

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cytomegalovirus (CMV) is known to cause congenital and postnatal infections in neonates. CMV may be transmitted placentally; via aspiration of secretions in the birth canal, or by exposure to infected secretions such as breast milk, saliva, or blood products.123 The prevalence of congenital CMV infection was reported to be 0.23%–0.64% in neonates456 and 1.3%–2.3% in very low-birth-weight infants.78 Postnatal CMV infection is generally asymptomatic in full term babies,1 but clinically symptomatic infection or long term-sequelae after perinatal CMV infection can occur in premature infants.19
Lanzieri et al.10 in 2013 and Kurath et al.11 in 2008 reported meta-analyses of breast milk-acquired infections in very low-birth-weight and premature infants. In 2012, the American Academy of Pediatrics (AAP) indicated that fresh breast milk is recommended over frozen or pasteurized milk for all preterm and full-term infants, even when the mother is CMV seropositive.12 However, the feeding protocols for preterm infants born to CMV-positive mothers vary by country.131415 Unlike congenital infection, postnatal CMV infection acquired via breast milk is usually asymptomatic and is not associated with severe morbidity and mortality, especially in full-term infants.11617 However, cases of symptomatic and severe CMV infection have been reported in very immature infants fed fresh breast milk.91819202122 Adolescents who suffered CMV infections soon after preterm birth exhibited long-term neuropsychological sequelae.23 We performed a systematic review and meta-analysis to evaluate the rate of breast milk-acquired CMV infection in preterm infants born to CMV-seropositive mothers since the 2012 AAP recommendation.
METHODS
Search strategy and study selection
In keeping with the review guidelines developed for systematic reviews and meta-analyses, we searched PubMed, Embase, and Cochrane Library databases using the terms: (“breast feeding” or “breast milk” or “human milk” or “breast”) and (“HCMV” or “cytomegalovirus”) and (“infant, extremely premature” or “premature birth” or “newborn” or “neonate” or “low birth weight” or “very low birth weight” or “premature” or “preterm infant”). We also performed manual searches of the reference lists of included studies and other electronic databases. The last search was performed on November 11, 2017. We first screened the articles by titles and abstracts, and the full-text articles were then independently reviewed by two reviewers (Park HW and Cho MH) using the selection criteria noted below for inclusion in the meta-analysis. No restrictions were applied on language. Ethical approval was not necessary because this meta-analysis was performed using the data from published studies.
Inclusion criteria
Studies were included for meta-analysis if they met the following criteria: 1) study design: cross-sectional, prospective cohort, or observational study; 2) patients: newborn infants born prematurely; 3) intervention: breast milk feeding; and 4) outcomes: CMV infection in newborn infants.
Data extraction and methodological quality assessment
Two authors (Park HW and Cho MH) reviewed the full text of all included studies independently and extracted the following data using a standardized form: first author, publication year, study population, study location, study design, study period, CMV detection method in infants and in mothers, maternal serologic status, definition of congenital CMV infection, information on blood transfusions, CMV shedding into breast milk, breast-fed neonates, CMV infection in neonates, and breast milk preparation method.
The quality of the included studies was assessed using a checklist for prevalence studies from the Joanna Briggs Institute, as described by Munn et al.24 This tool comprises the following nine questions:
1) Was the sample frame appropriate to address the target population?
2) Were study participants sampled in an appropriate way?
3) Was the sample size adequate?
4) Were the study subjects and the setting described in detail?
5) Was the data analysis conducted with sufficient coverage of the identified sample?
6) Were valid methods used for the identification of the condition?
7) Was the condition measured in a standard, reliable way for all participants?
8) Was there appropriate statistical analysis?
9) Was the response rate adequate, and if not, was the low response rate managed appropriately?
Each item could be rated as “yes,” “no,” “unclear,” or “not applicable.” Any disagreement during full text review or quality assessment of included studies was resolved by discussion with a third reviewer (Lee R), followed by reevaluation of the study.
Data synthesis and statistical analysis
We conducted a meta-analysis to generate pooled estimates of the CMV infection rate after feeding with CMV-positive breast milk and of CMV infection in neonates born to CMV-seropositive mothers using Comprehensive Meta-Analysis version 3.3 (Biostat, Englewood, NJ, USA). We used a random effects model for analysis if there was significant heterogeneity between studies. The meta-analysis was performed using a fixed effect mode, if there is no heterogeneity between studies. To assess statistical heterogeneity, we used the I2 statistic, which is expressed as percentage of total variation across studies. I2 values greater than 50% indicated significant heterogeneity. A sensitivity analysis was conducted, excluding individual studies sequentially, to explore the potential causes of heterogeneity and the effect of each study on the results. A cumulative analysis by year of publication was performed to detect temporal trends, adding one study at a time. We used the Begg–Mazumdar rank correlation test, Egger's regression test, and inspection of a funnel plot to assess publication bias. The presence of asymmetry of the funnel plot or P values < 0.05 in the Egger's regression test were taken as indicating publication bias. This study has been reported in accordance with the ‘Preferred Reporting Items for Systematic reviews and Meta-analysis (PRISMA)’ 2009 checklist (Supplementary Table 1).
