

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Suicide does not occur abruptly but instead is the final point of a trajectory called the suicidal process.1 The suicidal process begins with hopelessness and then transient suicidal ideation, which further develops into a suicidal plan and a suicide attempt, often leading to a reattempt with increased resolve and lethality. Each step of the process—suicidal ideation, suicide attempt, and suicide—share many common risk factors, and yet dissimilarities do exist.2 Thus, understanding suicidal ideation and the factors contributing to it can help prevent the process even from starting. A number of studies have identified risk factors for suicidal ideation.2 Psychosocial factors include hopelessness3 and stress.4 Clinical factors include psychiatric disorders such as major depressive disorder, anxiety disorders, substance use disorder,5 and chronic medical illness.6 Evidence has been accumulating that early trauma (ET) is associated with subsequent psychiatric conditions such as suicidality,7 including suicidal ideation,8 and specific psychiatric disorders, including depressive disorder and anxiety disorder,7 both of which are contributors to suicidal ideation.5 The presence or absence of ET therefore implies unique characteristics in the relationships between suicidal ideation and its risk factors.
Considering the lifelong effects of ET, such as an increase of trait impulsivity,9 differentiating between groups affected and unaffected by ET could help us both develop group-specific anti-suicidal strategies and deepen our knowledge of the consequences of devastating life events. However, despite the potential disparities between groups in terms of the presence or absence of ET, a paucity of studies separately conducted on each group leaves a gap in the literature examining potential relationships between suicidal ideation and its contributors. To our knowledge, only one study was performed specifically on victims of ET, showing associations of resilience, marital status, ET-related shame, and family support with suicidal ideation10; no such study was performed on non-victims of ET. Moreover, no study using two samples similar in composition (e.g., clinical/non-clinical status or ethnicity) but different in terms of the presence or absence of ET has collectively and simultaneously examined the relationships between suicidal ideation and contributing state (vs. trait) variables. In addition, even within the group of victims of ET, gender differences in aspects of suicidality are well-documented. ET has more harmful effects on women,11 including long-term deleterious consequences such as suicidal behavior.12 Females may be more likely to blame themselves for ET, and self-blame might increase risks for later hardship, possibly including suicidal behavior.13 A recent longitudinal study showed that ET is associated with later suicide attempts only in females.13 Depression, hopelessness, and familial dysfunction are stronger mediating factors for females than for males in the relationship between childhood sexual abuse and later suicidality in particular.14 Thus, stratification by gender appears to be necessary for better analysis of possible consequences of ET.
In the present study, we focused on three variables—recent stress, depressive symptoms, and anxiety symptoms—because they are well-established risk factors of suicidal ideation.151617 They are almost always evaluated in any psychiatric interview, making them clinically valuable. We chose to focus on adult females because the literature reports that they experience more catastrophic consequences of ET in terms of suicidality; understanding their problems is clinically urgent. Using data from suicidal ideators and suicide attempters, the current study investigated the contribution of the three factors to suicidal ideation within each group—female victims and non-victims of ET—without a between-group comparison. Based on previous studies, the researchers hypothesized that recent stress would present both a direct and an indirect relationship with suicidal ideation through depressive symptoms and anxiety symptoms. To evaluate interconnected relationships among multiple variables, the researchers employed the structural equation model (SEM), a statistical method that simultaneously examines associations among multiple variables. The results will help to develop in-depth interpretations of the consequences of ET and lay the groundwork for comparisons with other groups.
Go to : 
METHODS
Participants
This study was a secondary analysis of the Korean Cohort for the Model Predicting a Suicide and Suicide-related Behavior (K-COMPASS), a prospective cohort study aiming to identify predictors for suicide attempts and suicide. Participants were recruited from patients in eight university hospitals and visitors to eight community mental health welfare centers in the Republic of Korea from September 2015 to March 2018. The inclusion criteria comprised two suicidal groups: suicidal ideators, who had current, serious suicidal ideation and had not attempted suicide within one month from the enrollment day, and suicide attempters, who made at least one attempt during the same period. The time frame of one month was determined based on the intensity subscale of the Columbia-Suicide Severity Rating Scale, the measurement tool of suicidal ideation employed in the present study, as the subscale is originally designed to evaluate suicidal ideation during the last month. In evaluating suicidal ideation, it was not considered whether a suicidal plan was accompanied. Individuals with a history of intellectual disability or organic brain damage and people incapable of understanding Korean were excluded. For a comprehensive summary of the data collection procedure and participants' baseline characteristics, see our previous report.18 Participants were 351 women aged 18 years or older, 217 victims of ET and 134 non-victims of ET.
