

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
Spinal cord injury (SCI) is a serious clinical condition that impacts a patient’s physical, psychological and socio-economic status.12 The annual incidence of SCI is 26.4 cases per million in Korea, and ranges from 8 to 49.1 per million in other countries worldwide.34 Neurologic symptoms of SCI, such as loss of motor function, sensory impairment, and neuropathic pain, undermine the patient's health-related quality of life. Furthermore, several physiological changes contribute to bowel and bladder dysfunction, spasticity, and impaired respiratory function in chronic SCI patients.5
Generally, there is little improvement in paraplegia secondary to SCI over the year following the initial injury.6 As a consequence, chronic SCI patients are forced to be inactive and have a sedentary lifestyle, resulting in various secondary medical complications, such as cardiovascular and metabolic diseases. It has been reported that immobilization of SCI patients results in a loss of bone mineral density (BMD) and thus leads to osteoporosis.7 Moreover, decreased bone density of the femoral neck is associated with an increased risk of fractures in SCI patients.8 Systematic inflammation is also reported to be a secondary complication related to physical inactivity in chronic SCI patients.9
Various methods are currently being applied to improve functional mobility and better manage paraplegia in SCI patients. Wheelchairs are widely used for ambulation in SCI patients, but have some disadvantages given bipedal ambulation is impossible and the wheelchair only allows movement on flat surfaces. In the past, knee-ankle-foot orthosis (KAFO) was employed to aid bipedal ambulation; however, KAFO proved difficult to utilize for SCI patients with hip muscle strength less than grade 3, and required greater energy expenditure compared with wheelchair ambulation; due to a lack of practical advantages, KAFO was not widely adopted by SCI patients.1011
In order to achieve bipedal ambulation and increase physical activity in SCI patients, several wearable powered exoskeletons have been developed for SCI patients over the last decade. These include, the ReWalk (ReWalk Robotics, Inc., Marlborough, MA, USA), Ekso (Ekso Bionics, Richmond, CA, USA), HAL (Cyberdyne Inc., Tsukuba, Japan), and Indego (Parker Hannifin Corp., Cleveland, OH, USA) devices.1213141516
These wearable powered exoskeletons are able to perform various movements controlled by motors located bilaterally at the hip and knee joints.12131415 When using ReWalk, Ekso, and Indego, patients initiate walking using forward/backward trunk motion and by shifting their center of pressure.121315 In the HAL exoskeleton, ambulation is controlled by electromyographic signals received from the lower extremity muscles.14
Clinical effects on SCI patients and the safety of these exoskeletons have been reported in many studies.12131415171819202122 Recently, the safety and feasibility of exoskeleton-assisted walking (EAW) was verified even in acute SCI patients.23 The Hyundai Medical Exoskeleton (H-MEX; Hyundai Motor Company, Uiwang, Korea) is a newly developed wearable powered exoskeleton robot that enables bipedal ambulation in SCI patients.24 In this study, we assessed the feasibility of H-MEX training, and verified its suitability for use by SCI patients.
The aim of this study was to evaluate the effects of H-MEX training on functional mobility, physiological condition, and quality of life in non-ambulatory SCI patients. The feasibility and safety of H-MEX training were assessed during the study. The hypothesis was that H-MEX training is feasible and safe in chronic SCI patients, and improves functional mobility, physiological condition and quality of life.
METHODS
This was a prospective, single-center, single-group pilot study. Non-ambulatory patients with SCI were recruited from August 2019 to December 2019. The inclusion criteria were 1) chronic neurologically stable non-ambulatory SCI of at least 2 months duration 2) height between 1.6 m and 1.8 m, 3) weight less than 100 kg, 4) sufficient postural stability to sit independently, 5) ability to transfer from wheelchair to bed independently, 6) sufficient bilateral upper extremity strength to manage crutches, and 7) sufficiently alert mental status to follow the researchers’ instructions.