RESULTS
Literature search and characteristics of the included studies
A total of 585 studies potentially relevant to this meta-analysis of breast milk-acquired CMV infection in preterm infants were initially identified from database searching. During the review process, 566 of these were excluded for the reasons listed in Fig. 1. Thus, 19 studies were included in this systematic review and meta-analysis. The 19 included studies examined a total of 2,502 newborns. Included studies were performed in 10 countries from North America, Europe, Asia, the Middle East, and Latin America (Table 1). The characteristics of the included studies are shown in Table 1.
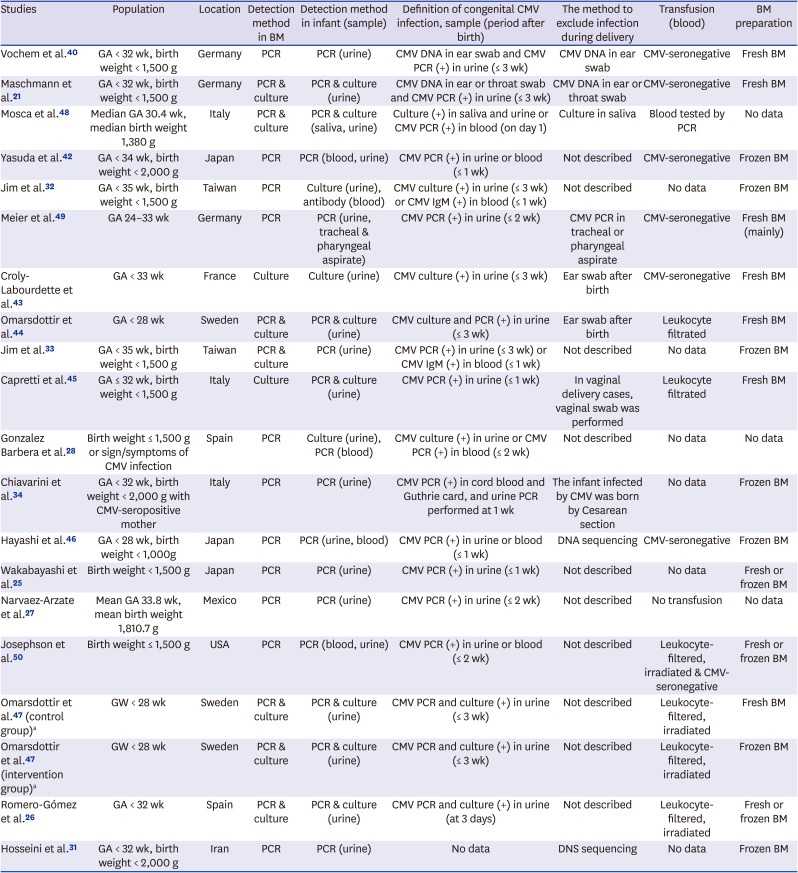
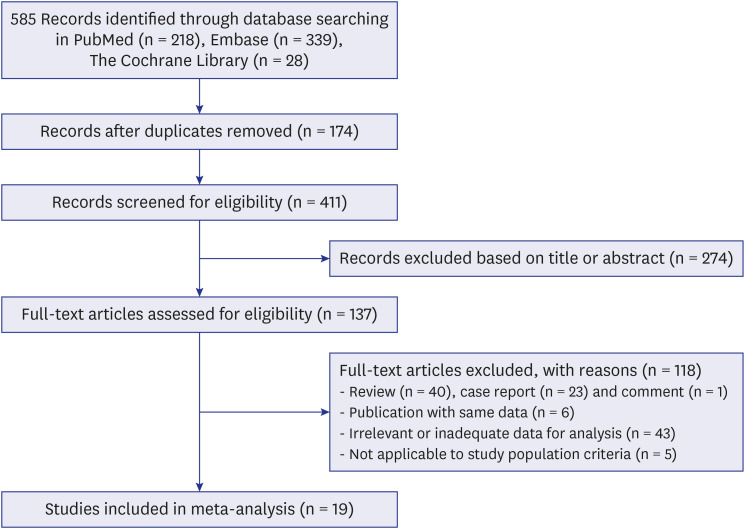
Table 1
Characteristics of studies included in this meta-analysis
| Studies | Population | Location | Detection method in BM | Detection method in infant (sample) | Definition of congenital CMV infection, sample (period after birth) | The method to exclude infection during delivery | Transfusion (blood) | BM preparation |
|---|---|---|---|---|---|---|---|---|
| Vochem et al.40 | GA < 32 wk, birth weight < 1,500 g | Germany | PCR | PCR (urine) | CMV DNA in ear swab and CMV PCR (+) in urine (≤ 3 wk) | CMV DNA in ear swab | CMV-seronegative | Fresh BM |
| Maschmann et al.21 | GA < 32 wk, birth weight < 1,500 g | Germany | PCR & culture | PCR & culture (urine) | CMV DNA in ear or throat swab and CMV PCR (+) in urine (≤ 3 wk) | CMV DNA in ear or throat swab | CMV-seronegative | Fresh BM |
| Mosca et al.48 | Median GA 30.4 wk, median birth weight 1,380 g | Italy | PCR & culture | PCR & culture (saliva, urine) | Culture (+) in saliva and urine or CMV PCR (+) in blood (on day 1) | Culture in saliva | Blood tested by PCR | No data |
| Yasuda et al.42 | GA < 34 wk, birth weight < 2,000 g | Japan | PCR | PCR (blood, urine) | CMV PCR (+) in urine or blood (≤ 1 wk) | Not described | CMV-seronegative | Frozen BM |
| Jim et al.32 | GA < 35 wk, birth weight < 1,500 g | Taiwan | PCR | Culture (urine), antibody (blood) | CMV culture (+) in urine (≤ 3 wk) or CMV IgM (+) in blood (≤ 1 wk) | Not described | No data | Frozen BM |
| Meier et al.49 | GA 24–33 wk | Germany | PCR | PCR (urine, tracheal & pharyngeal aspirate) | CMV PCR (+) in urine (≤ 2 wk) | CMV PCR in tracheal or pharyngeal aspirate | CMV-seronegative | Fresh BM (mainly) |
| Croly-Labourdette et al.43 | GA < 33 wk | France | Culture | Culture (urine) | CMV culture (+) in urine (≤ 3 wk) | Ear swab after birth | CMV-seronegative | Fresh BM |
