

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Total hip arthroplasty (THA) is the recommended treatment for patients with hip osteoarthritis who have failed both pharmacological and non-pharmacological treatments for severe pain.1 THA is the fourth most common surgery in the United States and was done for 460 million people in 2012.234 In 2013, 22,000 THAs were done, making it one of the 20 most common surgeries in Australia.5
However, despite these advantages, THA is associated with severe pain after surgery. Pain after THA can adversely affect early patient recovery postoperatively.6 In addition, pain can negatively affect mobility after surgery, increasing the risk of venous thromboembolism and interfering with rehabilitation. As a result, the consequences of such pain can prolong patient recovery and increase hospital stays and cost.7 In order to improve the patient's quality of life and improve postoperative results, it is necessary to emphasize proper postoperative pain management. Therefore, many pain management drugs and procedures are used to manage pain after surgery.8
As the cardiovascular risk of nonsteroidal anti-inflammatory drugs (NSAIDs), the ones most commonly used to control pain in these elderly patients, became known, the threshold for opioid use decreased.9 Because opioid painkiller purchases quadrupled between 1999 and 2010, the use of prescription drugs in the United States has been a danger to public safety over the last decade.10 Opioids can cause side effects, such as sedation, dizziness and balance problems, nausea, vomiting, constipation, and respiratory depression, and long-term use can lead to tolerance and physical dependence and sometimes, to addiction.11 Various studies on opioid use after THA reported prolonged opioid use before surgery as a representative risk factor for chronic use of opioid after THA.1213 Also, preoperative opioid use is associated with high complication rate and increased mortality after surgery.1214 And, it is reported that preoperative chronic users continue to use opioids up to 47%–62% at 1 year after surgery.15 However, studies on opioid use in patients with THA in East Asian countries are still lacking.
Therefore, the purpose of this study was to investigate the use of opioids before and after THA, to find out the effect of opioid use on mortality in patients with THA, and to analyze whether preoperative opioid use is a risk factor for sustained opioid use after surgery using Korean nationwide cohort data.
Go to : 
METHODS
Study subjects
The Korean National Health Insurance Service-Sample cohort (NHIS-Sample) was used to identify patients with THA. The NHIS-Sample was compiled and provided by the NHIS of South Korea for research purposes.16 To represent all people in South Korea, a total of 1,000,000 participants as of 2006 were selected into the NHIS Sample by simple 10% random sampling. Unless there was a disqualification, such as emigration or death, all the individuals in the NHIS Sample were followed until December 31, 2015. In addition to this data, data of all participants from 2002 to 2005 are provided. Under the single-insurer system of universal health coverage, the NHIS has all personal information, including demographics, medical use, or treatment information, for the Korean people.161718 The information in the data set included all inpatient and outpatient medical claims and prescription claims, including treatment and diagnostic procedures, and codes for generic prescription names.
Primary THA cohort
The eligibility criteria for patients with primary THA were as follows19: 1) first-time admission to a hospital with a surgery code of THA (International Classification of Diseases, 10th Revision [ICD-10] N0711, N2070); 2) at least a three-year THA-free period; 3) age 18–99 years at the time of THA. The exclusion criteria were as follows: To guarantee a minimal 1-year observation, patients with THA occurring less than 365 days before the end of the follow-up period (December 31, 2015) were excluded. 1) Patients with THA prior to December 31, 2004, were also excluded to ensure at least a 3-year THA-free period. 2) Patients with past history of malignancy. 3) Patients who had undergone THA twice were excluded. The last date of follow-up was defined as the date of death or December 31, 2015, whichever came first. To identify the use of opioids, the index date (time zero) was defined as 90 days after admission to a hospital to fulfill the eligibility criteria of patients with primary THA.
All-cause mortality
In the NHIS-Senior, each subject's unique de-identified number was linked to vital statistics, including dates and causes of death, from the Korean National Statistical Office.16 The dates of death from the mortality information were used to calculate the survival times.
Categorization by type of opioid and definition of opioid exposure
Opioids were defined as morphine, hydromorphone, oxycodone, dihydrocodeine, codeine, hydrocodone, pethidine, fentanyl, pentazocine, buprenorphine, butorphanol, nalbuphine, tapentadol, sufentanil, remifentanil, and tramadol.2021 The opioids were categorized into tramadol and strong opioids (other opioids except for tramadol). The patients who used opioids within six months before THA was defined as past users. If there was no history of opioid use within six months before THA, the patient was defined as a past non-user. Patients who received opioids within three months after THA were defined as current users, and those who did not were defined as current non-users. The cumulative dose of current tramadol and strong opioid use was calculated by adding the amount of dispensed defined daily dosages.22 To identify the sustained use of tramadol and strong opioids, their use was investigated during the period from three months to one year after THA (defined as sustained user).
