

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF) is the most common form of sustained cardiac arrhythmia in the elderly population.1)2) AF increases the risk of mortality and morbidity resulting from stroke, congestive heart failure, and impaired quality of life, explaining its enormous socioeconomic and healthcare implications.1)2)3) The age distribution of AF among populations in the developed countries is predicted to shift in the coming years, with an expected increase in prevalence among the elderly. The fact that AF prevalence has progressively risen 2.10-fold over the past 10 years in Korea, with an increase to 8.15% in patients ≥80 years of age, supports this predicted progression.2) Globally, 40 million people are living with dementia, and this number is expected to increase with a rising aged population.4) Although the pathophysiological mechanisms of dementia are largely unknown, evidence is accumulating that AF may contribute to the development of cognitive dysfunction and dementia, even in patients without overt stroke.5)6)7)8) In this review, we summarize the evidence linking AF to dementia and critically appraise potential treatment strategies for preventing AF-associated cognitive decline.
Go to : 
ATRIAL FIBRILLATION AND DEMENTIA
Atrial fibrillation increases the risk of dementia
The Rotterdam study demonstrated that cognitive dysfunction was approximately twice as common in subjects with AF than in those without.5) However, the cross-sectional design of that study precluded definitive conclusions regarding a causal relationship. Since then, several longitudinal studies have investigated the association between AF and incidental dementia, with inconsistent results. Some studies have found that AF is associated with an increased risk of cognitive decline or dementia.6)7)8) Others have shown no association.9)10)
Kim et al.11) investigated the association of incidental AF with the development of incidental dementia in 262,611 dementia- and stroke-free participants aged ≥60 years, using the Korea National Health Insurance Service (NHIS)-Senior cohort. The incidence of dementia was 4.1 and 2.7 per 100 person-years in the incidental AF and propensity score-matched AF-free groups, respectively. Incidental AF, being analysed as a time-varying factor to avoid immortal time bias, is associated with higher risks of dementia with a hazard ratio (HR) of 1.52, even after additionally censoring participants at the time of an incidence of stroke with a HR of 1.27 (Figure 1). Incidental AF increased the risk of both Alzheimer's disease and vascular dementia.
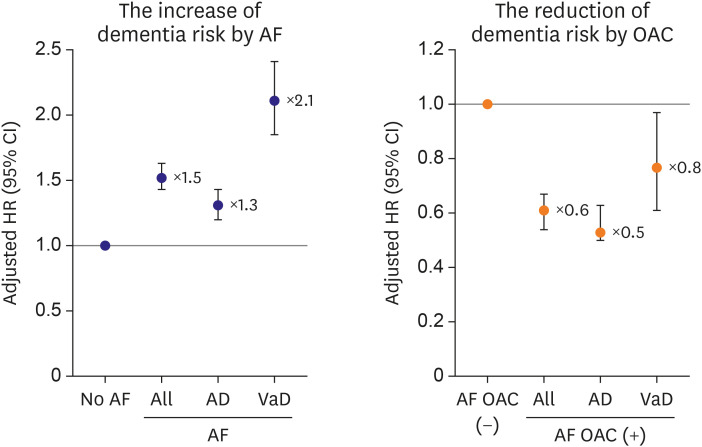 | Figure 1Risk of dementia according to atrial fibrillation in the study population (left). Effects of OAC on the risk of dementia in patients with atrial fibrillation (right). Figure courtesy of Kim et al.11)AD = Alzheimer's disease, AF = atrial fibrillation; CI = confidence interval; HR = hazard ratio; OAC = oral anticoagulant, VaD = vascular dementia.
|
Atrial fibrillation and early-onset dementia
In contrast to the aged population, early-onset dementia, with onset at age <65 years, is a devastating condition affecting patients who still have active socioeconomic involvements. The association between AF and dementia is not well identified in different age subgroups. Kim et al. investigated the associations between incidental AF and the risk of early-onset dementia / late-onset dementia (onset at age ≥65 years) in 428,262 participants without a history of dementia or stroke in the Korea NHIS-Health Screening cohort.12) Incidental AF was associated with an increased risk of both early- (HR, 2.91; 95% confidence interval [CI], 1.93–4.41) and late-onset dementia (HR, 1.67; 95% CI, 1.49–1.87), independently of a clinical stroke. Younger patients with AF were more prone to the development of dementia than older patients with AF (p for trend<0.001) (Figure 2).
