

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Hemophilia B is a rare hereditary bleeding disorder caused by the deficiency or dysfunction of coagulation factor IX (FIX), resulting in prolonged and uncontrolled bleeding [1, 2]. According to the 2018 annual global survey report of the World Federation of Hemophilia (WFH), 34,289 patients from 124 countries worldwide were reported to have hemophilia B, and of these, 427 patients were from South Korea [3]. The prevalence of hemophilia B in South Korea increased by 17% in 6 years, from 365 patients in 2012 [4] to 427 patients in 2018 [3].
The prevention and treatment of bleeding episodes in patients with hemophilia B are based on the replacement of deficient FIX with plasma-derived (pd) FIX products or recombinant FIX (rFIX) products either prophylactically or on an on-demand basis [5]. The Medical and Scientific Advisory Council of the National Hemophilia Foundation (NHF), WFH, and World Health Organization recommend prophylaxis as optimal therapy for patients with severe hemophilia B [6, 7].
Although treatment with pdFIX products has been in use for years, the risk of transmission of blood-borne pathogens such as non-enveloped viruses is a major concern [8, 9]. In contrast, the use of rFIX products eliminates such a risk of transmission. Furthermore, these products have a better viral safety profile than do pdFIX products because no human or animal plasma-derived proteins are used during their manufacturing process. Over the past few years, several advanced treatment options, including FIX products with extended half-lives, have been approved for the treatment of hemophilia B [10]. However, access to these products remains limited in under-developed countries [11]. Therefore, there is a greater need to increase the worldwide availability of these products to support higher demand and expand treatment options for hemophilia B.
Rixubis (rFIX, nonacog gamma, Baxalta US Inc., Thousand Oaks, CA, USA), a coagulation rFIX product was approved for the prevention and treatment of bleeding episodes and routine prophylaxis in patients with hemophilia B in the United States (2013), Europe (2014), and South Korea (2015). It is currently available in 17 countries worldwide and in the European Union. Previously published studies have reported the safety and efficacy of Rixubis globally in adults and children [12-15]. Because Rixubis has been recently launched in the global market, there is a paucity of published clinical studies evaluating its safety and effectiveness in a real-world scenario as an approved product. Therefore, this postmarketing surveillance (PMS) study aimed to evaluate the real-world safety and effectiveness of Rixubis in adult and pediatric patients with hemophilia B in South Korea.
MATERIALS AND METHODS
Study design and patient population
This multicenter, prospective, observational, PMS study was conducted between April 2015 and April 2019 in adult and pediatric patients with congenital hemophilia B. Patients who consented, in whom the treatment of hemophilia B with Rixubis (according to the Korean product leaflet) was indicated, and who were previously prescribed and newly prescribed Rixubis were considered eligible to participate in the study. The exclusion criteria were as follows: 1) known hypersensitivity or presence of any contraindication to Rixubis or its excipients, including hamster protein, 2) disseminated intravascular coagulation, and 3) signs of fibrinolysis. Following enrollment, information on patients’ demographic and clinical characteristics was collected. The scheduled dose and administration duration of Rixubis were determined based on the degree of FIX deficiency (severity), site and extent of bleeding, patient’s age and clinical conditions, and pharmacokinetic parameters of FIX. The safety and effectiveness data were recorded for each patient by using case report forms filled by the investigators at the study sites. The study was conducted according to Korean regulations and guidelines. The study protocol was reviewed and approved by the institutional review board of each study site.
Safety assessment
Safety was evaluated in terms of the number and incidence of adverse events (AEs) and serious AEs (SAEs), whether related or unrelated to the drug, their severity (mild, moderate, or severe), and outcome. All AEs were categorized by preferred terms according to Medical Dictionary for Regulatory Activities (MedDRA) version 21.1 and categorized as expected or unexpected AE according to the label information in South Korea.
Effectiveness assessment
Effectiveness was evaluated in terms of control and prevention of bleeding episodes in patients with hemophilia B. The hemostatic effectiveness was assessed by physicians and patients for every treatment type (treatment of bleeding, prophylaxis, and surgery and/or perioperative coverage) and classified as “unknown,” “excellent,” “good,” “fair,” and “none.” The overall effectiveness rate was calculated by combining the “good” and “excellent” assessment ratings and expressed as an effective number of assessments or in percentage.