The exclusion criteria were 1) unable to bear weight, for example due to spinal instability or unhealed bone fracture in the lower extremities, 2) severe lower extremity spasticity exceeding Modified Ashworth Scale (MAS) grade 3, 3) severe joint contracture in the lower extremities, 4) skin problems such as pressure ulcers at the contact area of the device, 5) functional impairment of the upper extremities due to motor weakness or contracture, 6) severe osteoporosis with high fracture risk, 7) deep vein thrombosis, 8) uncontrolled hypertension or hypotension, 9) psychiatric or cognitive problems that could interfere with the trial, and 10) lack of informed consent.
Before initiation of training, all participants were evaluated by a physiatrist to identify their ability to participate, and classified according to the American Spinal Injury Association Impairment Scale (AIS). Muscle strength, sitting balance, height, weight, neurological level of injury (NLI), and time since injury were recorded. An electrocardiogram and spinal radiograph were obtained to screen the participant's general medical condition.
Exoskeleton (H-MEX)
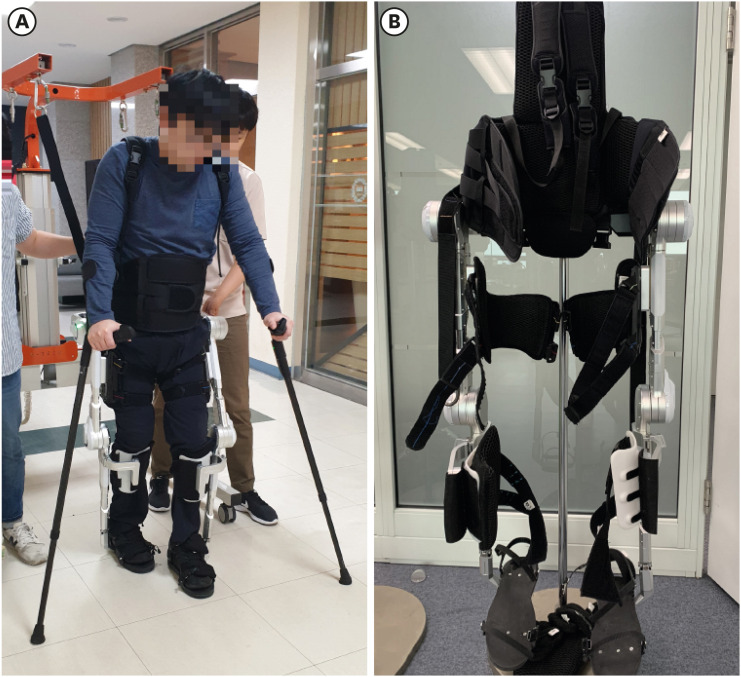
The H-MEX is an exoskeleton designed for non-ambulatory patients to regain independent ambulation (Fig. 1A and B). This exoskeleton consists of a motherboard, bilateral pelvic actuators (range of motion: −30° to 30°), hip actuators (range of motion: −30° to 150°), knee actuators (range of motion: −5° to 150°), and passive ankle joints.24 Rechargeable lithium ion batteries supply power to the pelvic, hip and knee actuators and allow the H-MEX to operate for 2 consecutive hours. The total device weight of the H-MEX is less than 19 kg.
Fig. 1
The H-MEX wearable powered exoskeleton (A) worn by the participant and (B) after takeoff.
H-MEX = Hyundai Medical Exoskeleton.
The figures are published under agreement of the patient.
