

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Remdesivir is a nucleotide prodrug that demonstrates in vitro antiviral activity against beta coronaviruses including severe acute respiratory syndrome coronavirus (SARS-CoV), Middle East respiratory syndrome coronavirus, and SARS-CoV-2, by inhibiting viral RNA polymerases.12 The first randomized controlled trial (RCT) of remdesivir therapy for coronavirus disease 2019 (COVID-19) was conducted in China and showed numerical tendencies favoring remdesivir treatment.3 The following phase III RCT, the Adaptive COVID-19 Treatment Trial-1 (ACTT-1), demonstrated a significant reduction for median recovery time in the remdesivir arm, especially among patients receiving O2 support.4 Based on the findings of the ACTT-1 trial, remdesivir has been widely used for the treatment of COVID-19 but controversies regarding its clinical effectiveness remain.56789 Previous studies have focused on clinical outcomes of remdesivir treatment, with heterogeneous results depending on study design, administration timing, and severity of host.34567 For more rational use of remdesivir for COVID-19, further detailed investigations regarding clinical and virologic response are required.
In the Republic of Korea, all costs of COVID-19 patient care are covered by the government. A nation-wide electronic case report form (eCRF) coding system for laboratory-confirmed COVID-19 patients has been implemented since February 2020.10 Remdesivir has been supplied from July 1, 2020 with strict clinical criteria, and detailed information regarding clinical course and the results of serial real-time reverse-transcriptase polymerase chain reaction (RT-PCR) tests have been recorded. Herein, we report our findings regarding clinical and virologic response to remdesivir among severe COVID-19 patients in the Republic of Korea.
METHODS
Study design
A nation-wide multi-center retrospective cohort study were designed to evaluate the effectiveness of remdesivir on the clinical and virologic outcomes of severe COVID-19 patients. Remdesivir became available for use on July 1, 2020 in the Republic of Korea, and therefore we included patients who were hospitalized with severe COVID-19 between June 1 and July 31. This period begins one month before remdesivir was introduced and ends one month after remdesivir became available. We compared clinical and virologic data between individuals who received (remdesivir group) or did not receive (supportive care group) remdesivir treatment during the study period.
Study patients
Laboratory-confirmed adult (age ≥ 18) COVID-19 patients who met clinical criteria for remdesivir supplement determined by the Korean government during hospitalization were screened.11 The clinical criteria included: 1) radiologically-identified pneumonia (either by chest X-ray or computed tomography), 2) hypoxia (SpO2 ≤ 94%), 3) O2 supply requirement (either by nasal cannula, facial mask, or high flow nasal cannula), and 4) early phase COVID-19 (≤ 10 days from symptom onset). The definition of severe COVID-19 in the present study followed the clinical criteria for the remdesivir supplement. Patients who meet the criteria 1) to 3) are defined as severe COVID-19 patients. Patients who met the clinical criteria for remdesivir treatment at the time of admission but received mechanical ventilator (MV) support on the day of admission, patients with incomplete outcome data, and patients in do not resuscitate status were excluded from the cohort. Included patients were classified into either the remdesivir group (admitted in late June or July and received remdesivir) or the supportive care group (admitted in June and could not receive remdesivir).
Outcome variables
Clinical status was assessed on hospital days (HDs) 14 and 28 to evaluate the clinical effectiveness of remdesivir treatment. The primary clinical endpoint was clinical recovery on HD 14 and 28, defined as a decrease of up to 1 or 2 points by the previously described 8-point ordinal scale or live discharge.10 Co-primary endpoints were requirement of additional MV support by HD 14 and 28, and duration of O2 and MV support before HD 28. Secondary endpoints were National Early Warning Score (NEWS) on HD 14 and 28, mortality associated with COVID-19 by HD 14 and 28, duration of hospital stay, and all-cause mortality during hospitalization.