Measurements
Early Trauma Inventory Self-Report-Short Form (ETISR-SF)
The ETISR-SF is a 27-item self-report questionnaire for assessing traumatic events suffered before the age of 18.19 Respondents are classified as victims of ET only if they report having undergone intense fear, horror, or helplessness and felt depersonalization or derealization at the time of the event. Otherwise, they are defined as non-victims of ET.
Stress Questionnaire for Korean National Health and Nutrition Examination Survey-Short Form (SQ for KNHANES-SF)
The SQ for KNHANES-SF is a self-report instrument evaluating the level of stress during the last month.20 Nine items are rated on a 5-point scale from 0 (“never”) to 4 (“very often”). The total score ranges from 0 to 36, with a higher score referring to a greater level of recent stress. Cronbach's alpha in the present sample was 0.862 and 0.866 for non-victims and victims of ET, respectively, indicating good internal consistency in both.
Patient Health Questionnaire-9 (PHQ-9)
The PHQ-9 is a nine-item self-report measure of depressive symptoms.21 Each item is rated on a 4-point scale from 0 (“not at all”) to 3 (“nearly every day”) on the basis of symptom frequency during the last two weeks. The overall score ranges from 0 to 27. Cronbach's alpha for the scale in the current sample was 0.819 and 0.797 for non-victims and victims of ET, respectively, indicating good internal consistency in both.
Beck Anxiety Inventory (BAI)
The BAI is a 21-item self-report rating scale of anxiety symptoms.22 Each item is rated on a 4-point scale from 0 (“not at all”) to 3 (“severely—it bothered me a lot”) based on symptom severity during the last two weeks. The total score ranges from 0 to 63. To improve quality of items and model fit, we employed item parceling,23 adopting the previous findings and factoring items in four dimensions: subjective, neurophysiological, autonomic, and panic anxiety.24 Cronbach's alpha for the scale in the present sample was 0.873 and 0.888 for non-victims and victims of ET, respectively, indicating good internal consistency in both.
Columbia-Suicide Severity Rating Scale (C-SSRS)
The C-SSRS is a semi-structured, rater-administered instrument for measuring suicidal ideation2526 that includes severity and intensity subscales. We used the intensity subscale, composed of five items about suicidal ideation during the last month, “Frequency,” “Duration,” “Controllability,” “Deterrents,” and “Reasons for Ideation.” The first two items are rated on a 5-point scale from 1 to 5, and the rest are rated on a 6-point scale from 0 to 5. The total score ranges from 0 to 25 (0 when the severity subscore is 0), with a higher score indicating a greater degree of suicidal ideation. Cronbach's alpha for the scale in the present sample was 0.576 for non-victims of ET and 0.446 for victims of ET, indicating poor and unacceptable internal consistency, respectively. We removed Item 4, “Deterrents,” and Cronbach's alpha became 0.503, still poor but considered acceptable. Because internal consistency tends to be underestimated in cases of a small number of items, it is problematic to routinely apply the widely used cut-off of 0.7 or 0.627; accordingly, a few papers reported the value ≥ 0.45 as acceptable or sufficient.28 Thus, we decided to accept the present values, taking into consideration the limited number of items.
Statistical analysis
Descriptive statistics of baseline characteristics were used to present sociodemographic factors. We performed Pearson's correlation analyses to evaluate the relationships among all the SEM variables used to construct a hypothesized model with multiple mediators (depressive and anxiety symptoms). The degree of multicollinearity between the three variables (recent stress, depressive symptoms, and anxiety symptoms) and suicidal ideation was quantified using the variance inflation factor (VIF). Each model for non-victims and victims of ET was tested through structural equation modeling to examine the contribution of recent stress to suicidal ideation and the mediating role of depressive and anxiety symptoms on the relationship.
