

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Extreme premature infants are born with immature lungs and despite the advances in neonatology, the incidence of bronchopulmonary dysplasia (BPD) is increasing. Severe BPD is associated with an increased risk of cardiovascular impairment, long-term pulmonary sequelae, and neurodevelopmental impairment.1 In addition, BPD is associated with increase in re-hospitalization after discharge and neurodevelopmental impairment, which decrease the quality of life in children.2 In the first year of life, 118 of 238 (49%) infants with BPD were re-hospitalized, more than twice the rate of re-hospitalization of the non-BPD population, which was 309 of 1,359 (23%).3
Many investigations for the prevention of BPD have been conducted. As a result, noninvasive instillation of artificial surfactant, minimizing pressure or volume during ventilator care, postnatal steroid treatment, nutritional support, etc. were suggested.4
Therefore, it is important to prevent the development of BPD in the first place. So far, a BPD prediction program has been published based on data of birth weight, gestational age (GA), sex, patent ductus arteriosus, sepsis and artificial ventilators, but the program is not widely adopted. In addition, even after the concept of new BPD was introduced in neonatology, the definition and classification of BPD was changed.5
In 2011, National Institute of Children Health and Human Development and Neonatal Research Network (NICHD-NRN) published a validated strategy for prediction of BPD, categorized as none, mild, moderate, or severe using the physiologic definition; prediction was based on demographic variables and respiratory support at days 1, 3, 7, 14, 21, and 28.6
Recently the online BPD outcome estimator form NICHD-NRN was launched.6 However, it is not applicable for Asians. Birth weight and gestational weeks are limited to less than 1,250 grams birth weight in 23 to 30 weeks gestation. In the 2016 annual report of Korean Neonatal Network (KNN),7 there were about 28.6% BPD in very low birth weight infants (VLBWIs) whose birth weight was more than 1,250 grams. Also, there were 30.4% BPD in KNN VLBWI whose GA was more than 31weeks.8 Thus, a BPD prediction program for Korean very low birth weight infants is necessary.
If BPD occurrence is predicted in certain patients, it is helpful not only for parents' consultations but also for participant selection of new clinical trials. This leads to the idea of using early steroid treatments, and neonatal therapeutic factors related to BPD occurrence, such as infection prevention and artificial ventilator management.
Therefore, we conducted a study for early clinical indicators that make it possible to predict occurrence and severity of BPD at the corrected age of 36 weeks. It can improve outcomes as a way of prognosis evaluation through prediction of BPD, the most common and important chronic pulmonary disorder. The aim of this study was to make a prediction model for BPD through clinical indicators within the first hour of delivery.
Go to : 
METHODS
Subjects
The KNN is a nationwide database on VLBWI across South Korea. Data were collected for 8,022 VLBWIs with GA ≥ 22 weeks who were born between January 1, 2013 and December 31, 2016, and admitted to the neonatal intensive care units of the KNN9 by local staff using a standardized electronic case report form.
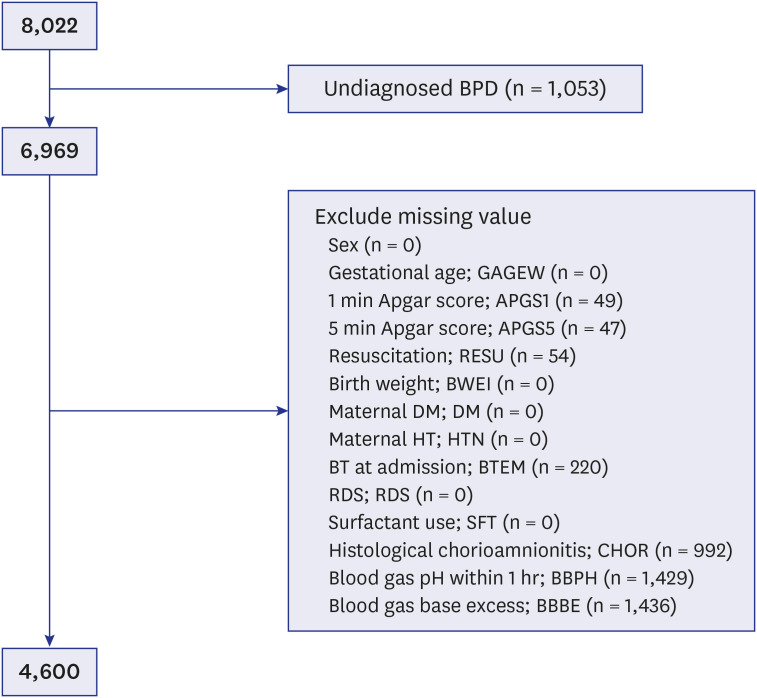
The inclusion criteria for this analysis from KNN data was all VLBWIs born in or transferred to participating neonatal centers within 28 days of birth and surviving to discharge home. In this study, 1053 undefined BPD VLBWIs died before 28 days. After all VLBWIs with missing data were excluded, 4,600 VLBWIs were included in the training dataset (Fig. 1).