For the analysis of virologic response, upper respiratory tract (URT) specimens including nasopharyngeal and oropharyngeal swabs and lower respiratory tract (LRT) specimens including sputum and endotracheal aspirate were evaluated. RT-PCR tests for SARS-CoV-2 were conducted at each hospital or commissioned laboratories, using test kits approved by the Korean Ministry of Food and Drug Safety for emergency use authorization. These kits include the Allplex™ 2019-nCoV Assay kit (Seegene, Seoul, Korea), PowerCheck™ 2019-nCoV RT-PCR kit (KogeneBiotech, Seoul, Korea), and Real-Q Direct SARS-CoV-2 Detection kit (BioSewoom, Seoul, Korea).12 Virologic responses were evaluated by HD 15, and changes of cycle threshold (Ct) values of the RNA-dependent RNA polymerase gene were used for the assessment of viral load reduction. Since several RT-PCR kits from different manufacturers were used, we calculated changes of Ct value individually, and compared calculated values between the groups. To calculate of viral load reductions in individual patients, three analyses were conducted, including comparison of slopes of Ct value increase calculated from all available individual RT-PCR test results (virologic analysis 1), comparison of slopes of Ct value increase calculated from three fixed time points, including HD 1–5, 6–10, and 11–15 (virologic analysis 2), and comparison of differences of Ct values between HD 1–5 and 11–15 (virologic analysis 3). For the calculation of Ct value slopes, at least two-point values are required and patients with more than single point RT-PCR test result were included in the virologic analysis 1. In the comparison of three fixed time points (virologic analysis 2 and 3), patients with RT-PCR test result at all of each time point were included in the analysis.
Statistical analysis
Baseline characteristics were summarized using descriptive statistics including proportion, mean and standard deviation. Slopes of Ct values were calculated by linear regression. Student's t-test and the Mann-Whitney test were used to compare continuous variables, and the χ2 test or Fisher's exact test were used to compare categorical variables. All P values were two-tailed, and values < 0.05 were considered to be statistically significant. All statistical analyses were performed using SPSS 26.0 for Windows (SPSS, Chicago, IL, USA), while GraphPad Prism 5.01 (GraphPad Software, San Diego, CA, USA) was used for figure development.
RESULTS
Baseline characteristics of severe COVID-19 patients
During the study period between June 1, 2020, and July 31, 2020, 101 patients were screened according to our inclusion criteria from the registries of 20 hospitals (Fig. 1). After excluding 15 patients due to insufficient data or requirement of MV support on day of admission, a total of 86 severe COVID-19 patients were included in the analysis and classified into remdesivir (n = 48) and supportive care (n = 38) groups. Baseline characteristics of cohort patients are presented in Table 1, and were not significantly different between groups. The mean patient age was 68.56 years and 39.5% were male. Patients were admitted to the hospital on average 3 days from symptom onset. Remdesivir was administered on average 7.42 and 4.42 days from symptom onset and from admission, respectively. Hypertension was the most frequently reported underlying disease (48.8%), followed by diabetes (24.4%), chronic heart disease (5.8%), chronic lung disease (4.7%), and chronic renal disease (4.7%). Mean body mass index was 24.6, NEWS at admission was 3.02 and initial Ct value was 24.42 in average. About a half of all patients (52.3%) were at ordinal scale 1 (no limit of activity) and 31.4% were at ordinal scale 3 (O2 with nasal prong) on admission. Laboratory findings including complete blood count, liver function tests, and renal function tests were within normal ranges, while lactate dehydrogenase (mean, 437.79 ± 193.26 IU/L) and C-reactive protein (8.16 ± 24.43 mg/dL) were elevated.