We used the statistical package IBM SPSS Amos 2.0.0 (SPSS, Inc., Chicago, IL, USA) for SEM. SEM simultaneously examines the relationships among variables by combining multiple regression and latent factor analysis.32 First, SEM constructs a hypothesized model, where a variable can function as a dependent or independent variable at the same time depending on the relationships with other variables; second, it decides whether data accord with the hypothesized model. To test whether the model was adequate, we used the Tucker-Lewis index (TLI) ≥ 0.90, comparative fit index (CFI) ≥ 0.90, and root mean square error of approximation (RMSEA) ≤ 0.08. Attempts to improve the goodness of fit were performed in the following order. An item whose relationship with a corresponding latent variable did not achieve statistical significance, or whose standardized factor loading was < 0.45, was eliminated from the model (Item 9 of the SQ for KNHANES-SF, Items 3 and 4 of the PHQ-9, and Items 3, 4, and 5 of the C-SSRS in the victims of ET). Subsequently, attempts were repeated by adding an inter-error covariance path according to the Amos modification index indicating the path, until the acceptable values were produced. Bootstrapping was performed to test mediation effects with a phantom variable approach. All statistical analyses except for structural equation modeling were performed using SPSS version 21.0 for Windows (SPSS, Inc.). A P value < 0.050 was considered statistically significant, and all tests were two-tailed.
Ethics statement
This study was approved by the institutional review boards of Seoul National University Hospital (H-1505-050-671) and all other participating study sites. Study participants' written informed consent, or that of their legal guardians in the case of 18-year-old participants, was obtained.
Go to :
RESULTS
Sociodemographic characteristics of participants
Participants' sociodemographic characteristics are shown in Table 1. No statistical difference was found in distributions of the cohorts to which they belonged (χ2 = 2.989; P < 0.084), indicating that they are similar in clinical/non-clinical status.
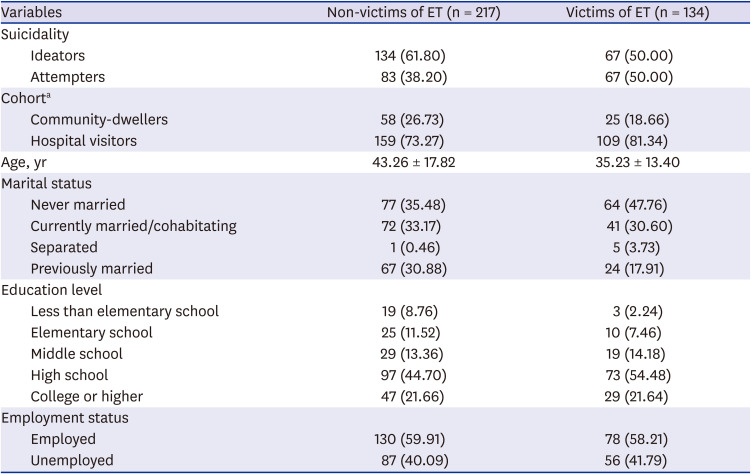
Table 1
Sociodemographic characteristics of participants
Data are presented as number (%).
ET = early trauma.
aPearson's χ2 test; χ2 statistic = 2.989; P = 0.084.
![]()
Bivariate analyses
The means and standard deviations (SDs) of the SEM variables and their correlations are presented in Table 2. Each variable was positively correlated with all other variables achieving statistical significance. The degrees of the VIF were all under 2, which indicates no multicollinearity between recent stress, depressive symptoms, anxiety symptoms, and suicidal ideation.
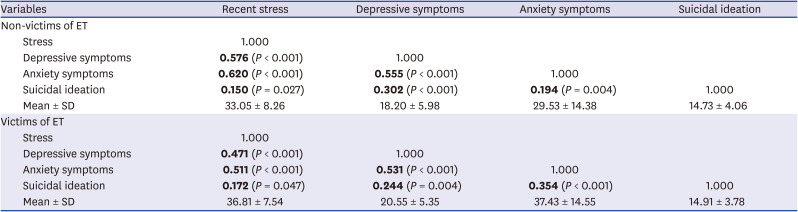
Table 2
Means, SD, and correlations between all study variablesa
![]()
SEM
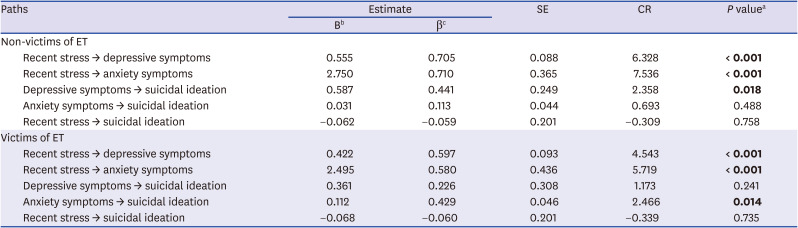
For non-victims of ET, the initial model failed to show a model fit adequacy: TLI = 0.840; CFI = 0.855; RMSEA = 0.068. Subsequent models were constructed and modified by the aforementioned procedures. The final model (Fig. 1) demonstrated an adequate model fit: TLI = 0.900; CFI = 0.913; RMSEA = 0.060. Unstandardized (B) and standardized (β) regression coefficients for the final model are given in Table 3. Recent stress directly predicted depressive symptoms (β = 0.705; standard error [SE] = 0.088; P < 0.001) and anxiety symptoms (β = 0.710; SE = 0.365; P < 0.001) each, with the former in turn influencing suicidal ideation (β = 0.441; SE = 0.249; P = 0.018).