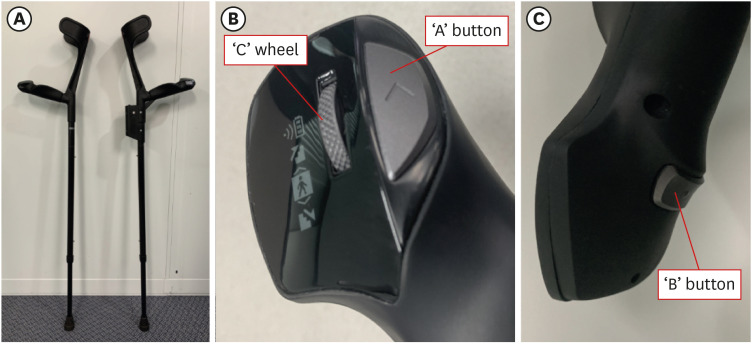
A pair of crutches were also supplied to improve the participant's balance and forward support (Fig. 2A). The postures and motions of the H-MEX are controlled by two buttons (A, B) and one scroll wheel (C) on the left crutch (Fig. 2B and C). The ‘C’ scroll wheel is used to select the gait mode: the participant can select modes for standing, sitting, walking, climbing stairs or descending stairs. The initial state is the sitting mode, which is converted to the standing mode by scrolling the ‘C’ wheel and pressing the ‘A’ button. In the standing mode, ground reaction forces on both feet are estimated by four optic force sensors placed on each foot plate.24 Forces of both feet are compared by the main controller and the foot with the higher value is set as the leading leg. The user then presses the ‘A’ button again, and right or left forward movement begins and consequently triggers bipedal gait. Continuous ambulation occurs if the participant keeps pressing the ‘A’ button. After ambulation, participants can gather both legs together into a standing posture by pressing the ‘B’ button. Moreover, participants can sit in a chair by scrolling the ‘C’ wheel to change the mode and pressing the ‘A’ button. As a result, participants can control their overall gait through just two buttons and one scroll wheel on the crutch.
Training sessions
All participants had 30 sessions of gait training with the H-MEX. The training program consisted of training periods of 60 minutes duration, 3 times per week, over 10 weeks. The training site was a flat indoor floor, and the overall width was about 20 m. Prior to the start of the 30 training sessions, participants were provided basic information regarding how to operate and wear the H-MEX. The device was adjusted to each participant's thigh/shank lengths. Each training session consisted of standing up from sitting on a chair, walking across a flat floor, and sitting down on a chair.
All training sessions were conducted under the supervision of the researchers. For the safety of participants, an overhead harness system (LG-1000; NEO-TECH, Gimpo, Korea) was connected to the posterior side of the H-MEX to prevent falls. The harness was loosely connected to the H-MEX and did not support the weight of the H-MEX or participants.
Measurements
To assess the functional outcomes of non-ambulatory SCI patients after training with the H-MEX, the 6-minute walking test (6MWT) and timed-up-and-go test (TUGT) were performed. The 6MWT was conducted by measuring the distance that a participant was able to cover while walking continuously for 6 minutes. The TUGT results included the estimated time required to 1) stand up from sitting in a chair, 2) walk forward 3 m, 3) turn around, 4) walk 3 m backward, and 5) sit down in the chair again. The 6MWT and TUGT were performed at initiation (pre-training), after 15 sessions (mid-training), and after 30 sessions (post-training); however, given that participants needed the time to adjust to the device, the pre-training values were measured after 1 to 3 training sessions.
The physiological outcomes of H-MEX training were evaluated by assessing spasticity, pulmonary function, BMD, colon transit time, and inflammatory serum markers. These parameters were evaluated before training (pre-training) and within 1 week after finishing 30 training sessions (post-training). Spasticity was measured bilaterally in the knee flexor, knee extensor, ankle dorsiflexor, and ankle plantar flexor muscles. The MAS was used to score spasticity. Pulmonary function testing (PFT) was performed using spirometry (MasterScreen-Pneumo, Jaeger, Germany) to evaluate the participant's forced expiratory volume in 1 second (FEV1, L), forced vital capacity (FVC, L), and the FEV1/FVC ratio (%). Dual energy X-ray absorptiometry was performed on the femoral necks bilaterally and BMD was calculated using a bone densitometer (Hologic QDR 4500; Integrity Medical, Fort Myers, FL, USA). Inflammation was assessed by measuring serum C-reactive protein (CRP) concentrations, the erythrocyte sedimentation rate (ESR) and white blood cell (WBC). To evaluate the bowel function of participants, a colon transit time test was carried out as follows: 1) twenty radio-opaque markers (Kolomark; M.I.Tech, Pyeongtaek, Korea) were given by oral administration to participants, 2) a simple abdominal radiograph was obtained on the seventh day, and 3) the number of retained radio-opaque markers was counted. If the marker remained on the follow-up radiograph, the participant was considered to have delayed colon transit time.