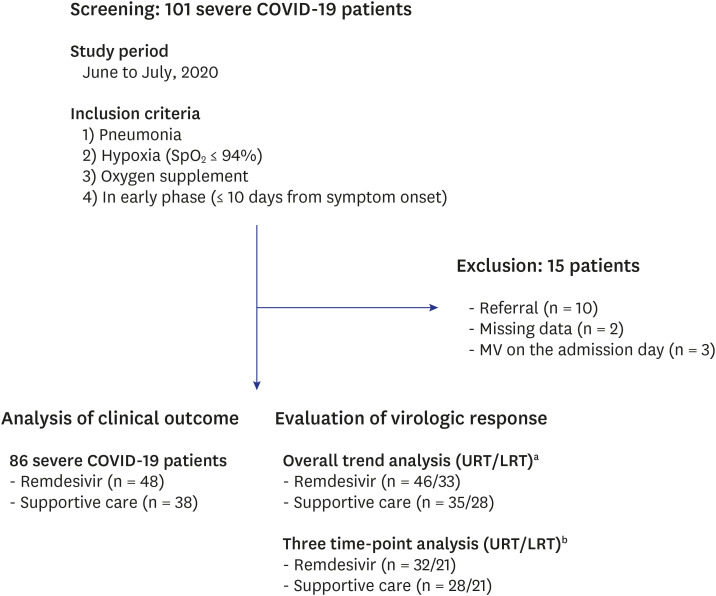
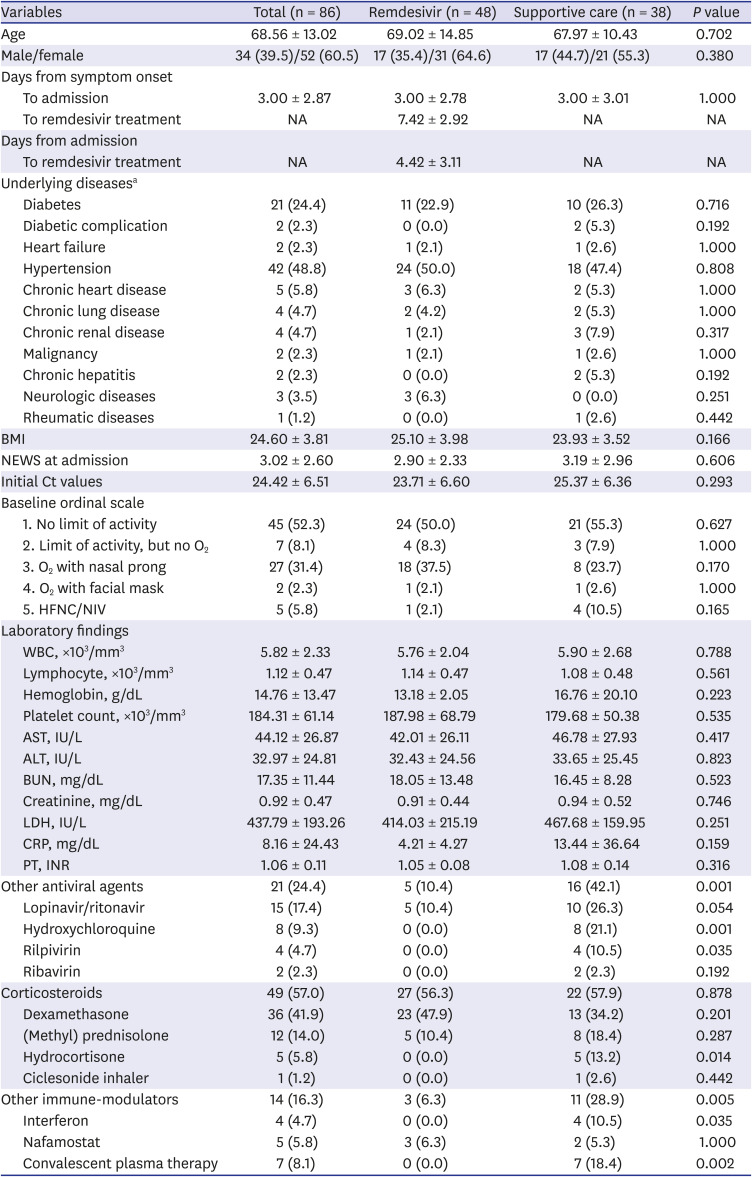
Fig. 1
Population of the cohort study.
COVID-19 = coronavirus disease 2019, MV = mechanical ventilation, URT = upper respiratory tract, LRT = lower respiratory tract, HD = hospital day, RT-PCR = real-time reverse-transcriptase polymerase chain reaction.
aFor the calculation of cycle threshold value slopes, at least two-point values are required and patients with more than single point RT-PCR test result were included in the overall trend analysis; bPatients with RT-PCR test result at all of each fixed time point (HD, 1–5, 6–10, and 11–15) were included in the three time-point analysis.
![]()
Table 1
Baseline characteristics of severe coronavirus disease 2019 patients on admission day
Data are expressed as the number (%) of patients or mean ± standard deviation.