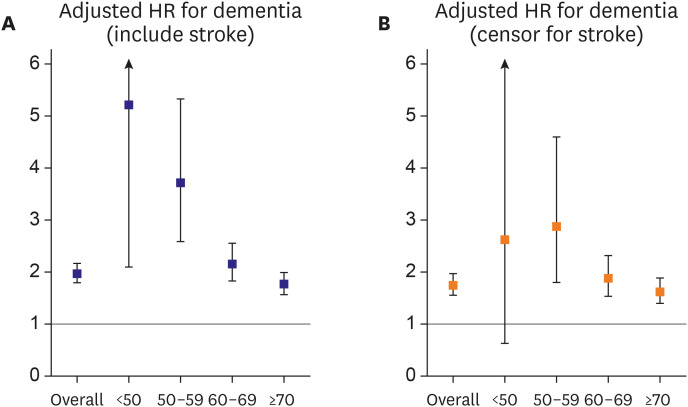 | Figure 2HRs for dementia per decade of age in the presence of AF. (A) Including stroke during the follow-up. (B) Excluding stroke during the follow-up. The horizontal line (at HR 1) indicates no difference in HRs between the AF and non-AF groups. Figure courtesy of Kim et al.12)AF = atrial fibrillation; HR = hazard ratio.
|
Go to :
HOW TO PREVENT DEMENTIA IN PATIENTS WITH ATRIAL FIBRILLATION
Lowering the risk of dementia with oral anticoagulants
Evidence is accumulating that the pathogenesis linking AF to dementia is likely multifactorial. However, cerebral infarction including silent stroke plays a central role.13) There is growing evidence to suggest that oral anticoagulants (OACs) are effective in lowering the risk of AF-related dementia, although preventing dementia is not the primary focus of OAC treatment in patients with AF.11)14)15) Kim et al. reported that OACs had a preventive effect on dementia with an HR of 0.61 among patients with incidental AF (Figure 1). A nationwide Swedish cohort study by Friberg and Rosenqvist14) found that patients with AF who received OAC treatment had a 29% lower risk of dementia than those with AF who were not prescribed OACs (HR, 0.71; 95% CI, 0.68–0.74). In the study, the benefit of OAC treatment appeared to be more prominent as it had been initiated since the initial diagnosis of AF, suggesting a dose-response relationship between time without OAC and the development of dementia. The same authors also reported that OAC use in AF patients aged >65 years was associated with a lower risk of dementia irrespective of their stroke risk score, suggesting the benefit of OAC even in patients with low risks.15)
Greater benefit of non-vitamin K antagonist oral anticoagulants than warfarin
In AF patients receiving warfarin, a lower time-in-therapeutic range has been associated with a higher risk of dementia.16)17) There is a concern regarding a higher risk of microbleeds in patients treated with warfarin, especially where the anticoagulation control is suboptimal. Microbleeds may cause chronic cerebral injuries and eventually lead to cognitive decline.18) Currently, there is no available randomized data on the efficacy of different OACs in preventing dementia in individuals with AF. A meta-analysis of 4 randomized trials comparing non-vitamin K antagonist oral anticoagulants (NOACs) to warfarin demonstrated that NOACs were associated with a significant risk reduction in terms of overall stroke and systemic embolism,19) with a greater effect observed in Asians compared to non-Asians.20) Since NOACs have more predictable pharmacokinetics, the therapeutic levels could be more steady. As such, it has been hypothesized that NOACs could further reduce the risk of dementia compared to warfarin. The risk of dementia according to oral anticoagulant regimens from Asian, European, and North American populations is presented in Figure 3. Two US cohort studies supported the hypothesis of a lower incidence of dementia in NOAC users compared with warfarin users.21)22) In contrast, nationwide Swedish and Danish cohort studies found similar incidences of dementia when comparing warfarin and NOAC usage in their patients.14)23) Large longitudinal studies with a longer follow-up time are needed to clarify the effect of NOACs on cognitive functions. Currently, several randomized-controlled clinical trials focusing on cognitive outcomes in patients with AF are in progress.24) Kim et al.25) enrolled 52,888 new OAC users with AF (aged ≥60 years, 31,211 NOAC users and 21,677 warfarin users) from the Korean NHIS database. Relative to propensity-matched warfarin users, NOAC users tended to have a lower risk of dementia (HR, 0.78; 95% CI, 0.69–0.90) (Figure 3). When comparing individual NOACs with warfarin, all the three NOACs (apixaban, dabigatran, and rivaroxaban) were associated with a lower dementia risk. The associations were more prominent among NOAC users on standard dosages.