Statistical analysis
All study variables were analyzed using descriptive statistics. Continuous variables are presented as mean and standard deviation (SD) values, and categorical variables are summarized as frequencies and percentages. Data analysis was performed using the SAS software package, version 9.4 (SAS Institute, Cary, NC, USA).
RESULTS
Patient demographic and clinical characteristics
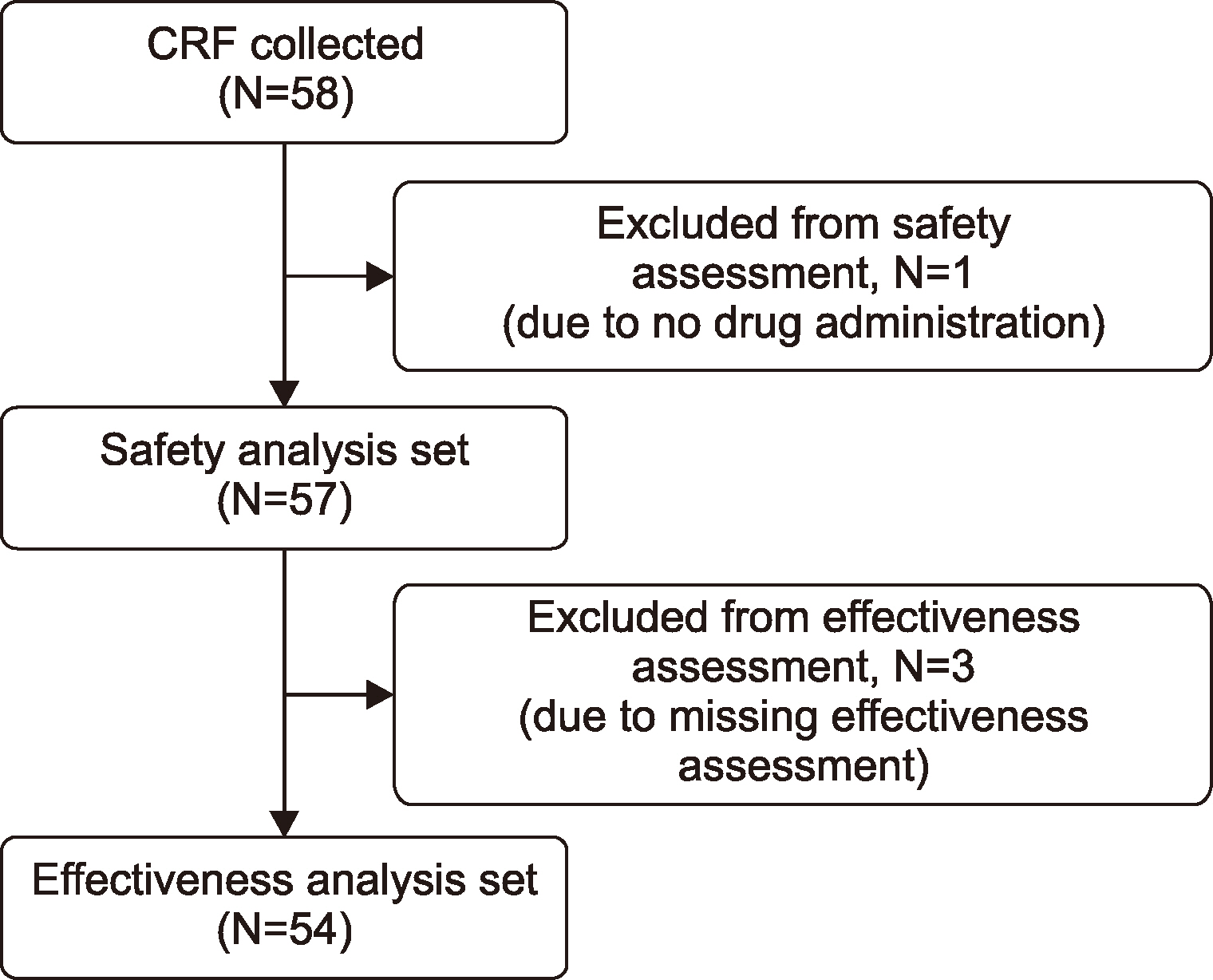
A total of 58 hemophilia patients were recruited at four centers by seven physicians in South Korea between April 2015 and April 2019, who were observed for up to 6 months after the initiation of Rixubis treatment. Of these, 57 (98%) patients (mean age, 34.6±19.0 yr) were included in the safety analysis set (SAS) and 54 (93%) were included in the effectiveness analysis set (EAS) (Fig. 1). The reasons for exclusion from SAS and EAS were no study drug administration (N=1) and missing effectiveness assessment (N=3), respectively. All patients were male and Asian. The mean patient age was 34.6 years, with the majority (77.2%) aged 19 years or higher with a mean body mass index (BMI) of 24.0 kg/m2 (Table 1).