Additional subjective outcome measures were also evaluated. To assess the fear of falling among the participants, the Korean version of the Falls Efficacy Scale-International (KFES-I) was used. The KFES-I was calculated by summing responses (ranging from 1 to 4 points) for each of 16 questions, to give total scores ranging from 16 to 64 points. The 36-Item Short-Form Health Survey version 2 (SF-36v2) was used to assess health-related quality of life, and was divided into 8 subscales: physical functioning, role limitations due to physical problems (RP), body pain (BP), general medical health (GH), vitality (VT), social functioning (SF), role limitations due to emotional problems (RE), and general mental health (MH). The above questionnaires were evaluated before and after 30 training sessions.
Statistical analyses
In this study, statistical analyses were performed using SPSS® for Windows version 25 (IBM/SPSS Inc., Armonk, NY, USA). Mean and standard deviation values were used as descriptive statistics for demographical data and outcome measurements. The outcomes of the 6MWT and TUGT were assessed by the Friedman test, and compared the pre-, mid-, and post-training values. If statistical significance (P < 0.05) was found, post hoc analyses were conducted using Wilcoxon signed-rank tests with Bonferroni correction (adjusting the P value for multiple comparisons, P ≤ 0.017). Differences between physiological and subjective outcome measurements pre- and post-training were analyzed using the Wilcoxon signed-rank test. These results were considered statistically significant if the P value was less than 0.05.
Ethics statement
This study was approved by the Institutional Review Board (IRB) at the Hanyang Medical Center (IRB File No. 2017-01-050) and all experimentation was conducted in conformity with ethical and humane principles of research. The trial protocol of the study was registered on ClinicalTrials.gov (Identifier: NCT04055610). All participants provided signed informed consent prior to enrollment.
RESULTS
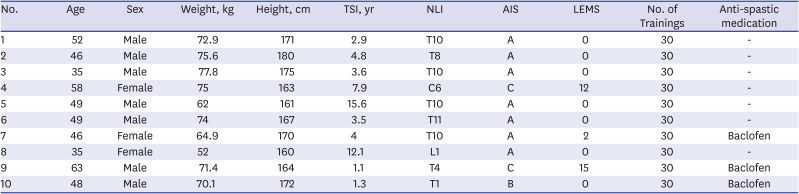
Of 19 patients with SCI who were screened, 11 participants were enrolled in the study. One eligible participant dropped out of the study due to personal reasons (scheduling conflicts), and 10 participants completed the training program. The participants ranged in age from 35 to 63 years, weighed between 52 to 77.8 kg, were between 1.61 to 1.80 m in height, and the time since their injury ranged from 1.1 to 15.6 years (Table 1). Among 10 participants, 8 were motor-complete SCI (AIS A or B) and 2 were motor-incomplete (AIS C). These 2 AIS C participants had insufficient lower extremity strength (lower extremity muscle grade ≤ 2 of 5) and they could ambulate only with a wheelchair. All participants had intact upper extremity muscle strength except one with NLI C6 (participant number 4). However, she had sufficient upper extremity strength (upper extremity muscle grade ≥ 4 of 5) to manipulate the H-MEX clutches and there were no difficulties with EAW training. There were no electrocardiogram abnormalities among the participants.
Table 1
Participant demographics
Ambulatory function
All participants demonstrated significant improvement in the 6MWT after using the H-MEX (χ2 = 18.200, P = 0.00; Table 2). After training, the mean distance achieved during the 6MWT (49.13 ± 15.22 m) was significantly enhanced compared with baseline (20.65 ± 5.55; Z = −2.805, P = 0.005). Statistically significant improvement between the pre- and mid-training assessment (Z = −2.805, P = 0.005), and between the mid-training and post-training assessment (Z = −2.448, P = 0.014) were also reported (Fig. 3A).
Table 2
Ambulatory function outcomes

Fig. 3
Functional mobility parameters pre-, mid-, and post-training; (A) Distance achieved in 6 minute walking test; (B) time to complete the first 3 m walk in the TUGT; (C) time to come to standing in the TUGT; (D) time spent sitting in the TUGT.
PN = participant number, TUGT = timed-up-and-go test.
aStatistically significant difference compared with pre-training, P < 0.017; bStatistically significant difference compared with mid-training, P < 0.017.
