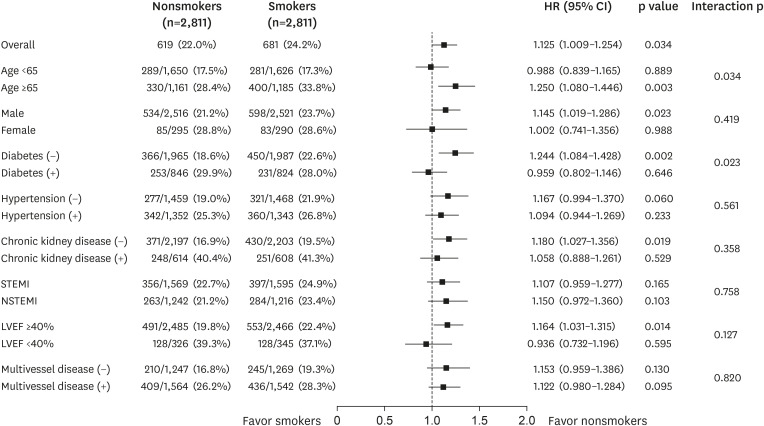
Figure 4
Comparative hazard ratios of major adverse cardiovascular events for subgroups in propensity-score matched patients.
CI = confidence interval; HR = hazard ratio; LVEF = left ventricular ejection fraction; NSTEMI = non-ST-segment elevation myocardial infarction; STEMI = ST-segment elevation myocardial infarction.
![]()
DISCUSSION
In the present study, we have shown in a large, multicenter cohort of patients with AMI that smoking is a strong and independent predictor of 5-year mortality and lung cancer. Smokers were younger than nonsmokers. The incidence of females, NSTEMI, hypertension, diabetes mellitus, prior MI, prior CABG, stroke, chronic kidney disease, and cancer was higher in nonsmokers compared with smokers. In the crude model, smoking was associated with decreased long-term cardiovascular events. However, after propensity-score matching, smokers had a higher risk of MACE, all-cause death, and cardiac death. Furthermore, smokers had a higher risk of lung cancer among patients with AMI.
Several mechanisms can explain the increase in adverse cardiovascular events in AMI patients who smoke. Smokers have higher plasma levels of fibrinogen and increased platelet aggregation, resulting in a hypercoagulability state.24) Smoking also causes coronary vasoconstriction and endothelial dysfunction.25)26) Moreover, smoking contributes to atherosclerosis and plaque progression, leading to LDL and HDL cholesterol changes.2)
In the thrombolytic therapy era, numerous studies reported that smokers were associated with favorable clinical outcomes compared with nonsmokers.17)18) However, recent studies have shown that this hypothesized survival benefit in smokers with CAD no longer exists in the PCI era.10)11)12)13)15)27) Nevertheless, some studies have reported the “smoker's paradox.”14)16) These previous studies have investigated on shorter clinical outcomes compared with our results assessing 5-year clinical outcomes.10)11)12)13) Parasuraman et al.13) collected 12,656 patients with acute coronary syndrome following PCI to assess 30 day and 6 month mortality according to smoking status. Yadav et al.10) investigated the relationship between smoking and 5-year clinical outcomes from an individual patient pooled database, however only approximately 25% of the study population were diagnosed with AMI. In contrast, we conducted a multicenter registry evaluation to investigate clinical outcomes of 10,683 AMI patients based on their smoking status.10) In addition, recent reports suggested that the smoker's paradox was limited to assessing in-hospital mortality only.15) The present study found no significant difference in the risk of in-hospital mortality between smokers and nonsmokers among the propensity-score matched cohort.
In the present study, smokers were significantly younger, predominantly men, and had a lower prevalence of risk factors, including hypertension, diabetes mellitus, chronic kidney disease, and stroke. These baseline differences are consistent with previous reports.27)28) This finding emphasized the fact that smokers are prone to more rapidly developing CAD requiring PCI with plaque rupture and thrombosis. Although smokers had a better prognosis in an unadjusted analysis, after proper adjustment for cardiovascular risk factors, smokers had a higher risk of cardiac death, all-cause death, and developing lung cancer during the 5-year follow-up period. However, smoking did not increase the risk of any revascularization, which was consistent with previous reports.27)29) Our study detected that the rate of MI did not differ between the 2 groups. Although our study included only AMI patients, the incidence of MI and any revascularization was relatively lower than those from the previous meta-analysis.10) The point to note in our study was that we investigated the relationship between smoking status and 5-year clinical outcomes, including MACE and risk of any cancer, in patients with AMI. In our study, the harmful effect of smoking was greatest in patients classified as elderly or nondiabetes. These results emphasize the importance of quitting smoking, especially in elderly and nondiabetic patients. More studies are needed to examine why the harmful effects of smoking are greatest in elderly and nondiabetic patients.
Smoking is involved in the development of most cancers, and lung cancer is the most closely associated with smoking among all smoking-related diseases.4) The impact of smoking on cancer development in AMI patients has not yet been reported. In our study, smoking did not increase the risk of developing other cancers, but it did increase the risk of developing lung cancer in AMI patients. From a public health perspective, the message of our study is that smokers with AMI are at a high risk of death and increased risk of lung cancer, increasing their socioeconomic burden.30)
Our study has several limitations. First, this study was a retrospective cohort study. However, this study had several advantages to minimize the limitations, such as large sample size, homogenous group of AMI patients and statistical adjustments, including propensity score matching. Second, we obtained the information on smoking status only at the time of the index event and not during follow-up. Based on the beneficial effect of smoking cessation, information on smoking status at serial time points would have provided additional useful information.1) Third, the smoking status presented here is self-reported. In addition, detailed data on smoking intensity and duration of smoking were not recorded. Finally, the incidence rates of MI, stroke, and any revascularization were relatively low. This could be related to selection bias because only patients who signed informed consent were included in our study. Alternatively, the incidence rates may have been underestimated in the process of collecting data. Nonetheless, despite these limitations, our results emphasize the impact of smoking on long term MACE and cancer risk in patients with AMI.
In conclusion, the present large-scale multicenter study of AMI patients shows that smokers undergoing PCI were significantly younger and had less coronary risk factors compared with nonsmokers. Smoking was associated with worse cardiovascular outcomes and lung cancer in AMI patients during the 5-year follow-up period. Our results emphasize the public message concerning the harmful effects of cigarette smoking.
 XML Download
XML Download