NA = not applicable, BMI = body mass index, NEWS = National Early Warning Score, Ct = cycle threshold, HFNC = high flow nasal cannula, NIV = non-invasive ventilation, WBC = white blood cell, AST = aspartate transaminase, ALT = alanine transaminase, BUN = blood urea nitrogen, LDH = lactate dehydrogenase, CRP = C-reactive protein, PT = prothrombin time, INR = international normalized ratio.
aNo patients had dementia, hematologic disorders, or human immunodeficiency virus infection.
![]()
Overall, 24.4% of patients received antiviral agents other than remdesivir, including lopinavir/ritonavir (17.4%), hydroxychloroquine (9.3%), rilpivirin (4.7%), or ribavirin (2.3%). More patients in the supportive care group received hydroxychloroquine or rilpivirin, compared to the remdesivir group (P = 0.001 and P = 0.035, respectively). About half of all patients (57.0%) received corticosteroid therapy, and the proportion of patients receiving corticosteroid therapy was similar between the two groups. Some patients in the supportive care group received interferon (10.5%) or convalescent plasma therapy (18.4%), while none of the remdesivir group did (P = 0.035 and P = 0.002, respectively).
Clinical outcomes of the remdesivir group compared to the supportive care group
Clinical outcomes of the cohort patients are presented in Table 2. Among the primary endpoints, the proportion of patients requiring MV support before HD 28 was significantly lower in the remdesivir group (22.9%) compared to the supportive care group (44.7%, P = 0.032). Duration of MV support was also significantly shorter in the remdesivir group (mean, 1.97 ± 4.44 days) compared to the supportive care group (mean, 5.37 ± 7.63; P = 0.017). Other primary endpoints including proportion of patients exhibiting clinical recovery at HD 14 and 28, time to recovery, MV support before HD 14, and duration of O2 support were not significantly different between the treatment groups.
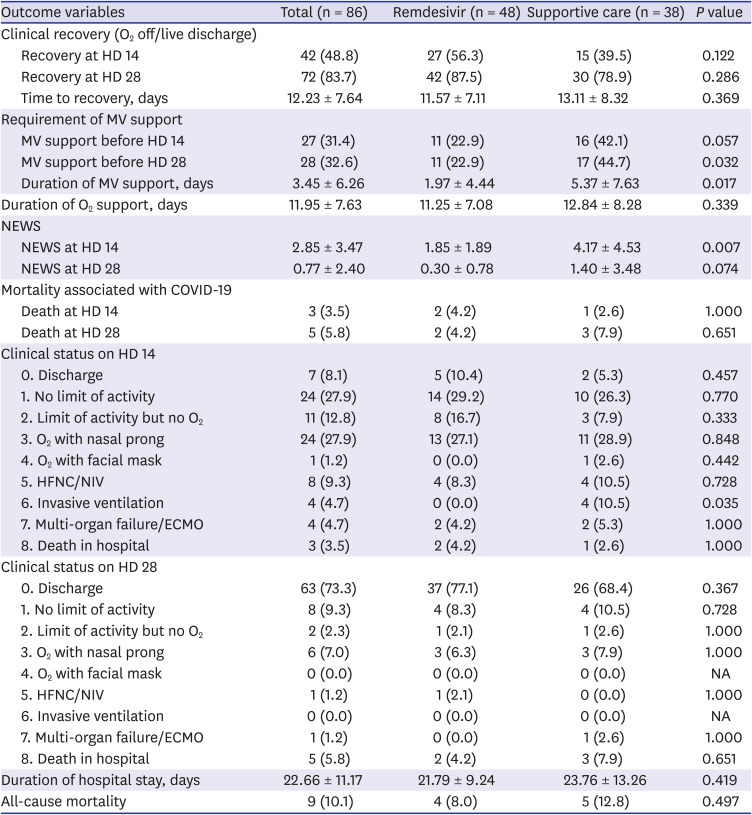
Table 2
Clinical outcomes of the remdesivir group and the supportive care group
Data are expressed as the number (%) of patients or mean ± standard deviation.
HD = hospital day, MV = mechanical ventilation, NEWS = National Early Warning Score, COVID-19 = coronavirus disease 2019, HFNC = high flow nasal cannula, NIV = non-invasive ventilation, ECMO = extracorporeal membrane oxygenation, NA = not applicable.