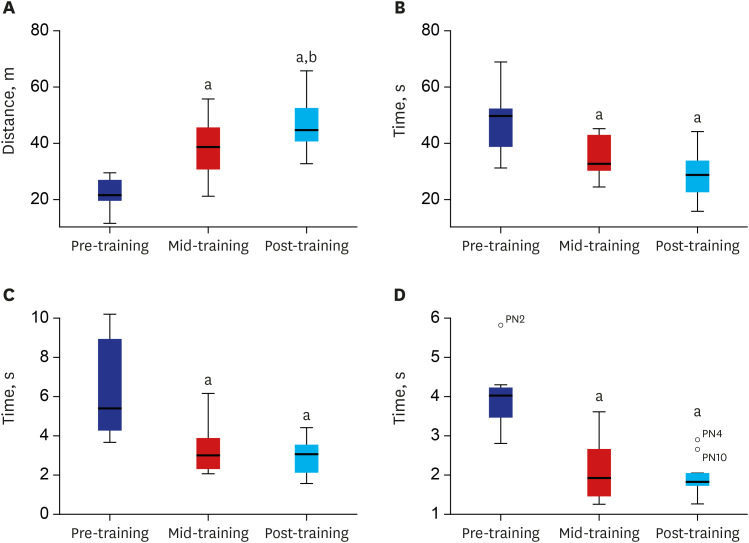
In the baseline TUGT, some participants had difficulty in turning when wearing the H-MEX. As a result, the time required to stand up from the chair, walk 3 m forward, and sit down in the chair were used for the data analysis (Table 2). Statistically significant differences were reported in the TUGT 3 m walk depending on the number of training sessions (χ2 = 11.400, P = 0.03; Fig. 3B). After training, the mean value for the TUGT 3 m walk (28.45 ± 9.06 seconds) was significantly improved compared with baseline (57.74 ± 39.30; Z = −2.701, P = 0.007). There were also significant improvements between the pre-training and mid-training assessments (Z = −2.395, P = 0.017).
Moreover, statistically significant differences in the time required to stand up (χ2 = 15.436, P = 0.00) and sit down (χ2 = 15.436, P = 0.00), were recorded (Table 2). Significant reductions in the time required to stand up between the pre-training (5.91 ± 2.40 seconds) and mid-training assessments (3.03 ± 1.24; Z = −2.395, P = 0.017) and between pre-training and post-training assessments (2.81 ± 0.89; Z = −2.499, P = 0.012) were noted (Fig. 3C). The time required to sit down was also significantly reduced between the pre-training (3.92 ± 0.83) and mid-training assessments (2.09 ± 0.85; Z = −2.803, P = 0.005) and between the pre-training and post-training assessments (1.91 ± 0.49; Z = −2.803, P = 0.005; Fig. 3D).
Physiological outcomes
There were no significant differences in physiological outcomes between pre- and post-training (Table 3): however, some participants showed non-significant but meaningful changes after H-MEX training.
Table 3
Physiological outcomes
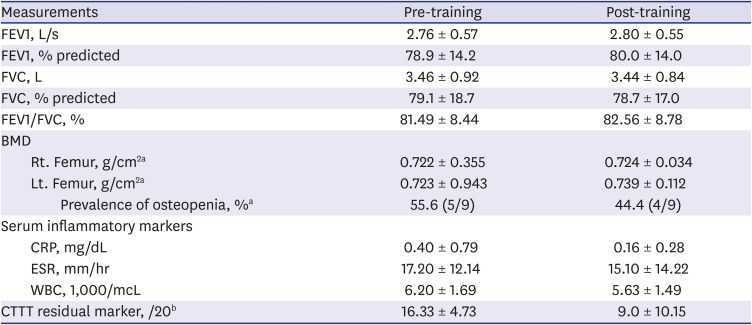
Values are means ± standard deviation.
FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity, BMD = bone mineral density, WBC = white blood cell, CRP = C-reactive protein, ESR = erythrocyte sedimentation rate, CTTT = colon transit time test.
aOne participant was excluded from the calculations due to history of hip arthroplasty; bParticipants without constipation were excluded from the calculations.