The Samsung Medical Center Institutional Review Board (2013-03-002) approved this study. From 2013 to 2016, a total of 49, 55, 60, and 66 neonatal intensive care units (NICUs) participated annually and registered 1,396, 2,123, 2,392, and 2,358 VLBWIs, in the registry of the KNN, respectively. The population in this study included about two-thirds of the annual VLBWIs born in Korea except 2013. This study is based on data from annual reports of the KNN from 2013 to 2016.10111213
Each institutional review board of all hospitals participating in the KNN approved the data registry. Written consent was obtained from the parents of infants during enrollment in KNN.
Maternal and neonatal variables
Representative clinical parameters were selected based on a previous 10-year study using data mining from a single institution investigating 100 variables associated with BPD. The maternal variables included gestational diabetes, pregnancy-induced hypertension, and maternal chronic hypertension. The neonatal variables included sex, GA, birth weight, Apgar score at 1- and 5-min, immediate resuscitation at delivery including intubation, chest compressions and use of surfactant at the DR, immediate result of postnatal blood gas analysis (measured within one hour after birth), respiratory distress syndrome (RDS) and BPD.
The definitions of collected data was guided by the manual of operations of the KNN (http://www.knn.or.kr/index.jsp). Maternal diabetes was diagnosed based on gestational diabetes or overt diabetes during pregnancy. Maternal hypertension diagnosis was based on any maternal diagnosis of pregnancy-induced hypertension or chronic hypertension in pregnancy. Chorioamnionitis was defined as the presence of acute inflammatory change in the amnion, chorion-decidua, umbilical cord, or chorionic plate based on histologic examination by a pathologist. Extensive resuscitation was defined as administration of chest compression, with or without administration of epinephrine, at birth in the delivery room.
GA was determined by obstetric examination with ultrasonography early during the pregnancy or via obstetric history based on the mother's last menstrual period. Birth weight was recorded for each baby as soon as the baby arrived at the NICU for admission. Infants with blood pH and base deficit (BD) values collected within the first hour after birth. BPD was defined by NIH classification.14 BPD was represented as none (0), mild (1) moderate (2) severe (3).
Statistical analyses
SAS 9.4 (SAS Institute Inc, Cary, NC, USA) and R 3.5.0 (R Foundation for Statistical Computing, Vienna, Austria) were used for all statistical analyses. Chi-square test and one-way ANOVA model was used to compare baseline characteristics between BPD stages. Multiple logistic regression models were used to calculate odds ratio (OR), 95% confidence intervals (95% CIs), and corresponding p values. Stepwise variable selection method in logistic regression model was used to evaluate prediction model. Propensity scores were calculated with prediction model. Moreover, it was used to search best cut-off value. PROC package (X. Robin et al. 2011) was used to calculate area under curve (AUC) and corresponding 95% CI. Significance level was set less than 0.05. External validation was performed with 2017 KNN data, which was the same treatment policy in the same Korean population.15
Ethics statement
The KNN registry was approved by the institutional review board at each participating hospital and informed consent was obtained from parents at enrollment in NICUs participating in the KNN (EUMC 2013-09-003-015).