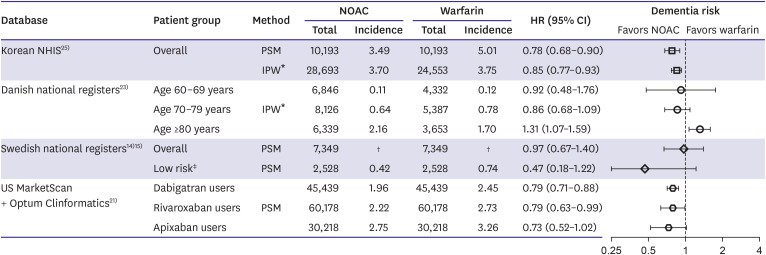 | Figure 3Risk of dementia according to oral anticoagulant regimens from Asian, European, and North American populations. Incidences were presented as rates per 100 person-years. Figure courtesy by Kim et al.25)Incidences were presented as rates per 100 person-years.
CI = confidence interval; HR = hazard ratio; IPW = inverse probability of treatment weighting; NHIS = National Health Insurance Service; NOAC = non-vitamin K antagonist oral anticoagulant; PSM = propensity score matching.
*Incidences and HRs were propensity-weighted; †Incidences were not presented in the article; ‡CHA2DS2-VASc ≤1 (no points for female sex).
|
Catheter ablation for atrial fibrillation can reduce the risk of dementia
Compared to antiarrhythmic drug therapy, catheter ablation for AF reduces the number of acute episodes and prolongs the duration of sinus rhythm, thereby improving the quality of life.26)27) Two recent studies demonstrated that cognitive function improved following catheter ablation.28)29) Conversely, AF ablation has been associated with declining cognitive function and acute brain lesions.30)31)32) However, a direct association between a silent cerebral embolism and decline in neurocognitive function is yet to be proven.33) The clinical significance of such asymptomatic cerebral embolic lesions is not known, and many will likely resolve to the point of being undetectable after weeks or months. These silent cerebral emboli are required to be distinguished from covert embolic strokes consequent to chronic AF.
Using the Korean NHIS database, Kim et al.34) compared the risk of dementia between 9,119 patients undergoing ablation and 17,978 patients managed using medical therapy (antiarrhythmic or rate control drugs). During a median follow-up of 52 months, compared to patients on medical therapy, ablated patients showed a lower incidence and a reduced risk of dementia overall (8.1 and 5.6 per 1,000 person-years, respectively; HR, 0.73; 95% CI, 0.58–0.93) (Figure 4). The association between ablation and a reduced dementia risk was consistently observed even after additionally censoring for incidental strokes (HR, 0.76; 95% CI, 0.61–0.95). The protective effect of ablation against dementia was strongly observed for the ablation success group, in whom the sinus rhythm was likely maintained. The authors inferred that the restoration of sinus rhythm, and not the ablation procedure itself, was the important mechanism. However, in the claims-based database the study used, repeated ablation, cardioversion, and antiarrhythmic drug use were the only indices of post-ablation AF recurrences; thus, the actual burden of AF was unknown.
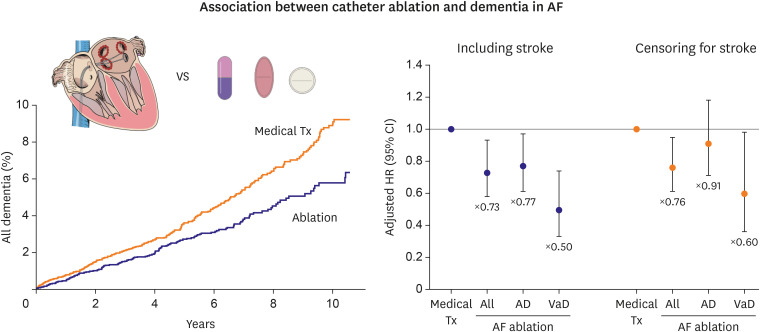 | Figure 4Cumulative incidence curves of overall dementia in propensity-matched patients undergoing ablation or medical therapy (left). Risk of dementia in propensity score-matched patients undergoing ablation or medical therapy (right). Figure courtesy of Kim et al.34)AD = Alzheimer's disease, AF = atrial fibrillation; Tx = treatment; VaD = vascular dementia.