Spasticity
Among the 10 participants, 5 had spasticity in the lower extremities. When comparing MAS scores pre- and post-training, 2 participants (participants number 9 and 10) showed improvement and 1 participant (participant number 3) showed mild aggravation of spasticity.
Pulmonary function
At baseline, 6 participants had restrictive ventilator defects (FEV1/FVC ratio > 0.7, and FVC < 80% of predicted) and 1 participant had an obstructive ventilator defect (FEV1/FVC ratio < 0.7). There were no statistically significant differences between the pre- and post-training results with regard to FEV1, FVC or FEV1/FVC (Table 3). However, among the 10 participants, 8 showed improvement in FEV1 after the training program (P = 0.314). One participant with a restrictive ventilator defect (participant number 2) had a 14.6% improvement in FEV1 and 15.7% improvement in FVC.
BMD
One participant was excluded from the BMD calculations due to a history of hip arthroplasty. Among the 9 remaining participants, 5 had osteopenia (T-score between −1.0 to −2.5; Table 3). Although there was no significant difference in the BMD pre- and post-training (left femur: P = 0.674/right femur: P = 1.0), there was improvement of BMD in some participants. Three participants had increased femoral neck BMD bilaterally and 2 participants had unilateral increases. In particular, one participant with osteopenia (participant number 5) had a 13.9% increase in BMD in the right femoral neck and improved his BMD status to a normal state.
Bowel function
Three participants (number 4, 6 and 10) had delayed colon transit times at initiation. Improvement of bowel function after training was identified in 2 among these 3 participants, with the number of retained markers reduced from 20 to 7 in participant number 4, and reduced from 11 to 0 in participant number 10. However, marker retention increased from 18 to 20 in participant number 6.
Serum inflammatory markers
The mean CRP concentrations before and after training were 0.40 ± 0.79 and 0.16 ± 0.28, respectively. The difference was not statistically significant (P = 0.465; Table 3). As for ESR (P = 0.161) and WBC (P = 0.307) level, the difference before and after training was not statistically significant (Table 3).
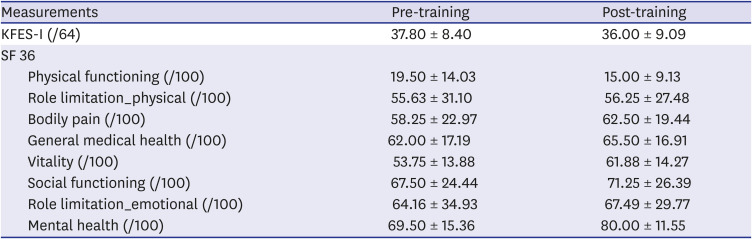
Subjective outcomes
The mean score in the KFES-I questionnaire was reduced post-training (36.00 ± 9.09) compared to pre-training (37.80 ± 8.40), but this result was not statistically significant (P = 0.475; Table 4). The KFES-I score was reduced in 6 participants after training. In the SF-36v2, which was conducted to evaluate the quality of life, the average score increased in 7 of 8 subscales, RP—BP, GH, VT, SF, RE, and MH—but none of these changes were statistically significant (Table 4). With regard to the MH subscale in particular, the scores increased after training in 8 participants, a finding with borderline significance (P = 0.082).
Table 4
Subjective assessment of fear of falling and quality of life
Adverse events
Although each participant completed all 30 sessions of training without reporting a severe adverse event, there were several minor events. Skin abrasions at the skin-contact area for the H-MEX were reported in 2 participants. This problem was managed by applying a thick pad to the area. And there was one near fall during gait training: a plastic buckle on the harness strap which fastened the participant to the H-MEX broke during ambulation, and this caused the participant to lose their balance; however, the overhead harness system prevented a major accident. The breakage of the plastic harness buckle was confirmed to be due to aging of the harness, and this part was immediately replaced. After the replacement, no similar events were reported.