![]()
Among the secondary endpoints, NEWS at HD 14 was significantly lower in the remdesivir group (mean, 1.85 ± 1.89) compared to the supportive care group (mean, 4.17 ± 4.53; P = 0.007). In addition, the proportion of patients requiring MV support at HD 14 was significantly lower in the remdesivir group (0.0%) compared to the supportive care group (10.5%, P = 0.035). Other secondary endpoints including mortality associated COVID-19, clinical status on HD 28, duration of hospital stay, and all-cause mortality were not different between the two groups.
A subgroup analysis was conducted among 29 patients who received O2 therapy (at clinical status ordinal scale 3 or 4) on admission day (Supplementary Table 1). Similar to the main cohort, the proportion of patients requiring MV support by HD 14 and 28 was significantly lower in the remdesivir group (both 21.1%), compared to the supportive care group (both 70.0%, P = 0.017). Other outcome variables were not different between the two groups.
Virologic response according to treatment group
For comparisons of overall virologic response, we calculated slopes of Ct values of individual patient was calculated using all available RT-PCR test results before HD 15 and compared slope values between the two groups (virologic analysis 1, Fig. 2). In analysis of URT specimens, the remdesivir group showed a significantly steeper increase in Ct value (n = 46; median, 1.33; interquartile range [IQR], 0.62, 1.33) compared to the supportive care group (n = 35; median, 0.80; IQR, 0.19, 1.13; P = 0.043). The remdesivir group also showed a steeper increase in Ct values when we examined LRT specimens (n = 33; median, 0.99; IQR, 0.26, 1.15) compared to the supportive group (n = 28; median, 0.75; IQR, −0.05, 0.99) but the difference was not significant (P = 0.291).
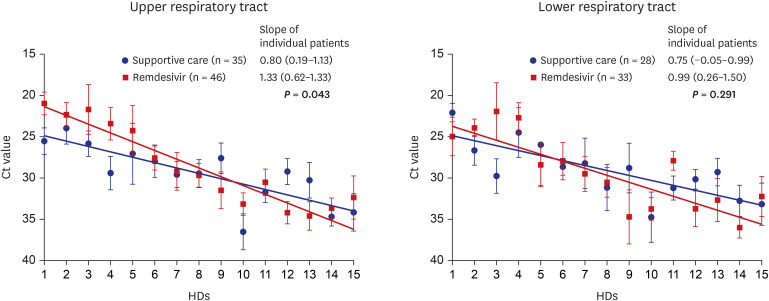
Fig. 2
Comparisons of overall virologic response between treatment groups. Slopes of Ct values were calculated for individual patients using all available RT-PCR test results by HD 15 and compared between treatment groups (virologic analysis 1). Since at least two-point values are required for the calculation of slopes (using linear regression), patients with more than single point RT-PCR test result were included in this analysis.
Ct = cycle threshold, RT-PCR = real-time reverse-transcriptase polymerase chain reaction, HD = hospital day.
![]()
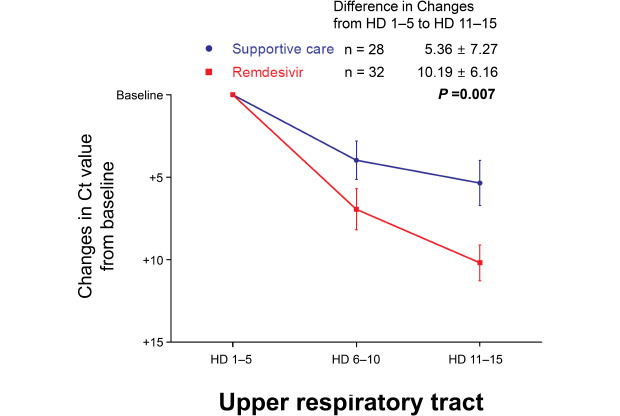
To evaluate viral load reduction along a controlled timeline, the first RT-PCR test results for each fixed time point (HD, 1–5, 6–10, and 11–15) were selected and compared between the two groups (Fig. 3). Using URT specimens, the slope of Ct value increase was significantly steeper in the remdesivir group (mean, 5.10 ± 3.08) compared to the supportive care group (mean, 2.68 ± 3.63; P = 0.007; virologic analysis 2). The increases of Ct value from HD 1–5 to 11–15 were also significantly greater in the remdesivir group (n = 32; mean, 10.19 ± 6.16) compared to the supportive care group (n = 28; mean, 5.36 ± 7.27; P = 0.007; virologic analysis 3). Using LRT specimens, the slope of Ct value increase was steeper in the remdesivir group (n = 21; mean, 4.54 ± 3.93) compared to the supportive care group (n = 21; mean, 2.97 ± 3.36), without statistical significance (P = 0.170). The remdesivir group showed greater Ct value increase from HD 1–5 to 11–15 (mean, 9.02 ± 7.84) compared to the supportive care group (mean, 5.94 ± 6.72), but the difference was not significant (P = 0.179).