Go to :
RESULTS
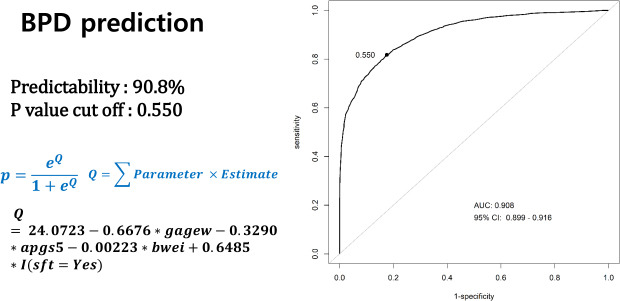
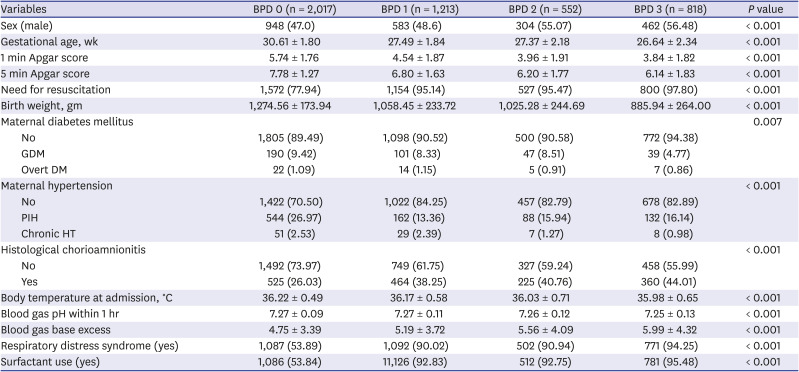
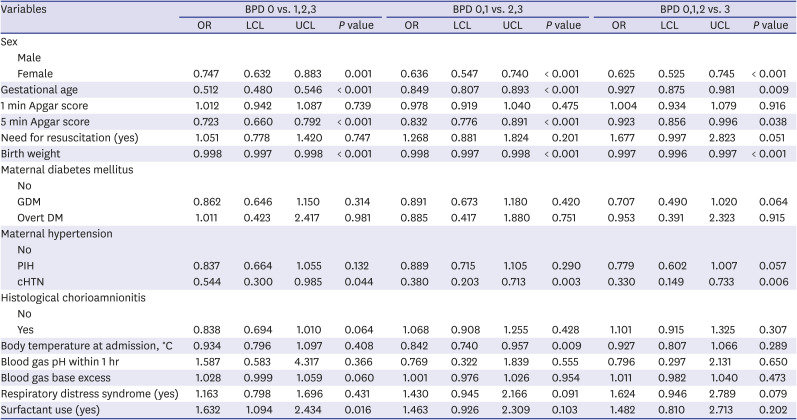
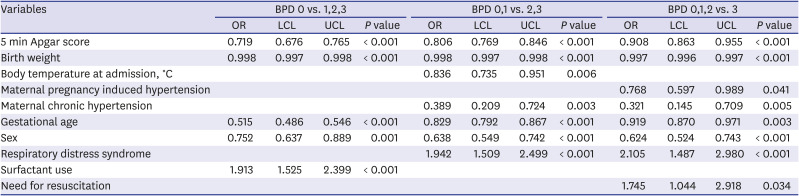
A total of 4,600 VLBWI were enrolled in the training dataset (Table 1). The range of GA was from 22.1 weeks to 34.6 weeks. The range of birth weight was from 280 grams to 1,499 grams. About 56.2% of Korean VLBWIs have BPD. All variables, except maternal DM, was correlated with a greater severity of BPD. Based on analysis of training dataset for each BPD grading group, sex, GA, birth weight, 5-minute Apgar score, and chronic maternal hypertension, were significantly associated with the severity of BPD. Body temperature at admission was significantly associated between more than moderate BPD and others. Use of artificial surfactant was significantly associated with the presence of BPD (Table 2). In multiple logistic regression model, stepwise selection method was used to select significant clinical indicator for BPD. For the analysis of diagnosis of BPD, 5-minute Apgar score, birth weight, GA, sex, and surfactant use were significant indicators. For the analysis of presence of more than moderate BPD, 5-minute Apgar score, birth weight, body temperature at admission, chronic maternal hypertension, GA, sex, and RDS were significant indicators. For the analysis of severe BPD, 5-minute Apgar score, birth weight, maternal PIH, chronic maternal hypertension, GA, sex, RDS, and need of resuscitation at birth were significant indicators (Table 3). In Figs. 2, 3 and 4, functions for prediction of present BPD (p) were suggested. These functions were calculated by logistic regression model with selection method. To calculate AUC, propensity score by p function and real BPD present were used. Sensitivities and specificities were calculated as increase cut-off value by 0.1 between 0 to 1, to propensity score.