DISCUSSION
In this pilot study, we evaluated the feasibility and safety of H-MEX training, and assessed functional mobility, physiological health outcomes, and responses to subjective questionnaires in SCI patients after training with the H-MEX. With the exception of 1 participant who dropped out mid-study due to personal reasons, all the remaining 10 participants finished 30 sessions of training and could manage the H-MEX independently. Moreover, the participants reported no severe adverse events, such as falls, fractures, or cardiovascular events.
As evaluated by the 6MWT and TUGT, functional mobility of participants was enhanced significantly compared with baseline. Improvements in the functional abilities of SCI patients have also been reported in previous powered exoskeleton studies.12131517182125 Since exoskeleton robots do not improve the lower extremity function of SCI patients, the patient's proficiency is an important factor in enhancement of mobility. In this study, participant's manipulation skill with H-MEX improved as they continued training. However, we could not identify whether the ambulation skill would be more improved even after 10 weeks of EAW.
According to a meta-analysis which analyzed 14 exoskeleton studies, only 76% of patients could succeed to EAW without physical assistance.22 Considering this, it is relatively meaningful that all participants except for one who dropped out of training due to personal reason could ambulate without physical assistance while wearing the H-MEX. Moreover, it implies that the participants in this study had high compliance with using the H-MEX.
Regarding the distance of 6MWT, the average value reported in a meta-analysis was 98 m, which is longer than our study's value (49.13 ± 15.22 m).22 However, the 6MWT result in this study could be thought to be significant for Korean SCI patients, given that the mean value of Kwon's study conducted with Korean patients using the ReWalk was 39.1 ± 5.4 m.26 In fact, there are no EAW studies of racial or national differences at the 6MWT distance.
Several studies reported that EAW training was conducted in outdoor environments.121521 According to Hartigan et al.,15 all participants with SCI were able to walk outdoors while wearing Indego. Benson et al.21 conducted EAW with ReWalk in an outdoor obstacle course that included a gravel section and 8 degrees inclination. In this study, since it was a pilot study about the newly developed H-MEX, EAW in an outdoor environment was not conducted to ensure participant safety. For practical H-MEX use, future outdoor EAW should be considered in further studies of the H-MEX.
The strengths of our study include that we comprehensively evaluated secondary physiological changes in various aspects, in addition to functional mobility. There were some clinically meaningful changes in secondary physiological outcomes although these were not statistically significant. As for spasticity, of the 3 participants who had spasticity during training sessions, 2 participants showed improvement in their MAS scores. This finding may be considered a relatively meaningful change, given the 2 participants reported no changes in the dose of their anti-spastic medication during the study. Reduced spasticity following exoskeleton training in SCI patients has been reported in previous studies.17192728 Mirbagheri et al.29 reported that robotic-assisted gait training in SCI patients reduced spasticity by modulation of intrinsic joint properties and stretch reflex stiffness. The reduction in spasticity in this study might be explained by the fact that the exoskeleton enables chronic SCI patients to perform bipedal ambulation and move through the normal range of motion of multiple lower extremity joints.
Regarding the PFT results, 8 of the 10 participants had increased FEV1 after training. There have been several studies investigating the effects of aerobic exercise on pulmonary function in SCI patients.3031 Soyupek et al.30 evaluated the efficacy of 6 weeks BWSTT in incomplete SCI patients and reported improvements in pulmonary parameters, especially FVC and inspiratory capacity. Aerobic training is an important component of pulmonary rehabilitation, and improvements in PFT parameters in this study may have resulted from aerobic exercise with the H-MEX.32
In non-ambulatory SCI patients, ambulatory dysfunction induces mechanical unloading of the skeletal system, resulting in imbalances between bone formation (typically reduced) and bone resorption (increased).33 To manage bone density reductions in SCI patients, several studies have investigated the effect of powered wearable exoskeletons on BMD. Karelis et al.34 reported that ambulation training with the Ekso in chronic SCI patients improved bone health, with a 14.5% increase in BMD. In this study, although not statistically significant, 5 of 9 participants had increased BMD measurement after the training program and 1 participant converted from osteopenia to normal status. These improvements may have been the result of H-MEX-assisted bipedal ambulation allowing mechanical loading during weight bearing and activation of osteogenesis in the skeletal system of the lower extremities.3536 Ambulation with the aid of an exoskeleton may therefore be beneficial in increasing bone density and may also be helpful to prevent osteoporosis in non-ambulatory SCI patients.