Past and current medication history of antihypertensive, antidiabetic, lipid-lowering, and anti-rheumatoid agents; anti-platelet, anti-dementia, and anti-Parkinson drugs; antiepileptics, antipsychotics, NSAIDs, COX-2 inhibitors, steroids, and warfarin within six months before hip fracture and within three months after hip fracture were investigated.
Statistical analysis
The baseline characteristics were identified at the time of admission for THA. Survival time used in the survival analyses was defined by days from the index date (90 days after THA admission) to the date of death or December 31, 2015, whichever came first. Patients who died during the 90-day landmark period were truncated. We used a multivariable-adjusted Cox proportional hazards model to investigate the effects of tramadol and strong opioid use on all-cause mortality in patients with THA. The effect sizes are presented as hazard ratios (HRs) and 95% confidence intervals (CIs). We used a generalized estimating equation model with a Poisson distribution and logarithmic link function to estimate the adjusted rate ratios (aRRs) and 95% CIs to assess the association between past use and sustained use. The potential confounders included were age group, gender, household income level, Charlson Comorbidity Score (CCS), anesthesia, transfusions, calendar year of the THA, past medication history and current medication history, which included tramadol and strong opioids. We used Quan's ICD-10 coding algorithm of the CCS23 diagnostic codes during the three years before THA admission to assess each subject's comorbidities. The presence of CCS disease-constituting categories was defined by at least two outpatient visits or one admission upon the primary or first secondary diagnosis. We did the statistical analyses using SAS Enterprise Guide version 7.1 (SAS Institute, Cary, NC, USA); a P < 0.05 was considered to be statistically significant.
Ethic statement
The study design and protocol were approved by the Institutional Review Board (IRB) of our Hospital (IRB No. 2020-03-007). Written informed consent was waived for all patients involved in this study.
Go to :
RESULTS
Between January 1, 2002, and December 31, 2015, a total of 1,766 patients were admitted to hospitals for THA. Of these patients, 645 were excluded because they did not meet the inclusion criteria (217 patients, 3-year free period; 149 patients, guarantee a 1-year observation; 1 