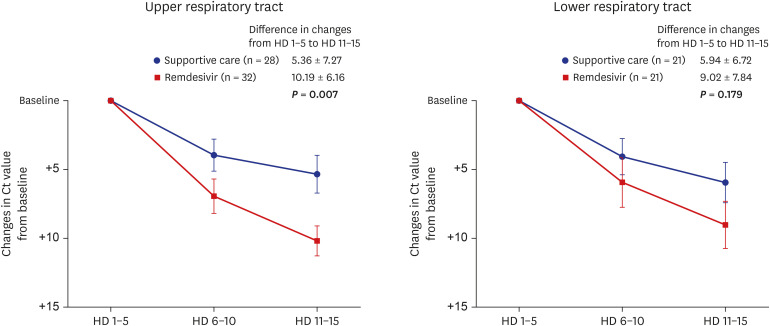
Fig. 3
Comparisons of virologic response at three fixed time points. To evaluate viral load reduction along a controlled timeline, the first RT-PCR test results during each fixed time point (HD, 1–5, 6–10, and 11–15) were selected and compared between the two groups. Patients with RT-PCR test result at all of each fixed time point (HD, 1–5, 6–10, and 11–15) were included in the three time-point analysis. The slopes of Ct value increase (virologic analysis 2) and differences of Ct values from HD 1–5 to 11–15 (virologic analysis 3) were compared between the two groups.
Ct = cycle threshold, RT-PCR = real-time reverse-transcriptase polymerase chain reaction, HD = hospital day.
![]()
DISCUSSION
The importance of early administration of antiviral agent in the treatment of respiratory virus infections has been emphasized.131415 In the first remdesivir RCT for COVID-19, drug administration was performed a median of 11 days from symptom onset, and patients who received remdesivir early (≤ 10 days of symptom onset) showed numerically better outcomes than those who received remdesivir late.3 Randomization was performed earlier in the ACTT-1 trial (median nine days from symptom onset), which also supported the clinical benefit of remdesivir.4 In subsequent studies supporting the beneficial effect of remdesivir, the drug was administered early, ranging from a median six to eight days from symptom onset.56 However, the Solidarity Trial, designed early in the COVID-19 pandemic by the World Health Organization, reported negative results of remdesivir treatment (rate ratio, 0.95; 95% confidence interval [CI], 0.81–1.11; P = 0.50).7 Although randomization time from symptom onset was not considered in this trial due to practical issues, the outcomes of this large trial (including about 2,700 patients per arm) cannot be disregarded. Since conducting another well-designed large-scale trial would not be feasible, detailed evaluations of the effectiveness of remdesivir would help clinicians engage in rational use of the drug.
