

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In recent years, adolescent suicide mortality in Korea has been increasing, in contrast to the decreasing trend in other OECD member countries; therefore, it is important to investigate the risk factors for adolescent suicide in Korea.12 The identified suicide-related problems differ by sex. The suicide attempt rate among adolescents aged 10–19 years in the United States from 2000 to 2008 remained at 7.6 to 6.7 per 100,000 in males and 1.7 to 1.9 in females, whereas the suicide attempt rate among Korean adolescents aged 10–19 years increased from 4.2 to 6.9 per 100,000 in males and from 3.3 to 6.2 per 100,000 in females.3 It is known that females have more risk for suicide ideation than males, and males have more risk for suicide attempt than females.4
Previous studies reported that males are more likely to complete suicide than females, and a prior history of suicide attempts is known to be a significant predictor of future suicide attempts and suicide death.4567 Therefore, it is meaningful to identify the risk factors for increased suicide attempts in male adolescents.
Suicide-related ideation in adolescents is associated with various factors, including emotional problems, such as depression, and behavioral problems, such as conduct disorders and attention deficit hyperactivity disorder.5 Behavioral problems, which are more common than emotional problems in boys, are more likely to increase the risk of suicide attempts in boys than in girls.5 The increase in risky behavior is affected by gonadal changes in the pubertal period in boys.589
Spermarche is one of the features of puberty in males. Because during puberty boys experience several physiological changes (e.g., weight gain and physical changes related to gonadal hormones, such as penile hair growth) and psychological obstacles (e.g., poor body image and scholastic underachievement), they are likely to be psychologically instable in terms of social adjustment.10 To date, early puberty among boys has been reported to be related to externalizing symptoms (e.g., substance use and delinquency)1112; however, few studies have investigated the association between early spermarche and suicide attempts in boys.12 Previous studies on pubertal timing and suicide have focused on girls.11131415 Therefore, this study aimed to investigate the relationship between early spermarche and suicide attempts in boys by using representative data on Korean adolescents.
METHODS
Subjects
The Korea Youth Risk Behavior Web-Based Survey (KYRBS) is conducted annually to develop and improve adolescent health promotion policy in Korea. The KYRBS includes questionnaires evaluating the psychological and physical health-related behaviors of adolescents. Data collected via the KYRBS from 2011 to 2015 were used in this study. The KYRBS uses multistage cluster sampling to obtain nationally representative data. Students from 800 schools (400 middle schools and 400 high schools) comprising all the public and private middle and high schools in 17 provinces participate in the KYRBS. Approximately 35,000 boys (aged 12 to 17 years) participate in the KYRBS every year. The sampling error was minimized by extracting samples through the steps of population stratification, sample allocation, and sampling. Details about the KYRBS can be accessed on the website (http://yhs.cdc.go.kr).
Measurements
The timing of spermarche in the participants was evaluated by using the following question: “When did you experience your first ejaculation (i.e., spermarche)?” The questionnaire for evaluating spermarche was also used in the KYRBS. The response options were as follows: 1 (have not yet experienced ejaculation), 2 (before entering elementary school), and 3 to 14 (Grades 1 to 12, respectively). In a previous study, pubertal timing was defined as grade of first spermarche in boys.16 This same definition was applied, and the average grade of the first spermarche was calculated for all subjects except those who had not yet experienced spermarche. The participants were divided into four groups based on the average grade at spermarche: group 1 (spermarche occurred earlier than the average grade), group 2 (average), group 3 (spermarche occurred later than the average grade), and group 4 (had not yet experienced).16
Self-reported questionnaires were used to investigate the perceived stress, depressive symptoms, suicidal ideation and suicide attempts experienced by the subjects. Perceived stress was assessed by the question “How much stress do you usually feel?.” The response options were as follows: 1, “I feel so much”; 2, “I feel a lot”; 3, “I feel a little”; 4, “I do not feel much”; and 5, “I do not feel it at all.” The subjects were divided into two groups: the high-stress group (1–2) and the low-stress group (3–5). Depressive symptoms were evaluated with the question “Have you experienced despair strong enough to interrupt daily life for more than two weeks within the last 12 months?” The response options were ‘yes’ or ‘no.’ Suicidal ideation and suicide attempts experienced during the prior 12 months were evaluated with the questions “Have you seriously thought about suicide within the last 12 months?” and “Have you attempted suicide within the last 12 months?” The response options were ‘yes’ or ‘no.’