patient, under 18 years; 205 patients, THA twice or more; 60 patients, histories of malignancy). Also, 13 patients who died within 90 days after hip fractures were excluded. A total of 1,121 patients were included in this study. The patient demographics and medication histories are presented in Tables 1 and 2.
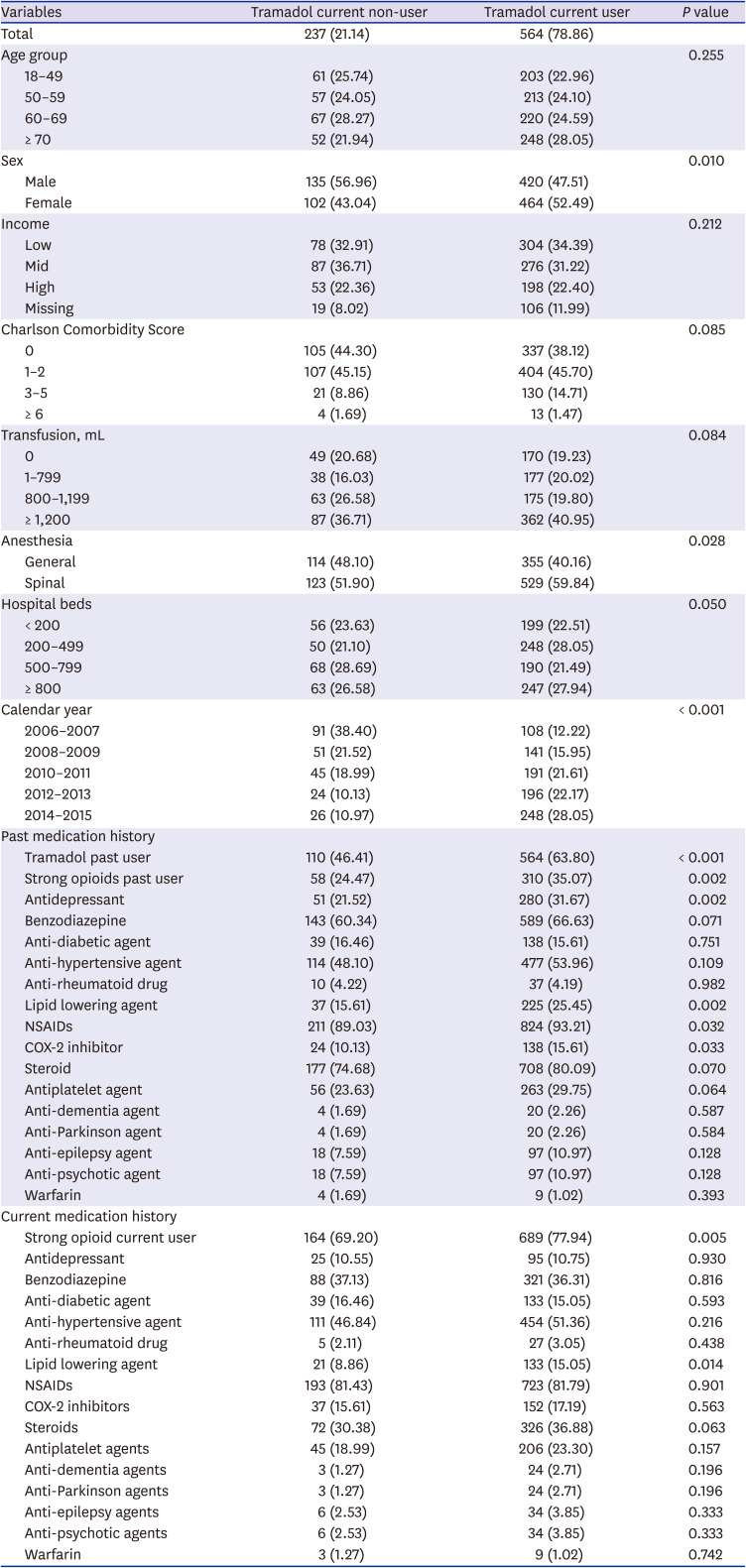
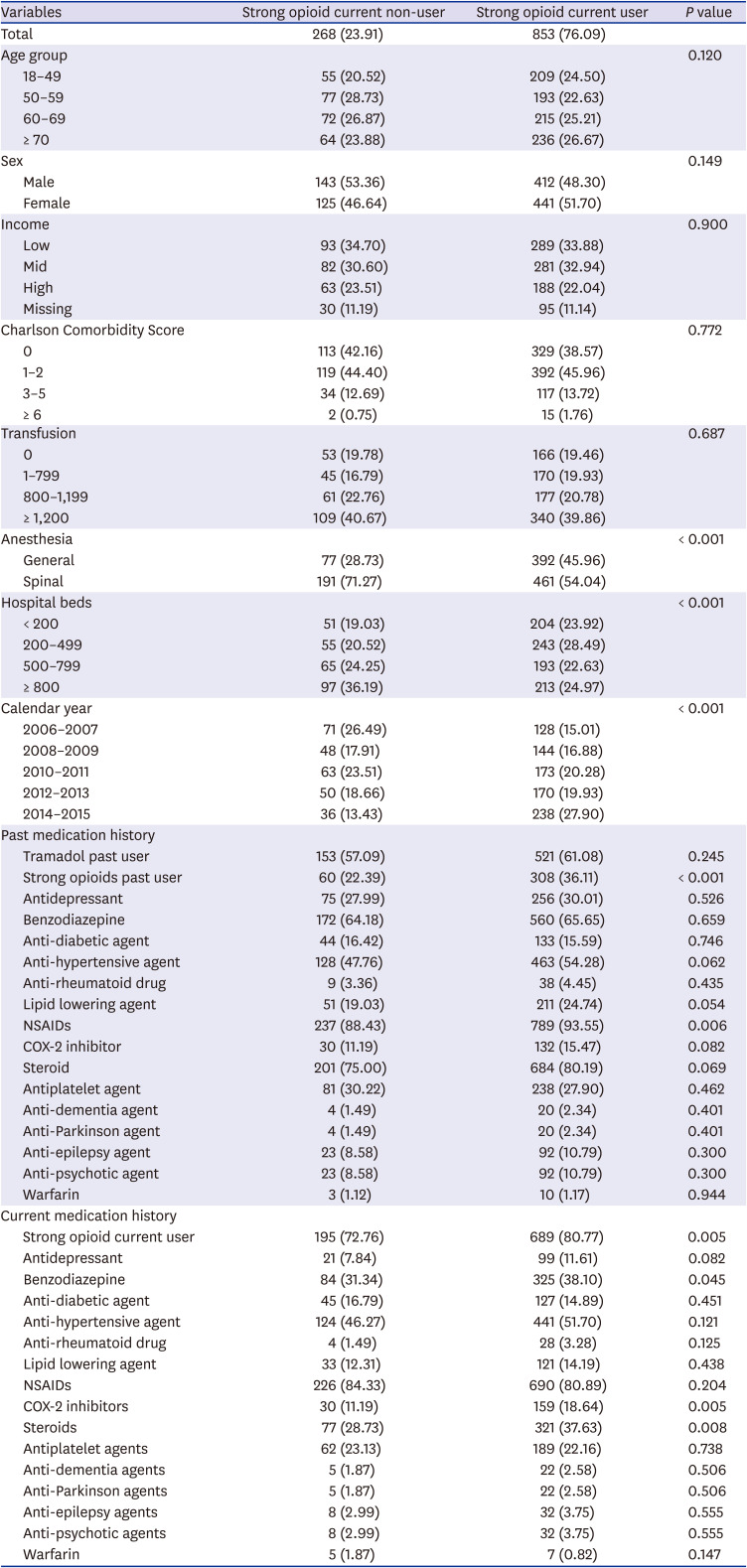
Table 1
Demographics and medication histories according to current use of tramadol
![]()
Table 2
Demographics and medication histories according to current use of strong opioid
![]()
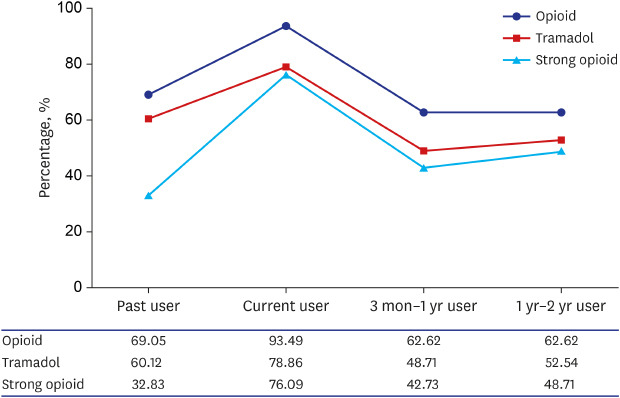
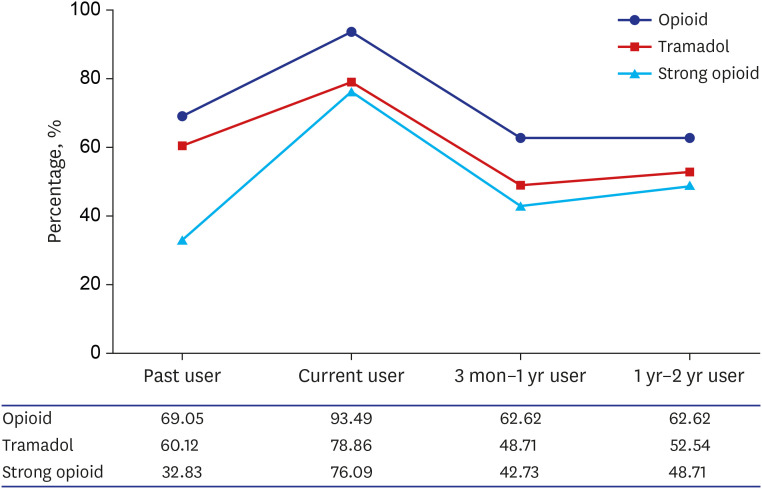
There were 774 (69.05%) patients who were past users of opioids (Fig. 1). There were 674 (60.12%) past users of tramadol and 368 (32.83%) past users of strong opioids. The number of current opioid users increased to 1,048 (93.49%). The numbers of current tramadol and strong opioid users were 884 (78.86%) and 853 (71.09%), respectively. The sustained users of opioids decreased to 702 (62.62%) patients. The trends in the use of tramadol were similar to that for opioids. However, the sustained use of strong opioids increased compared to past use of opioid.