| Omarsdottir et al.44 | GA < 28 wk | Sweden | PCR & culture | PCR & culture (urine) | CMV culture and PCR (+) in urine (≤ 3 wk) | Ear swab after birth | Leukocyte filtrated | Fresh BM |
| Jim et al.33 | GA < 35 wk, birth weight < 1,500 g | Taiwan | PCR & culture | PCR (urine) | CMV PCR (+) in urine (≤ 3 wk) or CMV IgM (+) in blood (≤ 1 wk) | Not described | No data | Frozen BM |
| Capretti et al.45 | GA ≤ 32 wk, birth weight < 1,500 g | Italy | Culture | PCR & culture (urine) | CMV PCR (+) in urine (≤ 1 wk) | In vaginal delivery cases, vaginal swab was performed | Leukocyte filtrated | Fresh BM |
| Gonzalez Barbera et al.28 | Birth weight ≤ 1,500 g or sign/symptoms of CMV infection | Spain | PCR | Culture (urine), PCR (blood) | CMV culture (+) in urine or CMV PCR (+) in blood (≤ 2 wk) | Not described | No data | No data |
| Chiavarini et al.34 | GA < 32 wk, birth weight < 2,000 g with CMV-seropositive mother | Italy | PCR | PCR (urine) | CMV PCR (+) in cord blood and Guthrie card, and urine PCR performed at 1 wk | The infant infected by CMV was born by Cesarean section | No data | Frozen BM |
| Hayashi et al.46 | GA < 28 wk, birth weight < 1,000g | Japan | PCR | PCR (urine, blood) | CMV PCR (+) in urine or blood (≤ 1 wk) | DNA sequencing | CMV-seronegative | Frozen BM |
| Wakabayashi et al.25 | Birth weight < 1,500 g | Japan | PCR | PCR (urine) | CMV PCR (+) in urine (≤ 1 wk) | Not described | No data | Fresh or frozen BM |
| Narvaez-Arzate et al.27 | Mean GA 33.8 wk, mean birth weight 1,810.7 g | Mexico | PCR | PCR (urine) | CMV PCR (+) in urine (≤ 2 wk) | Not described | No transfusion | No data |
| Josephson et al.50 | Birth weight ≤ 1,500 g | USA | PCR | PCR (blood, urine) | CMV PCR (+) in urine or blood (≤ 2 wk) | Not described | Leukocyte-filtered, irradiated & CMV-seronegative | Fresh or frozen BM |
| Omarsdottir et al.47 (control group)a | GW < 28 wk | Sweden | PCR & culture | PCR & culture (urine) | CMV PCR and culture (+) in urine (≤ 3 wk) | Not described | Leukocyte-filtered, irradiated | Fresh BM |
| Omarsdottir et al.47 (intervention group)a | GW < 28 wk | Sweden | PCR & culture | PCR & culture (urine) | CMV PCR and culture (+) in urine (≤ 3 wk) | Not described | Leukocyte-filtered, irradiated | Frozen BM |
| Romero-Gómez et al.26 | GA < 32 wk | Spain | PCR & culture | PCR & culture (urine) | CMV PCR and culture (+) in urine (at 3 days) | Not described | Leukocyte-filtered, irradiated | Fresh or frozen BM |
| Hosseini et al.31 | GA < 32 wk, birth weight < 2,000 g | Iran | PCR | PCR (urine) | No data | DNS sequencing | No data | Frozen BM |
GA = gestational age at birth, GW = gestational week, PCR = polymerase chain reaction, CMV = cytomegalovirus, BM = breast milk.