|
Go to :
RISK FACTOR CONTROL AND DEMENTIA
Risk factors and brain
AF is highly prevalent. A prevalence of 1–2% is found in the general population but this increases up to 10% in elderly individuals aged over 80 years.2) Dementia is also increasingly common in the elderly. This poses a major global challenge for healthcare and social care in ageing populations.35) The relationship between AF and dementia may also be explained by common vascular risk factors which increase with advancing age.36) Cox et al.37) observed associations of smoking, hypertension, pulse pressure, diabetes, hypercholesterolemia, body mass index (BMI), and waist–hip ratio, with poorer brain health across grey and white matter macrostructure and microstructure among 9,722 individuals of 44–77 years of age.37) Yaffe et al.38) also reported that increased cumulative exposures to hypertension, hyperglycemia, and hypercholesterolemia was associated with worse cognitive dysfunctions.
Since AF patients have a higher risk of dementia, the ability to predict its occurrence in the AF population is critical. A recent study showed that the CHA2DS2-VASc score was a significant predictor of dementia in AF subjects even after censoring for strokes.11) Therefore, physicians should be vigilant in detecting clinical manifestations that imply potential cognitive decline and functional impairment in AF patients, especially those with a high CHA2DS2-VASc score. This finding also implies that subclinical strokes and the shared risk factors play significant roles in the development of dementia among patients with AF.
Optimal blood pressure control
There is accumulating evidence indicating that hypertension in midlife increases the risk of dementia in later life, suggesting it to be a potentially modifiable risk factor.39)40)41) However, results of randomized clinical trials have generally been inconclusive regarding the effects of blood pressure (BP) reduction on cognitive outcomes in the general population.42)43)44) Since hypertension is common in patients with AF, the population attributable risk and potential healthcare burden are large.2)45) High stroke incidence and frequent OAC use in patients with AF increase the complexity of the relationship between hypertension and dementia risk.
Recently, Kim et al.46) reported a U-shaped relationship between systolic or diastolic BP and dementia risk in an analysis of 171,228 Korean patients aged 50–69 years, with incidental AF but no existing dementia (Figure 5). A 10 mmHg increase or decrease in the systolic BP, starting from a baseline of 120 mmHg, was associated with 4.4% (95% CI, 2.7–6.0%) and 4.6% (95% CI, 0.1–8.2%) higher dementia risk, respectively (Figure 5A). An increase or decrease of diastolic BP starting from a baseline of 80 mmHg also increased the dementia risk (Figure 5B). Time-updated regression of the study suggested that the optimal BP range for preventing dementia as 120 to 129/80 to 84 mmHg. An increased dementia risk in patients with high BP is present even after censoring for incidental strokes, suggesting that subclinical vascular brain injury including white matter lesions, microbleeds, and covert or microscopic infarcts, might be an important mechanism underlying the relation between hypertension and AF-associated dementia, as suggested in recent studies investigating magnetic resonance imaging of the brain and associated dementia among AF patients.47) The authors also reported that hypertension burden (the proportion of days with increased BP during follow-up) was linearly associated with higher dementia risk (HR, 1.10 per 10% increase, 95% CI, 1.08–1.12), suggesting that minimizing the burden of hypertension in AF patients may help to prevent dementia (Figure 6).
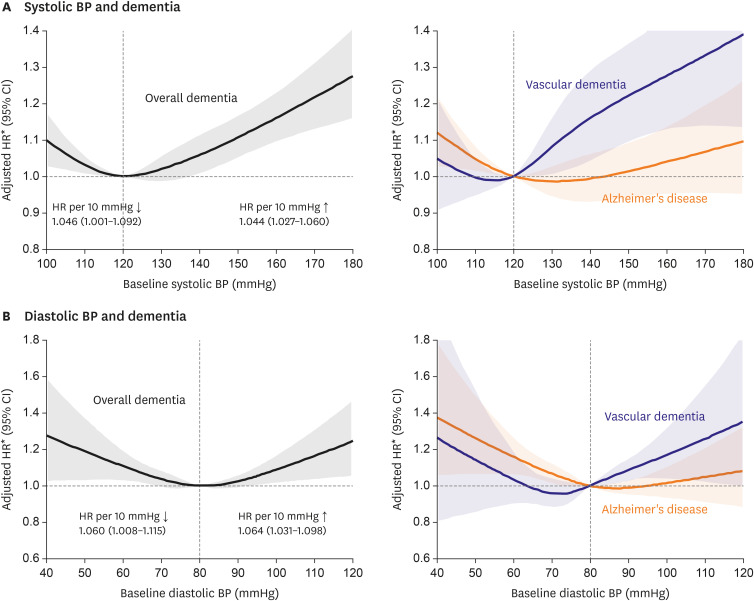 | Figure 5Association of (A) systolic and (B) diastolic BP at baseline with dementia risk. Figure courtesy of Kim et al.46)BP = blood pressure; CI = confidence interval; HR = hazard ratio.