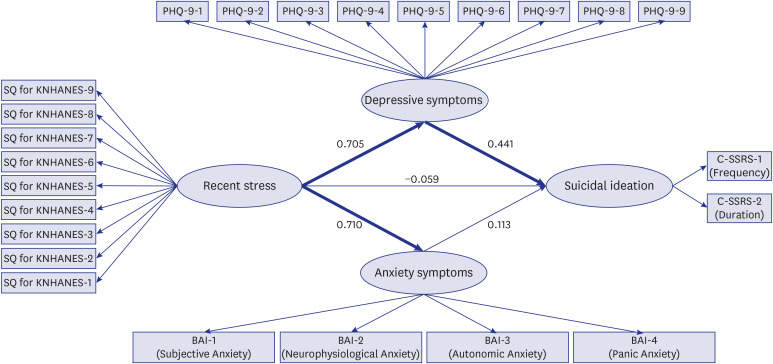 | Fig. 1SEM with standardized parameter estimates for relationships among stress, depressive symptoms, anxiety symptoms, and suicidal ideation for non-victims of ET. Thick lines connecting latent variables indicate significant path estimates (P < 0.050).SEM = structural equation model, ET = early trauma, PHQ-9 = Patient Health Questionnaire-9, SQ = Stress Questionnaire, KNHANES = Korean National Health and Nutrition Examination Survey, C-SSRS = Columbia-Suicide Severity Rating Scale, BAI = Beck Anxiety Inventory.
|
Table 3
Unstandardized and standardized regression coefficients for all pathways of the final SEM
SEM = structural equation model, SE = standard error, CR = critical ratio, ET = early trauma.
aSignificant findings at P < 0.050 are in bold; bUnstandardized regression coefficient; cStandardized regression coefficient.
![]()
For victims of ET, the model fit of the initial model also turned out to be inadequate: TLI = 0.794; CFI = 0.814; RMSEA = 0.082. After a series of model modifications, the final model (Fig. 2) showed adequate fit: TLI = 0.903; CFI = 0.917; RMSEA = 0.066. Recent stress was directly associated with depressive symptoms (β = 0.597; SE = 0.093; P < 0.001) and anxiety symptoms (β = 0.580; SE = 0.436; P < 0.001), with the latter in turn predicting suicidal ideation (β = 0.429; SE = 0.046; P = 0.014).
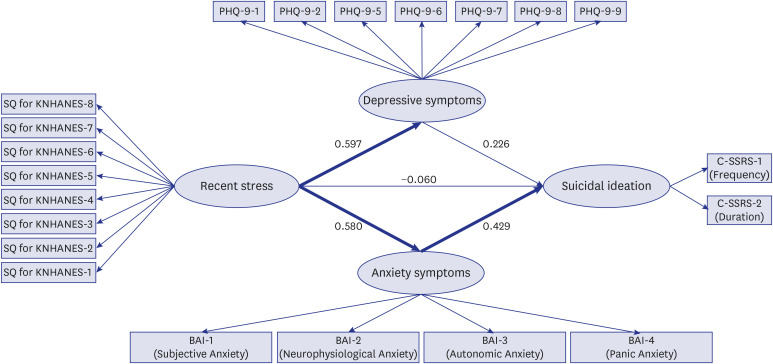 | Fig. 2SEM with standardized parameter estimates for relationships among stress, depressive symptoms, anxiety symptoms, and suicidal ideation for victims of ET. Thick lines connecting latent variables indicate significant path estimates (P < 0.050).SEM = structural equation model, ET = early trauma, PHQ-9 = Patient Health Questionnaire-9, SQ = Stress Questionnaire, KNHANES = Korean National Health and Nutrition Examination Survey, C-SSRS = Columbia-Suicide Severity Rating Scale, BAI = Beck Anxiety Inventory.
|
The results of multiple mediation analyses are summarized in Table 4. For non-victims of ET, there was only an indirect pathway from recent stress to suicidal ideation (B = 0.326; SE = 0.160; bootstrap 95% confidence interval [CI] = 0.090–0.790; P = 0.002), meaning that depressive symptoms fully mediated the relationship between recent stress and suicidal ideation. For the victims of ET, only an indirect pathway occurred from recent stress to suicidal ideation (B = 0.281; SE = 0.127; bootstrap 95% CI = 0.081–0.631; P = 0.005), indicating that the relationship between recent stress and suicidal ideation was fully mediated by anxiety symptoms.