The average disease duration was 18.1 years; 1.8% (1 patient) of the patients had a history of an allergic reaction, 5.3% (3 patients) had a family history of inhibitor development, and no patient had a history of inhibitor development. Most of the patients (N=41) reported minor bleeding, followed by moderate (N=14) and major (N=4) bleeding within the last 12 months. The mean number of episodes of minor, moderate, and major bleeding were 22.4, 2.5, and 1.3, respectively. Additionally, 54 patients (94.7%) used FIX concentrates before treatment with Rixubis. The most reported medical condition was hypertension (7.0%), followed by acquired immunodeficiency syndrome and chronic hepatitis C (5.3% each) (Table 1).
Most of the patients received Rixubis for prophylaxis (78.9%), followed by bleeding (63.2%), and surgery and/or perioperative coverage (3.5%). The mean (SD) doses of Rixubis for prophylaxis, bleeds, and surgery and/or perioperative coverage was 41.9±11.1 IU/kg, 43.8±14.4 IU/kg, and 45.0±1.8 IU/kg per infusion, respectively (Table 2).
Safety
In the SAS, 11 AEs were reported in eight patients (14.0%), of which three were SAEs and observed in three patients (5.3%). The SAEs included hemophilic arthropathy in two patients (3.5%) and one inhibitory antibody development in one patient (1.8%), for which the confirmatory test was negative. All 11 AEs that occurred were reported as unexpected and mild in severity; only one AE (unconfirmed anti-FIX antibody increase) was related to the study drug while the remaining 10 AEs were unrelated to the study drug. Based on outcomes, the 10 AEs (90.9%) were considered resolved and one (upper abdominal pain) was in the recovery stage. Anaphylaxis was not reported in any of the patients during the study period (Table 3).
Effectiveness
In the EAS, 66 assessments for the treatment of bleeding were conducted in 25 patients, and hemostatic effectiveness was evaluated as “excellent,” “good,” and “fair” in 5 (7.6%), 50 (75.8%), and 11 cases (16.7%), respectively. Overall, 55 assessments were reported as effective (excellent and good) in 18 patients (72.0%), and the clinical effectiveness rate was 83.3%. For prophylaxis, 76 assessments were conducted in 40 patients; of these, 68 (89.5%) assessments were reported as effective. The effectiveness was reported as “excellent,” “good,” and “fair” in 21 (27.6%), 47 (61.8%), and 8 cases (10.5%), respectively. A total of 142 assessments were conducted for both treatment types in 54 patients; of these, 123 were reported as effective in 42 patients (77.8%), and the overall clinical effectiveness rate was 86.6% (Table 4).
DISCUSSION
The present PMS study evaluated the safety and hemostatic effectiveness of Rixubis used prophylactically or on-demand and for surgery and/or perioperative coverage in pediatric and adult patients with hemophilia B in real-world settings in South Korea. Given the increased number of hemophilia B patients in South Korea in recent years [3, 4] and the paucity of prospectively collected data on real-world use, the clinical experiences of those receiving Rixubis for bleeding control, surgery and/or perioperative coverage, and prophylaxis in the current study are important.
Previous studies have demonstrated the safety and efficacy of Rixubis for routine prophylaxis as well as for bleeds and surgery and/or perioperative management [12, 14]. The first-in-human trial and subsequent studies of BAX326 showed improved outcomes with a reduction in the number of bleeds, a better safety profile, and improved health-related quality of life after prophylactic treatment in patients with hemophilia B [12-15]. Primary prophylaxis is considered the standard treatment for children with severe hemophilia in South Korea [16, 17]. In the current study, most patients received Rixubis for prophylaxis (78.9%) compared to that for bleeds (63.2%) or surgery (3.5%), indicating the safety awareness and importance of prophylactic treatment with recombinant products in South Korean patients with hemophilia B.