Bowel dysfunction is one of the major complications in SCI patients and the main pathologic mechanism is neuronal disconnection between the spinal cord and the colon.37 However, immobility of SCI patients may be another reason for bowel dysfunction, resulting in delayed colon transit times. Prolonged physical inactivity is correlated with functional constipation, and aerobic exercise such as walking may reduce constipation by increasing colonic motility.383940 Moreover, positive effects of EAW in bowel dysfunction for SCI patients has been reported in previous studies.131741 In the previous study with ReWalk, 5 of 11 participants reported that EAW improved bowel regulation.17 Chun et al.41 found improvement in bowel function in SCI patients after training with the ReWalk, as evaluated by participant responses to questionnaires. These previous studies evaluated bowel function based on participants’ subjective responses. However, we evaluated bowel function using radio-opaque markers, which is a relatively objective and quantitative bowel function evaluation method. In our study, among the 3 participants who had delayed colon transit times at study initiation, 2 participants reported improvement after completing the training sessions. These findings may suggest that ambulation with the H-MEX improved immobility and bowel dysfunction.
In this study, serum inflammatory markers were not elevated enough to suggest chronic inflammation. Different from our result, it was reported that chronic inflammation could be detected in asymptomatic chronic SCI patients and this condition was usually related to pressure ulcers or urinary tract infections.4243 There were other previous reports that chronic systematic inflammation in chronic SCI was correlated with physical inactivity and that inflammatory markers such as CRP and ESR significantly improved in SCI patients after 6 weeks of BWSTT.944 However, in this study, it might be difficult to assume that participants were in a chronic inflammatory status and we could not confirm the improvement of chronic inflammation through EAW.
In this study, the mean score in the KFES-I questionnaire was 37.80 at study initiation, while the mean value in able-bodied people under age 80 has been reported to be 23.97.45 This result indicates that non-ambulatory SCI patients have a greater fear of falling than adults without disability. After 30 sessions of training, participant mean KFES-I score was 36, which was not changed significantly compared to training initiation. Questionnaires for KFES-I consist of variable activities of daily living in indoor and outdoor settings. Because participants did not wear the H-MEX in daily life, it might be difficult to assess the difference in their activities of daily living, which caused little difference in KFES-I scores. However, if the H-MEX should be commercialized and be used by SCI patients in daily life, a decrease in KFES-I score would be expected.
Regarding the SF-36v2 results, non-ambulatory SCI patients had lower scores than healthy people in almost all subscales, except GH.46 With respect to MH, while the mean score was lower than those for healthy people at study initiation, after 30 training sessions the participants’ scores were higher than those in healthy people. The findings of a previous study indicated regular exercise could be used as a therapeutic tool to improve the overall quality of life in SCI patients.47 Moreover, emotional and psychological benefits were reported in SCI patients after EAW.17 In this study, increased mean scores in 7 of 8 subscales were recorded, indicative of increased quality of life. Some participants commented that H-MEX-assisted bipedal ambulation helped them regain confidence as their eye level became similar to that of able-bodied persons. Thus, bipedal ambulation with H-MEX may improve the quality of life and psychological condition of SCI patients.
There were several limitations of our study. First, the sample size was relatively small, and may have resulted in lack of statistical power for some measurements. Therefore, further study with a larger number of participants should be performed to more clearly identify the effects of H-MEX training. Second, the characteristics of the participants were relatively heterogeneous. The NLI ranged from C6 to L1 and the AIS score ranged from A to C. Thus, the results of this pilot study may not be generalizable to SCI patients with motor-complete paraplegia. Further studies that include a more homogenous participant group are needed.
In conclusion, this study demonstrated that the newly developed wearable exoskeleton, H-MEX is safe and feasible for non-ambulatory SCI patients, and may have the potential to improve patient quality of life by assisting bipedal ambulation. These results suggest that the H-MEX can be considered a beneficial device for chronic non-ambulatory SCI patients. Further studies should be conducted with a larger number of participants to more clearly identify the effects of H-MEX training.
 XML Download
XML Download