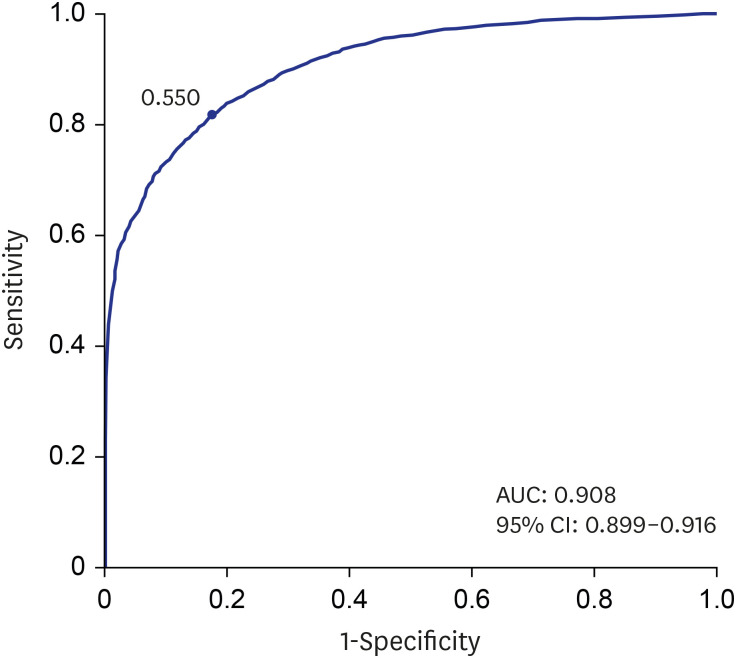 | Fig. 2 Receiver operating characteristic curve and accuracy of BPD prediction in Korean Very Low Birth Weight Infants. BPD prediction equation is p = eQ1+eQ
|

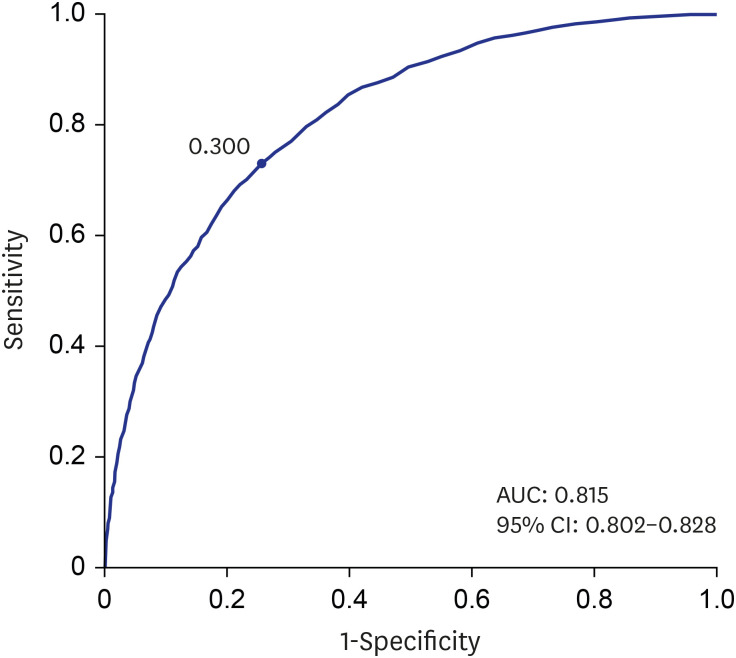 | Fig. 3 Receiver operating characteristic curve and accuracy of more than moderate BPD prediction in Korean Very Low Birth Weight Infants. BPD prediction equation is p = eQ1+eQ
|
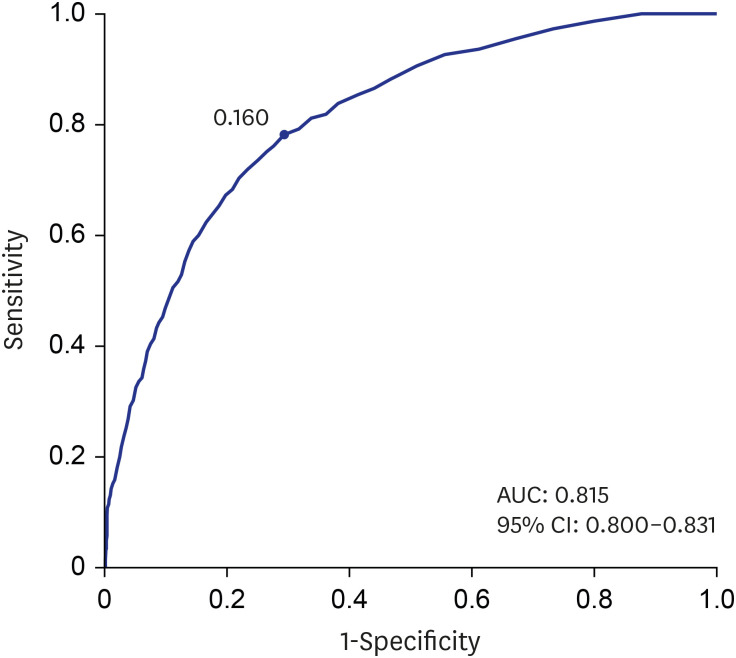 | Fig. 4 Receiver operating characteristic curve and accuracy of severe BPD prediction in Korean Very Low Birth Weight Infants. BPD prediction equation is p = eQ1+eQ
|
Table 1
Demographic characteristics of training dataset (n = 4,600)
Chi-square test and one-way ANOVA (P < 0.05). BPD represented as none (0), mild (1) moderate (2) severe (3).
GDM = gestational diabetes mellitus, DM = diabetes mellitus, PIH = pregnancy induced hypertension, HT = hypertension, BPD = bronchopulmonary dysplasia.
![]()
Table 2
Analysis in training dataset for each BPD grading
Multiple logistic regression (P < 0.05). BPD represented as none (0), mild (1) moderate (2) severe (3).
GDM = gestational diabetes mellitus, DM = diabetes mellitus, PIH = pregnancy induced hypertension, cHTN = chronic hypertension, LCL = lower cut-off limit, UCL = upper cut-off limit, BPD = bronchopulmonary dysplasia.
![]()
Table 3
Multivariate analysis by stepwise selection with significant clinical indicators for BPD prediction in training dataset
Stepwise variable selection method in logistic regression (P < 0.05). BPD represented as none (0), mild (1) moderate (2) severe (3).
LCL = lower cut-off limit, UCL = upper cut-off limit, BPD = bronchopulmonary dysplasia.
![]()
The stepwise selected clinical indicators were used for BPD prediction equation, and prediction rate was calculated as presented equation (Table 4). Moreover, it was used to search the best cut-off value and calculate the AUC as a prediction accuracy in each comparison. In case of prediction of any BPD, predictability is 90.8% and prediction P value cut off is 0.550 (Fig. 2). If using this equation, a P value more than 0.550 means that baby will be a BPD patient.