aBoth data from originated from single study47 divided into two studies by breast milk preparation method in this table.
![]()
The results of pooled meta-analysis
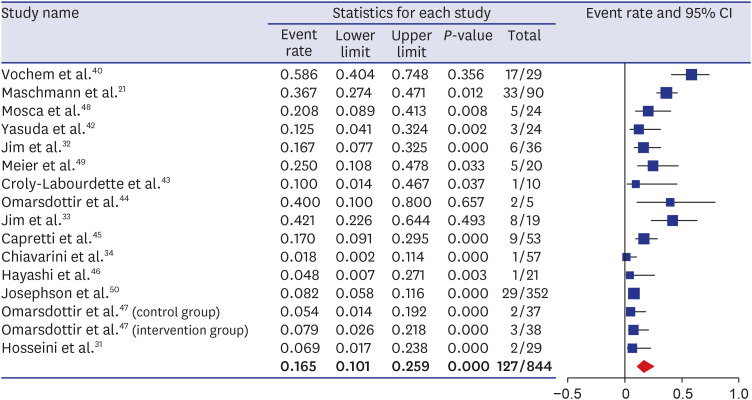
In the analysis, 15 studies reported the CMV serology status of mothers, and 4 did not.25262728 The overall CMV infection rate among infants born to CMV-seropositive mothers was 16.5% (95% confidence interval [CI], 0.10–0.26; P < 0.001) (Fig. 2) using a random effect model. With respect to breast milk preparation method, the acquired infection rate was 25.9% (95% CI, 0.14–0.42; P = 0.005) in infants fed fresh breast milk, 8.2% (95% CI, 0.06–0.12; P < 0.001) in those on a combined diet of fresh and freeze–thawed breast milk, 11.1% (95% CI, 0.05–0.23; P < 0.001) in those receiving freeze–thawed breast milk, and 20.8% (95% CI, 0.09–0.41; P = 0.008) among those for whom no information was available on breast milk preparation (Supplementary Fig. 1). Although heterogeneity among the included studies was detected (P < 0.001; I2 = 83.6%), a sensitivity analysis showed stable results without significant changes after removing any of the studies. No evidence of publication bias was found in the funnel plot (Supplementary Fig. 2) or indicated by either the Begg–Mazumdar rank correlation (P = 0.22) or Egger's regression test (P = 0.61). In the mixed effects analysis, the rate of postnatally acquired CMV infection among breastfed infants with CMV-seropositive mothers differed significantly among groups according to breast milk preparation method (P = 0.005) as follows; fresh breast milk (seven studies, point estimate = 0.259), a combined diet of fresh and freeze–thawed breast milk (one study, point estimate = 0.082), and freeze–thawed breast milk (seven studies, point estimate = 0.111). A sensitivity analysis using sequential exclusion of individual studies (Supplementary Fig. 3) and a cumulative study that added each study (Supplementary Fig. 4) showed no significant changes in the results. No evidence of publication bias was found in the inspection of the funnel plot, and the Begg–Mazumdar rank correlation test (P = 0.46) and Egger's regression test (P = 0.64) did not show evidence of publication bias.