Table 4
Multiple mediation analysis of the final SEM
SEM = structural equation model, SE = standard error, CI = confidence interval, ET = early trauma.
aUnstandardized regression coefficient; bSignificant findings at P < 0.050 are in bold.
![]()
Go to :
DISCUSSION
The purpose of the current study was to explore the associations between psychological factors and suicidal ideation among suicidal non-victims of ET and suicidal victims of ET by using SEM. As a multi-group analysis was not performed, an interpretation by each individual model, not a between-group comparison, was conducted. We tested depressive symptoms and anxiety symptoms as mediators of the relationship between recent stress and suicidal ideation, which has implications for tailored anti-suicidal strategies. Recent stress demonstrated only an indirect effect through depressive symptoms for non-victims of ET and anxiety symptoms for victims of ET, suggesting that the link between recent stress and suicidal ideation was fully mediated by depressive symptoms and anxiety symptoms, respectively.
Among the victims of ET, recent stress was directly associated with depressive symptoms and anxiety symptoms, which is consistent with earlier findings. A causal relationship has been established between stressful life events and major depressive episodes; significant stressors were found in both clinical and non-clinical samples.33 Several studies have reported the association between certain types of stressful life events and anxiety disorder34 or anxiety symptoms35 and between general stress and anxiety symptoms.36 However, contrary to previous results indicating that the severity of depressive symptoms is a contributor to suicidal ideation,1516 depressive symptoms did not have a direct effect on suicidal ideation in our sample. Our finding could be attributable to two factors. First, a limitation in accurately defining the construct “depressive symptoms,” based on the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition,37 criteria, appears to have occurred, because Item 3 of the PHQ-9 on sleep, and Item 4 on appetite, were eliminated to improve model fit. Insomnia in particular is associated with suicidal ideation among patients with depression.38 Likewise, from the intensity subscale of the C-SSRS, only two observed variables, “Frequency” and “Duration,” were used to measure the corresponding construct, suicidal ideation. Although many studies used each of the five items separately,3940 and one study left out “Reasons for ideation” and employed only four items to define suicidal ideation,41 we cannot exclude the possibility that there is a limitation in accurately representing the construct with only the remaining two items. In addition, depressive symptoms did not present a mediating effect on the association between recent stress and suicidal ideation, contrary to the previous results showing a full mediation42 or a partial mediation4344 depending on the group. Taking into consideration the presence of difference by groups, we speculate with caution that the absence of a mediating role of depressive symptoms might be a unique characteristic of suicidal victims of ET, suggesting the need for further studies on different groups to obtain an in-depth understanding of the mediating effect of depressive symptoms.
On the other hand, our study produced a novel finding: among victims of ET, recent stress had only an indirect effect on suicidal ideation, with the relationship fully mediated by the increase in the level of anxiety symptoms caused by stress. According to the diathesis-stress model, victims of ET have a vulnerability to suicide through increased impulsivity.45 When exposed to stress, they may suddenly undergo an intolerable emotional experience, distinct from depression.46 The psychological literature depicts suicide as “a combined movement toward cessation and away from intolerable, unendurable, unacceptable anguish,”47 and several psychoanalytic papers describe this emotional state using the term “anxiety.”46 Sigmund Freud called the state “traumatic anxiety,” where emotion is overexcited beyond a range mental apparatus can control,48 and Margaret Little used the term “annihilation anxiety”49 to describe feelings of terror.48 Collectively, when those with diathesis, or a vulnerability to suicide (such as victims of ET), experience severe stress, they suffer from agony including anxiety; their way of thinking loses flexibility, they fail to contemplate alternatives, and consequently they have suicidal thoughts or ideation.48 Moreover, according to recent biological findings, early traumatic experiences increase trait anxiety by affecting development of behavioral and emotional traits through epigenetic regulation.50 People with an increased level of trait anxiety have a tendency, or diathesis, to experience symptoms of state anxiety in stressful, threatening circumstances,5152 and it appears that the symptoms at that moment are similar to the anxiety mentioned in the psychoanalytic literature.