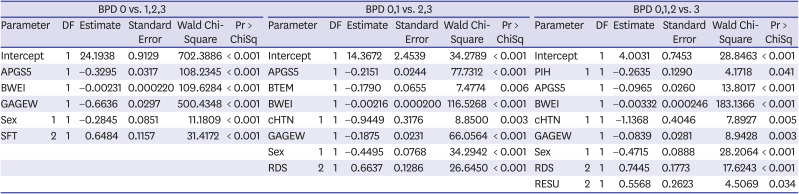
Table 4
Clinical indicators for BPD prediction equation in Korean very low birth weight infants
BPD represented as none (0), mild (1) moderate (2) severe (3).
APGS5 = 5 min Apgar score, RDS = respiratory distress syndrome, SFT = surfactant use, BWEI = birth weight, GAGEW = gestational age, BTEM = body temperature at admission, cHTN = maternal chronic hypertension, PIH = maternal pregnancy induced hypertension, RESU = need for resuscitation at birth, BPD = bronchopulmonary dysplasia.
![]()
In case of prediction of more than moderate BPD, predictability is 81.5% and prediction P value cut off is 0.300 (Fig. 3). If using this equation, a P value more than 0.300 means that baby will be treated until corrected 36 weeks gestation or 56 postnatal days with oxygen or ventilator. In case of prediction of severe BPD, predictability is 81.5% and prediction P value cut off is 0.160 (Fig. 4). If using this equation, a P value more than 0.160 means that baby will be treated until corrected 36 weeks gestation or 56 postnatal days with ventilator. This patient will have a chronic morbidity and mortality associated with BPD.
External validation
We were able to perform external validation with the 2017 KNN data,15 which included patients treated with the same treatment policy in Korean population. Data were collected for 2,075 VLBWIs with GA ≥ 22 weeks who were born between January 1, 2017 and December 31, 2017, and admitted to the neonatal intensive care units of the KNN. In 2017 KNN data analysis, there were 290 undefined BPD VLBWIs who died before 28 days. After all missing data were excluded, 1,740 VLBWIs were included in external validation (Fig. 5). Because of some clinical parameters, which were neonatal blood pH and BD, and maternal histological chorioamnionitis were not used to make prediction equation, we did not exclude infants with those missing data. Demographic pattern of test dataset (2017) was almost same as training dataset (2013–2016). In test dataset, about 57.6% Korean VLBWI have a BPD. All variables, except maternal DM, expressed worse severity of BPD (Table 5). Result of external validation presented as a sensitivity and specificity (Table 6). In case of prediction for present BPD, sensitivity slightly increased from 0.818 to 0.855. Specificity slightly decreased from 0.824 to 0.747. In the case of prediction for more than moderate BPD, sensitivity slightly decreased from 0.692 to 0.581. Specificity slightly increased from 0.779 to 0.837. In the case of prediction for severe BPD, sensitivity slightly increased from 0.782 to 0.797. Specificity slightly decreased from 0.706 to 0.748.

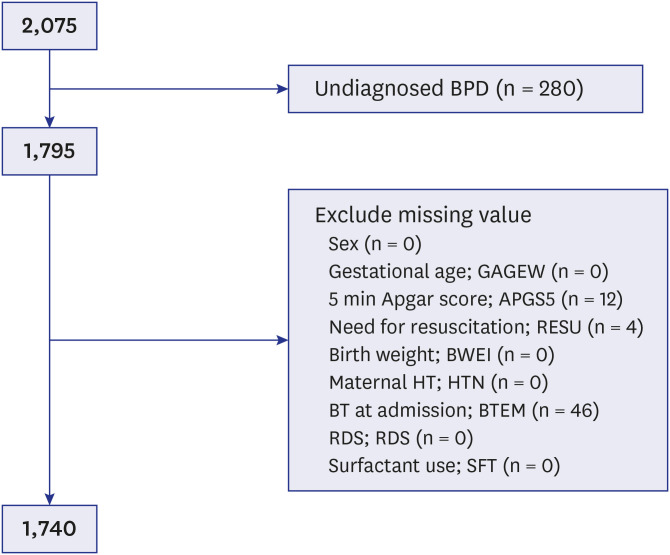 | Fig. 5Algorithm of selection in test dataset.BPD = bronchopulmonary dysplasia, HT = hypertension, BT = body temperature, RDS = respiratory distress syndrome.