During the study period, the number of daily new COVID-19 patients in the Republic of Korea remained within the tolerable capacity of the Korean healthcare system. Remdesivir was administered with strict clinical criteria, serial RT-PCR tests for most severe COVID-19 patients could be performed, and medical records were collected anonymously by the governmental eCRF system. Remdesivir was administered early in our cohort, within 7.42 days from symptom onset and 4.42 days from admission on average. Other baseline characteristics were not different between the two groups. Although antiviral agents other than remdesivir were administered more often in the supportive care group, corticosteroids, which have proven efficacy in the COVID-19 treatment, were similarly administered between the two groups. We demonstrated clear clinical benefits of remdesivir treatment in the present study. Significantly fewer patients required MV support before HD 28 (P = 0.032) and the duration of MV support was shorter (P = 0.017) in the remdesivir group compared to the supportive care group. NEWS at HD 14 was significantly lower in the remdesivir group (P = 0.007). Subgroup analysis was performed among patients who received O2 therapy on admission, because such patients derived the most clinical benefit from remdesivir in the ACTT-1 trial.4 Significantly lower requirement for and shorter duration of MV in the remdesivir group were also detected. These findings support the clinical effectiveness of remdesivir treatment for severe COVID-19 patients, especially by preventing the requirement of MV. Although other clinical outcomes including proportion of clinical recovery, duration of hospital stay, and all-cause mortality were not statistically different between the two groups, the numerical difference of these outcomes showed a tendency favoring the remdesivir group. Considering that the ACTT-1 trial exhibited survival benefit in a subgroup of patients who required O2 supplement (n = 435; hazard ratio, 0.30; 95% CI, 0.14–0.64), a large scale meta-analysis study evaluating severe COVID-19 patients who received remdesivir at an early stage of infection need to be conducted.4
In addition, rapid viral load reduction was observed after remdesivir treatment in the present cohort. Since RT-PCR tests are conducted at irregular intervals in real-world practice, it would be difficult to assess the exact time required for viral clearance. In addition, the initial viral loads of patients in each group may have been different without randomization into treatment groups comprising sufficient patient numbers. To overcome such limitations, we estimated the reduction of viral load using a similar method to that used in RCT studies for monoclonal antibodies.1617 In analyses of URT specimens, increases of Ct value were significantly steeper in the remdesivir group, both in the overall analysis and three-point evaluation. Although significant differences were not observed in analyses of LRT specimens, the increase in Ct values was numerically steeper in the remdesivir group. The reason why the difference of Ct value changes in LRT specimens were not statistically significant would be probably due to limited number of evaluated LRT specimens. In vitro and animal studies previously demonstrated the anti-SARS-CoV-2 effect of remdesivir,218 but its effect on viral load has not been clearly elucidated in clinical studies. To our knowledge, this is the first clinical study to examine virologic response to remdesivir treatment together with clinical benefits, which may enhance the rationale underlying remdesivir treatment for the management of severe COVID-19.
Our study has several limitations. First, since this retrospective cohort study was conducted during a short period when the COVID-19 outbreak in the Republic of Korea was relatively well-controlled, the number of patients evaluated in the cohort was limited. However, as healthcare capacity remained tolerable during the study period, patient care was more homogenous and RT-PCR tests could be conducted more frequently than during later outbreak-surging periods. Remdesivir was provided according to strict clinical criteria, and medical records were carefully kept. Second, several RT-PCR kits from different manufacturers were used and Ct values were not converted to viral copies and heterogeneous test kits were used. To overcome this limitation, Ct values were not directly compared between groups. Changes of Ct value were calculated individually, and then the changes were compared between two groups. Although it would not completely reflect changes of viral loads, this approach would compensate potential biases that may occur from using different RT-PCR kits to some degree. Third, RT-PCR tests were not conducted at regular intervals, and some patients were not included in analyses of virologic response due to insufficient RT-PCR test data. Fourth, as a retrospective cohort study, various clinical factors that might affect clinical and virologic outcome would be different between the two groups. Significantly more patients in the supportive care group received antiviral agents other than remdesivir, based on in vitro research data.1920 Nevertheless, baseline characteristics were not statistically different between the two groups. Most antiviral agents other than remdesivir, especially lopinavir/ritonavir and hydroxychloroquine, were proved to be ineffective for COVID-19.212223 Although the effect of interferon and convalescent plasma therapy is still controversial,24252627282930 potential antiviral effect of these agents may not result in over-estimation of the positive effect of remdesivir, since these agents were administered only in the supportive care group. Despite these limitations, this study presents an additional rationale for the application of remdesivir treatment in severe COVID-19 patients, which may help clinicians in the field during the ongoing COVID-19 pandemic.
In conclusion, the remdesivir group exhibited clinical and virologic benefit in terms of lower MV requirement and more rapid viral load reduction compared to the supportive care group, though the proportion of clinical recovery and all-cause mortality were not statistically different between the groups. Our findings support the use of early remdesivir treatment for severe COVID-19 patients.
 XML Download
XML Download