Among 844 CMV-seropositive mothers, the CMV status of breast milk was determined for 773; CMV was detected in breast milk of 590 mothers. Among CMV-seropositive mothers, the rate of CMV shedding into breast milk was 39.6%–100%25262728; four studies did not report the CMV serology of mothers. In the meta-analysis of 15 studies reporting the mothers' CMV status, the overall rate of CMV shedding into breast milk among CMV-seropositive mothers was 80.5% (95% CI, 0.71–0.87; P < 0.001) (Supplementary Fig. 5). Heterogeneity was found across the studies (P < 0.001; I2 = 82.9%) and a random effects model was used for meta-analysis. The funnel plot showed asymmetry (Supplementary Fig. 6), but the Begg–Mazumdar rank correlation test (P = 0.052) and Egger's regression test (P = 0.059) did not show evidence of publication bias.
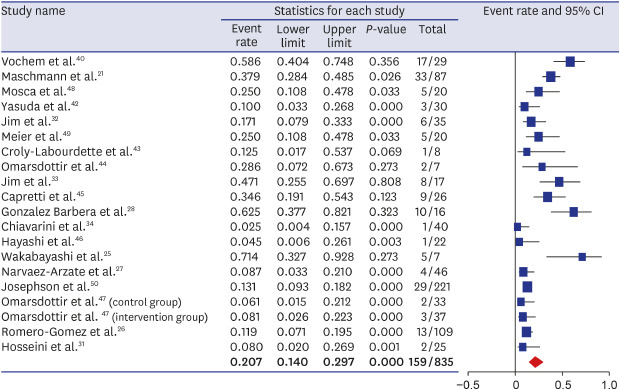
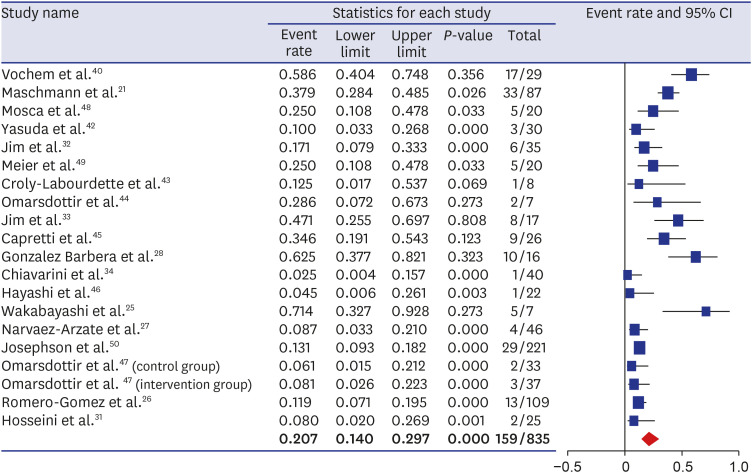
Of a total of 835 infants exposed to CMV-positive breast milk, 159 in the 19 studies acquired CMV infections. Among infants fed CMV-positive breast milk, overall, 20.7% (95% CI, 0.14–0.30; P < 0.001) acquired CMV infections (Fig. 3). By preparation method, the acquired infection rate was 30.3% (95% CI, 0.19–0.45; P = 0.009) in infants fed fresh breast milk, 19.9% (95% CI, 0.09–0.39; P = 0.004) in those receiving a combined diet of fresh and freeze–thawed breast milk, 11.6% (95% CI, 0.05–0.24; P < 0.001) in those receiving freeze–thawed breast milk, and 27.3% (95% CI, 0.07–0.66; P = 0.24) among those where no data on preparation were available (Supplementary Fig. 7). Heterogeneity across the studies was present (P < 0.001; I2 = 81.0%), and a random effects model was used for meta-analysis.
Results of the quality assessment of the included studies, performed using the checklist for prevalence studies from the Joanna Briggs Institute (Munn et al.24), are presented in Table 2.