|
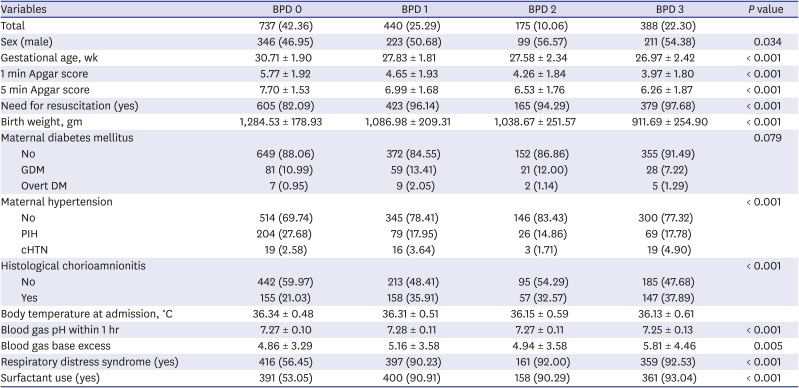
Table 5
Demographic characteristics of test dataset for external validation (n = 1,740)
χ2 test and one-way ANOVA (P < 0.05). BPD represented as none (0), mild (1) moderate (2) severe (3).
GDM = gestational diabetes mellitus, DM = diabetes mellitus, PIH = pregnancy induced hypertension, HT = hypertension, BPD = bronchopulmonary dysplasia.
![]()
Table 6
Comparison of sensitivity and specificity between training dataset and test dataset with developed prediction equation program
BPD represented as none (0), mild (1) moderate (2) severe (3).
TP = true positives, FN = false negatives, FP = false positives, TN = true negatives, BPD = bronchopulmonary dysplasia.
![]()
Go to :
DISCUSSION
Those 1,053 infants who died or were discharged before the diagnosis of BPD were excluded in the initial analysis, leaving 6,969 infants for analysis. The predictability of any BPD was 90.1% and more than moderate BPD was 80.5%. If we included only 4,600 infants with complete datasets, the predictability of any BPD was 90.5% and more than moderate BPD was 81.5%. Both were similar in predicting BPD but only the later set was included for analysis in this paper. Furthermore, the later data set was used because the range of GA (22.0–34.6 weeks) and birth weight (280–1,499 g) of the 6,969 infants was not different from the range of GA (22.1–34. 6weeks) and birth weight (280–1,499 g) of the 4,600 infants. Early death before the diagnosis of BPD were excluded from analysis in this study because they could not decide severity of BPD.
Many studies have addressed prediction of BPD, they each have employed different timing of evaluation, different factors, and different statistical methods but as mentioned in the review article by Onland et al.16 only two studies have validated their program with external data. As each patient has multiple variables such as unique disease sensitivity, treatment course, and race, it is quite difficult to predict BPD at an early age. Parker et al.17 used five clinical indicators at birth such as GA, birth weight, sex, race, RDS from several parameters. Percent explanation with complete data was 72% in one regional center for newborn care in America. Henderson-Smart et al.18 used only three clinical indicators at birth such as GA, birth weight, and sex. From their prediction model, area under the receiver operating characteristic (ROC) curve was 0.84 in Australia and New Zealand's population. In our study, AUC for prediction of present BPD was 0.908 in Korean population. Also, for prediction of more than moderate or severe BPD, AUC was 0.815. Chien et al.19 used five clinical indicators such as GA, sex, SGA, out-born status, 5-minute Apgar score and physiology-based parameters of SNAP-II during a 12-hour period. AUC for prediction of BPD by five clinical indicators with SNAP-II slightly increased to 0.83 compared to AUC without SNAP-II. It suggests that physiology-based parameters can improve prediction power. We chose several physiology-based parameters such as initial neonatal blood PH and BD with in the first hour, and body temperature at admission. There was only one indicator, body temperature at admission, used for prediction of more than moderate BPD. Recently, several biomarkers studied to identify for early diagnosis of BPD.20 Nevertheless, many of the studies were exploratory and performed in a very small number of patients. Disadvantages of using serum biomarker or OMICs technology related to challenge associated with sample collection and volumes needed. The meaning of this program is by using first 1 hour of data after delivery up to 90 percent of occurrence of BPD after corrected age of 36 weeks was predicted. This information may be used to select patients in need for early steroid treatments, novel neonatal therapeutics and focus on infection prevention and artificial ventilator managements. Using our prediction program, the predictability for BPD calculated from zero to one accordingly. The ROC curve, 95% CI of the AUC and the best cut-off values predicting the event was determined. The best cut-off values were determined according to the maximum AUC and AUC value depicts the