In the comparison of death risk according to current use and the defined daily dose of tramadol in each patient group according to past opioid use, there were no statistically significant differences in the adjusted HR for death compared to the current non-users in all groups (P > 0.05) (Table 3). In the comparison of death risk according to current use and the defined daily dose of strong opioids in each patient group according to past opioid use, there were no statistically significant differences in the adjusted HR for death compared to the current non-users in all groups (P > 0.05) (Table 4).
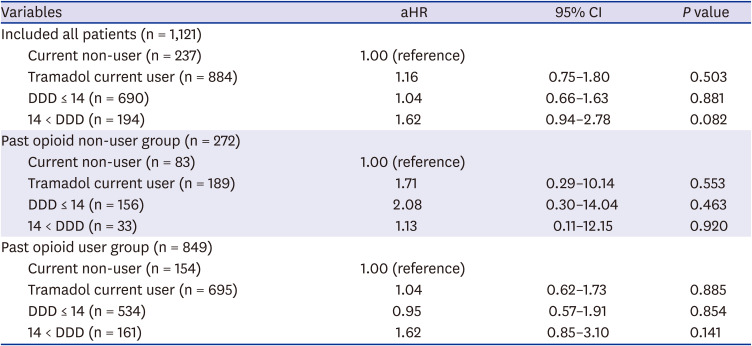
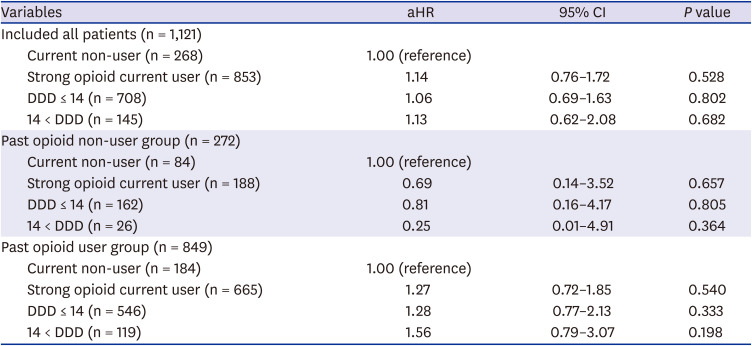
Table 3
Comparison of hazard for death according to current use and DDD of tramadol in each patient groups according to the presence of past opioid use
![]()
Table 4
Comparison of hazard for death according to current use and DDD of strong opioid in each patient groups according to the presence of past opioid use
![]()
Past tramadol and strong opioid use in current users increased the risk of sustained use of tramadol and strong opioids 1.45-fold (aRR; 95% CI, 1.12–1.87; P = 0.004) and 1.65-fold (aRR; 95% CI, 1.43–1.91; P < 0.001), respectively, compared to past non-users (Table 5). Also, the risks for sustained use of tramadol and strong opioids increased in both groups regardless of age.
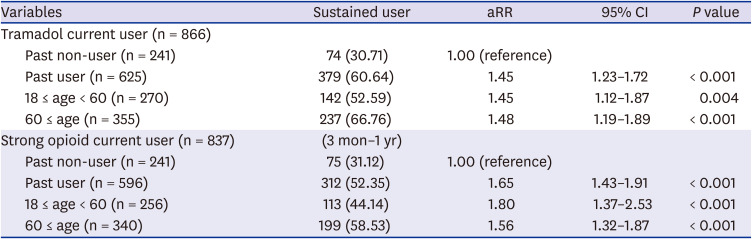
Table 5
Among the current user of tramadol and strong opioid, the relationship between past user and sustained user of tramadol and strong opioid after 3 months of hip fracture in survivor until 1 year after hip fracture
![]()
Go to :
DISCUSSION
The main finding of this study was that of the THA patients, 774 (69.05%) were past users of opioids, 674 (60.12%) were past users of tramadol, and 368 (32.83%) were past users of strong opioids. In addition, the number of current opioid users after THA was 1,048 (93.49%) with current tramadol and strong opioid users being 884 (78.86%) and 853 (71.09%), respectively. However, the sustained users of opioids decreased to 702 (62.62%) patients. In addition, the sustained use of strong opioids increased compared to past use of opioids. Past tramadol and strong opioid use in current users increased the risk of sustained use of tramadol and strong opioids 1.45-fold and 1.65-fold, respectively, compared to past non-users. Also, the risks for sustained use of tramadol and strong opioids increased in both groups regardless of age. When comparing the risk of death from current use and daily tramadol doses defined in each patient group from past opioid use, there was no statistically significant difference in deaths compared to current non-users in all groups.