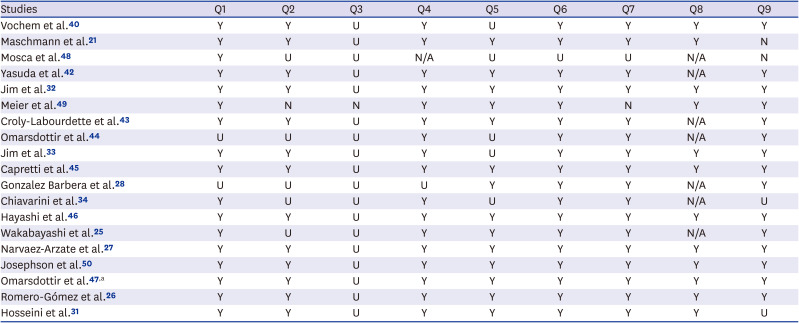
Table 2
Quality assessment of included studies reporting prevalence data
| Studies | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 |
|---|---|---|---|---|---|---|---|---|---|
| Vochem et al.40 | Y | Y | U | Y | U | Y | Y | Y | Y |
| Maschmann et al.21 | Y | Y | U | Y | Y | Y | Y | Y | N |
| Mosca et al.48 | Y | U | U | N/A | U | U | U | N/A | N |
| Yasuda et al.42 | Y | Y | U | Y | Y | Y | Y | N/A | Y |
| Jim et al.32 | Y | Y | U | Y | Y | Y | Y | Y | Y |
| Meier et al.49 | Y | N | N | Y | Y | Y | N | Y | Y |
| Croly-Labourdette et al.43 | Y | Y | U | Y | Y | Y | Y | N/A | Y |
| Omarsdottir et al.44 | U | U | U | Y | U | Y | Y | N/A | Y |
| Jim et al.33 | Y | Y | U | Y | U | Y | Y | Y | Y |
| Capretti et al.45 | Y | Y | U | Y | Y | Y | Y | Y | Y |
| Gonzalez Barbera et al.28 | U | U | U | U | Y | Y | Y | N/A | Y |
| Chiavarini et al.34 | Y | U | U | Y | U | Y | Y | N/A | U |
| Hayashi et al.46 | Y | Y | U | Y | Y | Y | Y | Y | Y |
| Wakabayashi et al.25 | Y | U | U | Y | Y | Y | Y | N/A | Y |
| Narvaez-Arzate et al.27 | Y | Y | U | Y | Y | Y | Y | Y | Y |
| Josephson et al.50 | Y | Y | U | Y | Y | Y | Y | Y | Y |
| Omarsdottir et al.47,a | Y | Y | U | Y | Y | Y | Y | Y | Y |
| Romero-Gómez et al.26 | Y | Y | U | Y | Y | Y | Y | Y | Y |
| Hosseini et al.31 | Y | Y | U | Y | Y | Y | Y | Y | U |
Q = question, Y = yes, N = no, U = unclear, N/A = not applicable.
aThis study included control group and intervention group.
![]()
DISCUSSION
Routes of CMV infection in neonates, in addition to congenital acquisition from primary maternal infection, include postnatal infections from aspiration of contaminated secretions in the birth canal and exposure to infected breast milk or blood products.123 The transmission rate of CMV has been reported as 0.4%–2.5% by congenital infections and 11.1% via postnatal routes.2729 Among the latter infections, approximately 40% may be acquired through breastfeeding, while 30% of postnatal infections stem from other exposures, such as from saliva or urine.30
Breast milk-acquired CMV infection were diagnosed after the exclusion of other possible causes such as congenital infection, infection during delivery, or horizontal infection after delivery including transfusion.17 Congenital CMV infection (i.e., a positive result within 3 weeks after birth) or infection during delivery (i.e., a positive result in the analysis of swabs from the baby's body surface) was ruled out in all but one study (Table 1).31 Transfusion-associated CMV infection was ruled out in all but six studies,252831323334 as shown in Table 1.
Diosi et al.35 first reported the isolation of CMV from human milk and the association of acquired CMV infections in neonates with virus shedding into breast milk. Breastfeeding increased the risk of CMV acquisition by 1.6 fold over formula feeding.30 Reported rates of acquired CMV infection in breast-fed infants varied widely, from 5.7% to 60%.3637 By gestational age, the rate of CMV infection was higher in extreme preterm infants than in more mature infants (57.1% in those born after 23–24 weeks gestation, 17.1% at 25–26 weeks, 15.2% at 27–28 weeks, and 7.1% at 29–30 weeks).38
Postnatal CMV infection is generally not symptomatic due to maternal antibody transfer across the placenta to the fetus,1 but extremely immature or very low-birth-weight infants with immature immunity and insufficient maternal antibody can suffer severe morbidity and mortality.9 In particular, preterm infants born at gestational ages < 30 weeks39 or < 28 weeks15 and/or at birth weights < 1,000 g are at greater risk of symptomatic CMV infection through breast milk.15 Symptomatic or severe CMV infection was reported in 0–35% (median, 3.7%) of very low birth weight (VLBW) infants or preterm infants.3637 In one report,15 severe breast milk-acquired CMV infections developed between the 15th and 70th postnatal day in preterm infants born after 25–33 weeks of gestation. In very low-birth-weight infants, acquired CMV infection can present with sepsis-like symptoms necessitating prolonged hospital stays, including apnea with bradycardia, pneumonia, hepatitis/cholestasis, hepatosplenomegaly, lymph node swelling, neutropenia, thrombocytopenia, elevated liver enzymes, and gastrointestinal symptoms ranging from enteral feeding intolerance to necrotizing enterocolitis.181920374041In the present analysis, 13 studies,21263132333440424344454647 including that by Omarsdottir et al.,47 described the included patients as preterm, and another 6 studies252728484950 described their study populations as having a mean gestational age of either 27.8–33.8 or 28–30.4 weeks or as having birth weights ≤ 1,500 g. Except the study by Meier et al.49 ranged 24 to 33 weeks of gestation, we performed subgroup analysis in clearly defined study population as premature infants and unclearly defined as premature infants. In meta-regression analysis, there is no differences between two groups (data not shown) in the rate of postnatal acquired CMV infection among breastfed infants with CMV-seropositive mothers (P = 0.492) and the rate of breast milk-acquired CMV infection among infants fed CMV-positive breast milk (P = 0.132).