prediction value of this prediction program. This will provide useful information for VLBWIs in the prediction of BPD as the predictability was not changed when tested in a different dataset for external validation. External validation of the prediction program carried out with a different data set of Korean VLBWIs other than the KNN dataset. The program demonstrated improved sensitivity and positive predictive value with the external data compared with the KNN data. The specificity of predicting severe and above BPD was improved. KNN database is Korea's one and only national network that includes almost 80% of the VLBWIs born in Korea and contains the clinical course, outcomes, and follow up data of more than 10,000 VLBWIs as of 2019. Furthermore, continuous accumulation of such clinical data will aid in improving the predictability of prediction programs in the future. However, as the pathogenesis of BPD is evolving and the change of diagnostic criteria is under discussion, the prediction program will subsequently need to evolve accordingly. Other papers have reported lower sensitivity and specificity after external validation. However, our external validation dataset was uniform as it was from a single institution and from a uniform race. Such factors contributed to higher sensitivity and specificity in our external data validation. Moreover, the advancement of neonatology in Korea with the help of KNN for the past five years have upgraded and standardized the medical care offered to the VLBWIs in Korea. Current literature describes novel therapeutics for BPD involving gene therapy, administration of deficient products and stem cell therapy. Early prediction of BPD using this program will be helpful in the selection of the high-risk group eligible for such novel therapies and anticipated to contribute to the earlier more aggressive management of high risk for BPD in Korean VLBWIs.
The limitations of this study are as follows; exclusion of death cases and not considering the clinical parameters that will affect the development of BPD during the NICU stay. Out of the 1,053 infants without data on BPD, 19 were of greater than 32 weeks gestation and 481 cases had incomplete data. Excluding those cases, we included the 533 deaths before 28 days under death of BPD, the predictability increased to 91.9% with a cutoff P value of 0.600. Longitudinal clinical parameters during the NICU stay were not included in the analysis because each NICU has a different treatment policy and individual response to those various treatments may decrease the overall predictability of BPD. The cause of effect of such treatments affecting the incidence of BPD may be vague. That is why only clinical parameters within the first hours of life were analyzed.
This study used data from KNN, a Korean national registry of VLBWIs and will provide the optimal prediction program for Korean VLBWIs as the racial and genetic differences in BPD prediction cannot be ignored. Furthermore, the data was analyzed in a stepwise fashion and externally validated. It was also found to have high predictability for severe or above BPD with data from 1 hour of life. Thus will prove to be useful in counselling family and selecting the high-risk population for clinical trials. Not only the continuous accumulation of KNN data and the subsequent increase in the study population but also the employment of AI programs will aid in prediction programs with higher predictability. It has the advantage of checking the prediction and the consistency with actual clinical results in advance. Up to this day, over 10,000 VLWBI data are gathered, and continuous gathering is expected to increase the predictability of the program, which also leads to increase in the BPD occurrence prediction. In addition, all the diseases show racial differences. This program will be helpful for Koreans or Asians since it contains oriental race. This factor is not provided by the current online NICHD BPD estimator. We are in the process of making comparative analysis between our prediction program and the NICHD BPD estimator and further develop our program using cumulative future KNN data.
Go to :
 XML Download
XML Download