Opioid has been reported as one of the common causes of medication related death, and Summer et al reported that mortality after hip fracture surgery was higher in opioid users compared to non-users.2425 However, previous studies on opioid use after total joint arthroplasty are limited to studies on the risk factors of chronic opioid use or whether opioid use is related to postoperative functional outcome, readmission, infection, and revision rate.122627 Also, there are few analyses of the effect of opioid use on death after THA. And, study designs that consider both preoperative and postoperative use after THA are also rare. Moreover, no studies have analyzed the effects of opioids in different age groups. Kim et al.28 investigated the association of preoperative opioid use among patients 65 years and older with mortality and other complications at 30 days after total knee arthroplasty. They reported that there were no statistically significant differences in in-hospital or 30-day mortality between continuous opioid users and opioid-naive patients. Fortunately, the results of our study are consistent with the above study. This is probably because the dosage and pattern of opioid prescriptions in Korea are different from those in Western countries.
Chen et al.29 reported that the proportion of chronic opioid users at 3 months postoperatively was 19% and decreased to 4% at 1 year in total joint arthroplasty patients 65 years of age or older. Pivec et al.30 reported that 19% of preoperative opioid users and 4% of preoperative non-opioid users were still using opioid at last follow-up. However, in our study, the proportion of opioid users reached 69% before THA, and even after 1 year or more after surgery, it was lower than before surgery, but it was 62%, indicating that opioids are still used in these patients at a high rate. This is thought to be due to differences in the definition of the types and user of opioids included in the study. In this study, if there was even one opioid prescription, it was classified as an opioid user, and the cause of opioid use was not identified. Nevertheless, the proportion of opioid users decreased at 1 year after surgery than before, and THA appears to be effective in reducing pain in these patients. However, there is a report that the use of opioid is high in patients with revision surgery, so it is considered that attention should be paid to follow-up of patients using opioid after surgery.13
One of the most important issues in the use of opioids is abuse and addiction. Goesling et al.31 did well-designed prospective studies for assessing trends and predictors of opioid use following total knee and THA. They estimated that 4.3% of patients who were opioid naïve on the day of surgery had opioid usage at postoperative 6 months. In contrast, 34.7% of THA patients who registered opioid usage on the day of surgery maintained opioid use at 6 months. Patients consuming > 60 mg oral morphine equivalents preoperatively had an 80% chance of continued postoperative use. In this study, current opioid users showed a high rate of continued use of opioids, and the use of strong opioids in this patient group was also high. Kim et al.32 used statistics on claims (2004–2013) from the US Private Health Program, recognizing individuals who received hip or knee arthroplasty and obtained ≥ 1 opioid prescription within 30 days of operation. They reported that overall, 7.6% persistently used opioids after the surgery. Among patients who used opioids 80% of the time for ≥ 4 months preoperatively (3,023 patients), 72.1% became persistent users. Preoperative opioid usage trends were good predictors of continued opioid use after surgery. In our study, as in previous studies, the proportion of sustained users after surgery was higher in preoperative opioid users. Moreover, this phenomenon has been observed not only in patients 65 years of age or older, but also in patients with younger age. Recently, it has been reported that opioid prescriptions are increasing in Korea. When using opioids for postoperative pain control after THA, taking history of preoperative medication use is thought to be important to prevent sustained use of opioids.33
This study has several limitations. First, we were unable to assess the severity of the specific disease or pain for which THA was done. In addition, we have not been able to confirm indications for opioids. In other words, some patients may have used opioids for reasons other than the health status of the disease for THA surgery. This is an obvious limitation of our observational cohort studies. However, we tried to investigate not only CCS, but also several medications to adjust for the various underlying diseases in these patients. Second, the patient's functional status, pain level, or other behavioral factors related to opioid use were not analyzed. Third, we were unable to assess whether the patient was actually taking the drug as prescribed or how often. Fourth, there is a possibility of misclassification, because we relied on diagnostic or procedural codes to define the type of operation and diagnosis, and the history of taking opioids.
In THA patients, the use of opioids within 6 months before surgery and within 3 months after surgery does not affect postoperative mortality, but past use of opioids is a risk factor for sustained opioid use. Even after THA, the use of strong opioids increases compared to use before surgery.
Go to :
 XML Download
XML Download