We found that postnatally acquired CMV infection occurred in 25.9% of breastfed infants with CMV-seropositive mothers, if the breast milk was consumed fresh, 8.2% if in a combined diet of fresh and freeze–thawed breast milk, and 11.1% if freeze–thawed. In the study by Lanzieri et al.,10 the rates of acquired CMV infection in infants born to CMV-seropositive mothers was 19% (11%–32%) in the untreated breast milk group and 13% (7%–24%) in the frozen breast milk group.10
In the 2012 guidelines from AAP, fresh breast milk was recommended for all preterm and term infants. Even if there is the possibility of clinical deterioration in very low-birth-weight infants, such as late onset of a sepsis-like syndrome after acquiring CMV infection through breast milk, there is no evidence of long-term neurodevelopmental impairment after acquired CMV infection.12 However, the results of long-term outcome data in preterm infants with breast milk-acquired CMV infections are inconsistent, ranging from no differences in neurodevelopmental outcome or growth status relative to uninfected controls29323451525354555657 to poor neurodevelopmental outcomes, including hearing loss, after CMV infection.18415859
Enteral feeding protocols for infants born to CMV-seropositive mothers after less than 32 weeks of gestation or with birth weights of 1,500 g or less vary from region to region. Responses to a questionnaire on enteral feeding protocols in Swiss, German, and Austrian neonatal intensive care unit (NICUs) indicated that breast milk was administered after short-term or long-term pasteurization, after freeze–thawing, or fresh and untreated.13 Since 2005 in France, unpasteurized breast milk has not been recommended for preterm infants born to CMV-positive mothers if the infants weigh 1,500 g or less, or if they were born at or before 32 weeks' gestation.15 However, these guidelines are difficult to follow in practice owing to the lack of routine CMV screening of pregnant women and the limited availability of breast milk pasteurization in NICUs.15 The California Perinatal Quality Care Collaborative recommended that, until 32 weeks of gestation, the breast milk of CMV-positive mothers may either be fed after freezing for at least 24 hours or be left untreated during breastfeeding.14 The practice of breast milk preparation for preterm infants to prevent CMV infection varies among facilities and among countries.1315 However, pasteurization of breast milk is recommended for preterm infant with body weights ≤ 1,500 g or gestational age ≤ 32 weeks in France15 and for all infants of CMV-seropositive mothers younger than gestational age 34 weeks in Austria.25
CMV is reactivated during lactation in up to 70%–95% of CMV-seropositive mothers; CMV shedding into breast milk is observed in 67%–92% of CMV-positive mothers and in 40%–70% of all mothers.3449506061 CMV reactivation in the postpartum period may be caused by the suppression of cellular immunity, but low levels of CMV DNA may not be observed soon after birth due to the presence of CMV-neutralizing or -inhibiting IgA antibody, tumor necrosis factor-α, interferon-γ, and lactoferrin in colostrum.626364 Although the mechanism of CMV shedding that leads to acquired CMV infection via breast milk is not fully understood, infected cell lysis or viral release from mammary epithelial cells are believed to contribute.6566 Postpartum CMV shedding into whey occurred as a cell-free virus rather than as cell-associated forms in breast milk.63 Viral shedding into breast milk is usually observed between the time of birth (as early as postpartum day 3) and 6–12 weeks, peaking between 4 and 8 weeks postpartum.345060616768 CMV shedding into breast milk was observed in 80.5% (range from 71%–87%) of CMV-seropositive mothers in this study. This result was comparable to a previous report and lower than that of Meier et al.49 (95% in CMV-seropositive mothers).