Statistical analysis
Complex sampling procedures were used to analyze the raw data, which were collected by a complex sampling design. Stratified variables, clustered variables, and weighted variables were included in these analyses. The t-tests and χ2 tests were performed to compare the mean age, perceived stress (high), suicidal ideation (yes), and suicide attempts (yes) between groups 1 and 2 in each year. Complex sampling logistic regression analyses were performed to compare the odds ratios (ORs) of suicidal ideation and suicide attempts between groups 1 and 2 with a 95% confidence interval (CI). Covariates were included in the analyses: in the analysis for suicidal ideation, age, perceived stress, and depressive symptoms were included as covariates; in the analysis for suicide attempts, age, perceived stress, depressive symptoms, and suicidal ideation. All statistical analyses were performed using SPSS version 21.0 (IBM Corporation, Armonk, NY, USA), and two-tailed P values less than 0.05 were considered indicative of statistical significance.
RESULTS
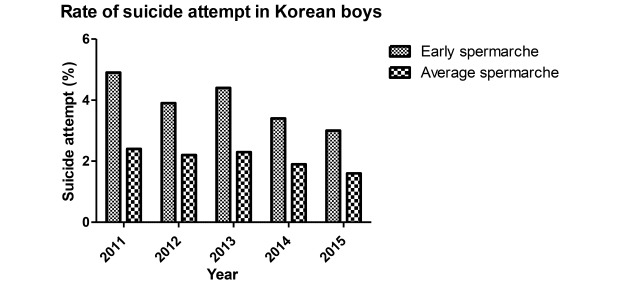
The mean age (mean ± standard error) of the subjects in each year was as follows: 2011 (15.1 ± 0.0); 2012 (15.0 ± 0.0); 2013 (15.0 ± 0.0), 2014 (15.0 ± 0.0), and 2015 (15.1 ± 0.0). The mean grade of pubertal timing (mean ± standard error) in each year was as follows: 2011 (9.1 ± 0.0); 2012 (9.1 ± 0.0); 2013 (9.1 ± 0.0), 2014 (9.0 ± 0.2), and 2015 (9.0 ± 0.2). The number of boys included in groups 1 and 2 in each year was as follows: 2011 (6,099, 5,924); 2012 (5,971, 5,665); 2013 (5,721, 5,289); 2014 (5,746, 4,998); and 2015 (5,562, 4,819). The number of subjects with suicide attempts in each year was as follows: 2011 (1,167, 3.0%); 2012 (1,062, 2.8%); 2013 (1,065, 2.8%); 2014 (839, 2.3%); and 2015 (679, 2.0%). The demographic and clinical characteristics of the participants are presented in Table 1. In 2011, the mean age was not significantly different between groups 1 and 2; other variables, including perceived stress, depressive symptoms, suicidal ideation, and suicide attempts, were significantly different between groups 1 and 2. In all years except 2011, significant differences in age, perceived stress, depressive symptoms, suicidal ideation, and suicide attempts were found between groups 1 and 2. Subjects with suicide attempts were significantly more common in groups 1 than in 2 in all years (2011–2015, P for all < 0.001). Generally, depressive symptoms, suicidal ideation, and suicide attempts were more common, while perceived stress was less common in groups 1 than in 2 (Table 2). Regarding the results of the complex sample logistic regression analyses of the boys, the ORs (95% CI; P value) of suicide ideation in group 1 compared with those in group 2 were as follows: 1.243 (1.122–1.378; P < 0.001) in 2011; 1.239 (1.101–1.394; P < 0.001) in 2012; 1.265 (95% CI, 1.117–1.432; P < 0.001) in 2013; and 1.324 (95% CI, 1.133–1.548; P < 0.001) in 2015. In 2014, the OR for suicide ideation in Group 1 was not significant (OR, 1.118; 95% CI, 0.969–1.289; P = 0.126). The ORs for suicide attempts in Group 1 compared with those in group 2 were as follows from 2011 to 2015: 1.782 (1.429–2.223; P < 0.001), 1.490 (1.159–1.917; P = 0.002), 1.693 (1.336–2.144; P < 0.001), 1.541 (95% CI, 1.187–2.003; P = 0.001), and 1.393 (95% CI, 1.024–1.895; P = 0.035) (Table 3). The ORs for suicide attempts in group 1 were significant in all years.