*HRs were calculated with a systolic or diastolic BP of 120 or 80 mmHg as reference.
|
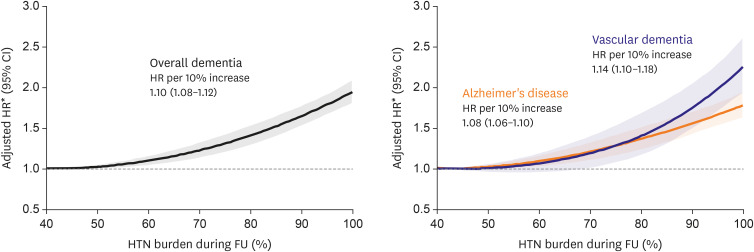 | Figure 6Association of hypertension burden during follow-up with dementia risk. Figure courtesy of Kim et al.46)CI = confidence interval; FU = follow-up; HR = hazard ratio; HTN = hypertension.
*HRs were calculated with the burden under 40% as reference.
|
Integrated atrial fibrillation management
Recently published Korean and European AF guidelines advocated the AF Better Care (ABC) pathway for a more integrated approach beyond anticoagulation therapy for patients with AF, with the aim to reduce death and adverse outcomes in AF.27)48) This ABC pathway facilitates care as follows: ‘A’ Avoid stroke with optimal anticoagulation; ‘B’ Better symptom management; and ‘C’ Cardiovascular and comorbidity management.49) Yoon et al.50) previously reported that compliance with the ABC pathway was associated with improved clinical outcomes in patients with AF. Application of the simple ABC pathway was associated with a lower risk of all causes of death and the composite outcome including all causes of death, ischemic stroke, myocardial infarction, or major bleeding, in patients with AF.50)51)52)
Yang et al.53) evaluated whether compliance with the ABC pathway was associated with a lower risk of dementia. In fact, the ABC compliant patients with AF had a lower risk of dementia overall, as well as a reduced risk of Alzheimer's disease and vascular dementia. Since ischemic stroke is closely related to an increased risk of dementia, the reduction of dementia risk in the ABC group may be related to oral anticoagulation adherence and the control of risk factors. The findings that adherent use of NOAC was associated with a lower risk of ischemic stroke without increasing bleeding risk supports the hypothesized pathway.54) The strong impact of the ABC pathway on the risk of dementia substantiates and strengthens the concept that a holistic approach for integrated management is associated with a significant clinical benefit for patients with AF.
Other risk factors
The modification of risk factors (obesity, hypertension, heart failure, diabetes mellitus, and sleep apnea) related to the development and/or progression of AF could delay the onset and progression of cognitive dysfunctions.55)56) In lean Asian populations, prehypertension and impaired fasting glucose were important risk factors of AF, implying that strict blood pressure control and early treatment of diabetes should be emphasized.57) Avoiding abdominal obesity58) and weight fluctuation59) have been associated with reduced risk of AF development, which possibly reduces or delays the onset and progression of cognitive decline.
Lifestyle behaviors such as smoking, drinking, and physical activity should be monitored in an integrated manner. Alcohol abuse has been associated with an increased risk of dementia (HR, 1.53; 95% CI, 1.41–1.66) among patients with AF in an observational cohort study.14)
Go to :
CONCLUSIONS
Incidental AF was associated with an increased risk of both early- and late-onset dementia, independent of clinical strokes. Younger patients with AF were more prone to the development of dementia than older patients with AF. A higher CHA2DS2-VASc score was a significant predictor of dementia in patients with AF even after censoring for strokes. Among patients with AF, OAC use was related to a lower incidence of dementia. In particular, NOAC usage was associated with a reduced risk of dementia compared with warfarin. Moreover, successful catheter ablation for AF was associated with a decreased dementia risk. Among midlife AF patients, there were a U-shaped association of BP and a linear association of hypertension burden with dementia risk. Minimizing the burden of hypertension in patients with AF may help to prevent dementia. Finally, integrated management of AF was associated with a reduced risk of dementia. In sum, due to the high medical burden of AF and dementia, it is necessary to implement integrated AF management to reduce the risk of dementia.
Go to :
 XML Download
XML Download