In previous reports, the rate of CMV transmission to infants through CMV-positive breast milk was 58%–69% for term infants and 38% for preterm infants with birthweights of 1,500 g or less.2969 In this study, the CMV infection rate among infants fed CMV-positive breast milk was approximately 21% (range 14%–30%), and was as high as 30% in infants fed fresh breast milk. The incidence of CMV infection among infants fed CMV-positive breast milk was reported to be 15.3% at 12 weeks after birth in the study by Josephson et al.50 and 37% in the study by Meier et al.49 In the latter study, the different incidence of infection may be due to differences in preparation processes (Table 1).
Various preparation methods; to eradicate CMV have been reported recently, including freezing, pasteurization, microwave irradiation, and ultraviolet-C irradiation.7071 The viral load of CMV in milk can be reduced by freezing but CMV was not eradicated by freezing and could be detected by polymerase chain reaction (PCR) or in cultures.3134727374 However, the CMV viral loads estimated from by DNA PCR tests include non-replicable particles, which are not associated with high infectivity or transmission.75 Moreover, freezing at −20°C for more than 3 days reduced CMV infectivity and titers by 85%–99%. 3134727376 Pasteurization methods, including low temperature long-term pasteurization (30 minutes at 62.5°C), and high temperature short-term pasteurization (5 seconds at 72°C), are highly effective for viral inactivation. Short-term pasteurization was effective for both viral inactivation and preservation of nutritional or immunological contents in breast milk,77 but long-term pasteurization did not completely preserve the nutritional constituents or immunological factors in the milk.123977 In addition, a high power microwave irradiation (750 watts) entirely eradicated CMV in breast milk, whereas low-power microwave irradiation resulted in a 13% failure rate.70 Other effects of microwave treatment on breast milk are unknown, so further studies are needed. Ultraviolet-C irradiation was effective for both the inactivation of CMV and preservation of bioactive factors.71
CMV may be transmitted via breast milk, but breast milk has numerous advantages for premature infants or VLBW infants.78 In previous reports, the incidence of CMV infection among infants fed fresh breast milk was 40%, compared with 8%–15% among infants fed freeze–thawed milk and 0% among infants fed pasteurized breast milk.3751 We also found a lower incidence of CMV infection among infants fed freeze–thawed breast milk than among infants fed fresh breast milk. Based on the results of this study, we cautiously suggest that freeze–thawed breast milk or pasteurized breast milk, rather than fresh breast milk, could be fed to preterm and VLBW infants to avoid symptomatic CMV infection by CMV transmission.
There were some limitations that need to be addressed in the present study. First, five studies2527284850 including the study by Meier et al.49 ranged 24 to 33 weeks of gestation, described their study populations in terms of mean gestational age or birth weight, including preterm infants. Second, all included studies (except for one47) were observational in nature. Well-designed, randomized controlled trials are required to evaluate the exact incidence of breast milk-acquired CMV infection in preterm infants born to CMV-seropositive mothers. Third, given the limitations of meta-analyses, we assumed that CMV was acquired via breast milk. We could not completely exclude the possibility of postnatal CMV infection via routes other than breast milk-acquired CMV infection. However, we extracted the methods used in various studies to distinguish congenital from postnatal CMV infection after a thorough survey of the literature. Information on possible CMV infection via other routes (e.g., aspiration of vaginal secretions, or via transfusion) is included in Table 1. Moreover, we did not examine the long-term outcomes of breast milk-acquired CMV infection. However, eight studies included in our analysis were published after the meta-analysis by Lanzieri et al.10 There remains no consensus, and freezing or pasteurization of breast milk is still recommended in many countries, even after the 2012 AAP recommendations, to prevent CMV infection in preterm infants of < 32 weeks' gestation and/or < 1,500 g. Symptomatic or severe CMV infections have been reported from breast milk-acquired infections in preterm infants. Thus, further study of the short- and long-term prognosis for neonates who have acquired CMV infection via fresh breast milk is needed.
This meta-analysis found that the rate of postnatally acquired CMV infection among breastfed infants with CMV-seropositive mothers was higher in preterm infants fed fresh breast milk. Poor long-term outcomes and symptomatic infections in preterm infants with breast milk-acquired CMV infection has been reported in extreme preterm infants since the 2012 AAP recommendations. Further studies are needed to re-evaluate the long-term prognosis after breast milk-acquired CMV infection, especially in extreme preterm infants, and to refine recommendations based on those results. Currently, pasteurization is the safest method by which to prevent CMV infection via breast milk; however, it is not easy to use pasteurized breast milk in Korean NICUs. Therefore, we cautiously suggest that freeze–thawed breast milk, not fresh breast milk, should be given to preterm or VLBW infants until further data are available.
 XML Download
XML Download