The safety profile of any rFIX product is characterized by a low incidence of AEs [18-20]. In the present study, the overall incidence of AEs was 14% (11 AEs reported in eight patients). All the AEs reported in this study were unexpected and mild in severity. Furthermore, most of the AEs (10) were unrelated to the study drug. Three SAEs were reported in three patients (5.3%) and included hemophilic arthropathy in two patients (3.5%) and one unconfirmed event of inhibitory antibody development in one patient (1.8%), which was found to be negative in subsequent testing. Of note, all AEs that occurred were temporarily associated and resolved by the time the study was completed. None of the patients developed anaphylaxis, and no death was reported during the study. Our observations on the safety of Rixubis are consistent with those of a prospective study that reported a 17% incidence of AEs (22 AEs in 11 patients) in previously untreated patients receiving BeneFix [19].
The development of inhibitory antibodies against FIX is the most critical complication in patients with hemophilia B [21], with an incidence of 1–4% [22, 23]. In the current study, there was an unconfirmed report of increased anti-FIX antibody levels in one patient (1.8%), for which the dose was not changed, and the outcome was recovery/resolution at the end of the study. Additionally, in this study, there were three patients with a family history of inhibitor development, which is one of the high-risk factors for inhibitory antibody development; inhibitor development did not occur in these patients [24]. Similar to our findings, previously published studies reported no incidence of inhibitory or Rixubis-related specific antibody development [12, 14, 15]. However, other studies reported a higher incidence of inhibitor development in patients with hemophilia B. In a 20-year Swedish population-based study, 37% (6/16) of patients with hemophilia B developed inhibitors after treatment with a high-purity pdFIX product [25].
Early prophylactic treatment aimed at maintaining a trough level higher than 1% has been associated with a decrease in the number of bleeds [6]. In this study, the overall hemostatic efficacy of Rixubis was rated as “effective” in 86.6% (123) of the assessments by both physicians and patients. When individual treatment type was considered, the effectiveness rates were 83.3% (55) and 89.5% (68) for on-demand treatment of bleeding and prophylaxis, respectively. The study results are consistent with those of previously published studies that have reported the hemostatic efficacy of rFIX products as good/excellent for ≥90% of bleeding episodes [9, 12, 15]. Further, the ratings for hemostatic effectiveness by physicians were higher than those of patients’ for both treatment of bleeding and prophylaxis. This finding is similar to that of a PMS study wherein the physicians’ evaluation of drug effectiveness was favorable for both on-demand treatment and prophylaxis [26].
The development of Rixubis is an important step toward increasing the worldwide availability of rFIX products for the treatment of hemophilia B. As a recombinant protein product devoid of viruses and other pathogens, Rixubis minimizes the risk of transmission of blood-borne pathogens and thereby can be an important treatment option over pdFIX products. Furthermore, Rixubis, which is an rFIX product with a standard half-life, has the ability to control FIX activity and may help in reducing thrombotic risk during acute bleeding episodes and surgery [27].
Limitations
This prospective real-world study is limited by its study design, wherein causal inferences cannot be made due to the lack of a control or comparator group. Furthermore, the data on annualized joint bleed and bleeding rates (based on both treatment types, i.e., on-demand vs. prophylaxis) were not estimated, and hence, the effectiveness of Rixubis in terms of lowering the frequency of joint bleeds and all bleeds could not be inferred. Rixubis was recently approved in the global market, and a complete elucidation of its safety profile for routine use will require long-term PMS studies in various geographies and different cohorts.
CONCLUSION
The study results demonstrated that Rixubis administered for on-demand treatment of bleeding, surgery and/or perioperative coverage, and prophylaxis was effective without increasing the risk of AEs in pediatric and adult patients with hemophilia B in real-world settings in South Korea. The overall safety and effectiveness rate were comparable with those of other currently available rFIX products, supporting the use of Rixubis in the prevention and treatment of bleeding in hemophilia B.
 XML Download
XML Download