Table 1
Demographic and clinical characteristics of the participants
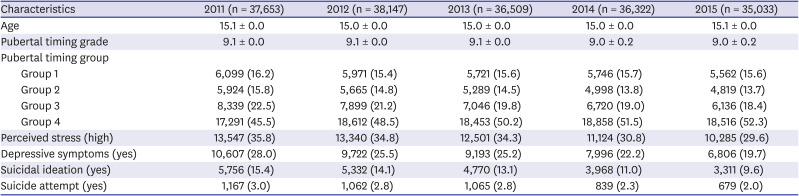
Data are presented as mean ± standard deviation or number (%). The participants were divided into four groups based on the average grade at spermarche: group 1 (spermarche occurred earlier than the average grade), group 2 (average), group 3 (spermarche occurred later than the average grade), and group 4 (had not yet experienced spermarche).
Table 2
Comparison of perceived stress (high), depressive symptoms (yes), suicidal ideation and suicide attempts (yes) between the early spermarche group and the average spermarche group
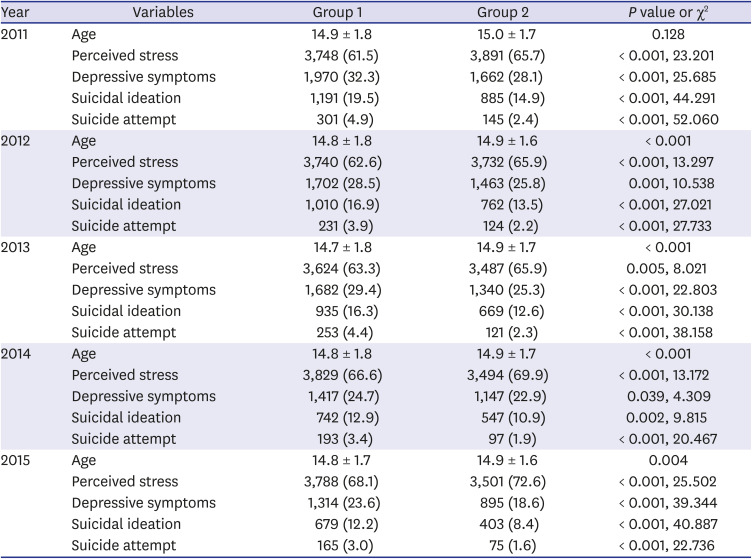
Data are presented as mean ± standard deviation or number (%). The participants were divided into four groups based on the average grade at spermarche: group 1 (spermarche occurred earlier than the average grade), group 2 (average), group 3 (spermarche occurred later than the average grade), and group 4 (had not yet experienced spermarche) (data of groups 3 and 4 are not shown in this table).
Table 3
Associations between early pubertal timing and suicide attempts in Korean boys using complex sample logistic regression

DISCUSSION
This study is the first to investigate the association between early spermarche and suicide attempts in Korean boys. In addition, this study is meaningful in that it uses the data from a representative consecutive survey conducted in Korea from 2011 to 2015. The results of this study show that boys with early spermarche had a higher risk of suicide attempt than boys with average spermarche. In some previous studies, early spermarche among boys was correlated with various psychological states (such as depression, substance use and delinquency) that increase suicide risk, as well as with suicide attempts.1112 However, in this study, the higher risk for suicide attempt in the early spermarche group was the result after adjusting for confounding factors such as age, depressive symptoms, perceived stress, and suicide ideation. This result indicates that suicide attempt was independently associated with early spermarche in boys, even when the effect of psychiatric symptoms, such as depressive symptoms, a high level of stress, and suicidal ideation, was considered.
In the pubertal period, boys experience psychological instability and physically embarrassing changes (such as spermarche and penile hair growth), which indicate biological exposure to sex hormones.17 Early exposure to sex hormones could negatively affect brain development in the growth period of boys and increase risk-taking behaviors. In particular, testosterone may be associated with suicide. Puberty is a phase marked by a rapid increase in testosterone levels and hormonal changes.8 High levels of testosterone work on the central nervous system to increase impulsivity, aggression, and suicide-related problems in boys with early spermarche.8 Impulsivity and risk-taking behavior are increased by early exposure to gonadal hormones and could be relevant to the results of this study, which reported a higher risk of suicide ideation/attempts in boys with early spermarche after adjusting for depressive symptoms and perceived stress.
Previous studies have suggested that puberty-induced gonadal hormone changes may affect brain development and influence the development of complex behavioral and emotional patterns that comprise various psychopathologies.121819 There is a difference in the maturation process of the two neural systems associated with the dopaminergic pathway influenced by gonadal hormone changes during puberty.202122 Social information processing and reward sensitivity (governed by subcortical limbic structures) in the brain undergo increased development in early to mid-adolescence, and in contrast, cognitive control systems (governed by the prefrontal cortex) develop more linearly across adolescence.202122 Gonadal hormones, which increase during puberty, have important effects on the arousal of the socioemotional network through heightened activation of areas including the limbic system.20 Therefore, adolescents who undergo early maturation may experience greater gonadal hormone effects on the subcortical limbic system while continuing to have a less developed cognitive control system.1218 Such development patterns are related to impulsive or increased risk-taking behaviors and increased emotional arousal that may influence vulnerability to various psychopathologies.1223 To date, studies have supported a positive relation between risk-taking and suicidal ideation/behaviors.2425 Risk-taking behaviors may represent a vulnerability to act impulsively on suicidal ideation.24 Meta-analytic findings have shown that typically developing males are more prone to risk-taking than females, although the size and significance of the effects differed.2627
In addition, the temporary imbalance of dopamine receptors between the prefrontal cortex and the striatum that occurs in puberty may have important implications for reward processing in adolescence (e.g., reward deficiency syndrome). Something, such as a sense of social recognition, may activate the same neural circuitry implicated in reward processing; thus, risk-taking behavior within peer groups may increase in puberty.20 Previous studies showing that boys are more sensitive to peer pressure in the context of risk-taking than girls are significantly more numerous than studies showing the opposite result.26 Additionally, maturation of the prefrontal cortex occurs at an earlier age in girls than in boys.28 That is, boys may be more susceptible to peer pressure than girls because of differences in coping skills and regulatory capabilities.26
This study has several limitations that are worth mentioning. First, it was difficult to evaluate the psychopathologies in detail because this study used a simple-structured self-report questionnaire related to depressive symptoms and perceived stress. However, as mentioned in a previous study,15 the results showed a general consistency from 2011 to 2015; therefore, this study suggests the probability of a significant association between early spermarche and suicide attempts in boys. This study also used a single-item, self-administered questionnaire to assess pubertal timing as grade at spermarche or have not yet experienced. Other measures or dimensions of pubertal timing (e.g., subjective pubertal timing, secondary sex characteristics, Tanner stage, pubertal development scale) may be superior.16 However, many previous studies have evaluated pubertal timing in boys using age at spermarche.16293031 Second, only depressive symptoms and perceived stress were adjusted for in this study. It is known that depression and emotional symptoms have a stronger association with suicide in girls than boys.5 Other factors could not be adjusted since this study was based on existing data. Adolescents with conduct disorder have an increased risk of suicide attempts.32 Previous studies have shown conduct disorder to be more prevalent among boys than girls.3334 Therefore, additional studies that adjust for conduct problems are recommended. Finally, it is not possible to confirm any correlation between suicide attempts and neurobiological changes in boys with early spermarche because this study is based only on demographic information.
Despite these limitations, considering that previous studies have shown consistent results regarding the positive relationship between suicide and early pubertal timing in girls,1314 this study showed a higher risk of suicide attempts in boys with early spermarche. This suggests that screening for early secondary sexual characteristics might be helpful for preventing suicide-related problems in adolescents. However, further research on neurobiological evidence of this association will be necessary.
 XML Download
XML Download