From the current findings, whether the victims of ET develop suicidal ideation under recent stress entirely depends on the level of anxiety symptoms. Facing stress in everyday life is almost unavoidable; therefore, we suggest that mental health professionals focus on reducing anxiety symptoms to prevent the development of suicidal ideation. A few studies have addressed various aspects of anxiety-reducing intervention for the victims of ET. The way a history of ET influences, or does not influence, response and treatment processes varies according to treatment modality. For victims with a history of emotional abuse who experience social anxiety disorder, antidepressant treatment is more likely to produce higher symptom improvement.53 On the other hand, a history of ET in those with social anxiety disorder does not affect responsiveness to cognitive behavior therapy.54 A recent study on children showed the effect of physical exercise on reducing anxiety among victims of ET.55 However, no studies have been performed on anxiety-reducing treatment for adult victims of ET with accompanying suicidality. An evidence-based modality of treatment of anxiety symptoms, whether pharmacological or psychosocial, would be recommended until further evidence accumulates.
Whereas anxiety symptoms had a mediating role on the relationship between recent stress and suicidal ideation, depressive symptoms did not. That appears to imply an existence of a subtype of depression not fully detected by the PHQ-9. A major depressive episode is heterogeneous; there are many subtypes, among which mixed depression refers to severe depression accompanied by psychomotor or inner excitation.56 Psychomotor excitation can emerge as physical agitation or psychological tension.57 Mixed depression is not only distinct from the traditional melancholic subtype58 but also associated with severe clinical conditions including a high risk of suicide.59 The prevalence of mixed depression was reported to be high among suicide attempters60; as 42.7% of our participants were suicide attempters, a substantial proportion likely had mixed depression. Further, agitation is a well-known symptom of mixed states,61 including mixed depression, and suicide attempters with mixed depression in particular are 61.1 times more likely to experience psychomotor agitation than those with non-mixed depression.60 Therefore, it is crucial to identify mixed depression and agitation; however, the use of the self-rating PHQ-9 is limited in its ability to identify either. Because agitation, especially restless movement,62 is not a subjectively reported feeling but an objectively observed behavior,63 self-judgment is fundamentally unable to measure it. In addition, mixed depression cannot be accurately assessed with a scale like the PHQ-9 that includes diagnostic criteria only of a major depressive episode, one that lacks manic or hypomanic symptoms. Accurate identification and measurement of mixed depression using a tool with items specifically assessing the subtype characterized by agitation, such as the Koukopoulos Mixed Depression Rating Scale,57 might have produced a different result in the association between recent stress and suicidal ideation. In addition, according to many sources, one of the emotions associated with agitation is anxiety,63 and severe anxiety manifests as agitation with motor symptoms.64 Because agitated people generally feel anxious,65 the possibility that agitation in mixed depression is partly reflected in the BAI score cannot be excluded. According to the finding of a factor analysis performed using all items from the BAI and the Beck Depression Inventory-II (BDI-II),66 the item “agitation” in the BDI-II and five items out of the BAI constitute the “subjective anxiety” factor,67 supporting the possibility that the characteristic aspect of mixed depression—agitation—might have been measured as anxiety symptoms in the present study.
Among the non-victims of ET, recent stress was also directly associated with depressive symptoms and anxiety symptoms, which corresponds with earlier findings.33343536 In addition, depressive symptoms fully mediated the association between recent stress and suicidal ideation, consistent with a previous result.42 As in the aforementioned discussion about victims of ET, this might also be a distinct characteristic of suicidal non-victims of ET. Anxiety symptoms did not affect suicidal ideation, which was different from the finding about victims of ET. Nevertheless, we cannot determine from the current study design whether there is a statistical difference between the two groups in the path from anxiety symptoms to suicidal ideation. However, based on earlier findings, we speculate cautiously that the effect of anxiety symptoms on suicidal ideation might differ according to the presence or absence of ET. One study reported that anxiety does not have a direct but an indirect effect on suicidal ideation by increasing rumination,68 which is a tendency to appraise problems repetitively without acting to change them. Rumination prolongs depressive mood69 and is regarded as a dimension in forming schemas of negative emotion.70 A stronger ruminative response style is found among victims of ET,71 and rumination mediates the association between severity of ET and suicidal ideation,8 implying a potential between-group difference in the effect of rumination on the suicidality path, a difference that needs to be studied further.
Last, contrary to our hypothesis, recent stress did not have a direct effect on suicidal ideation in either group. Previous studies reported many different ways that stress affects suicidal ideation, depending on the group involved. Although a study on Japanese college students reported that stressful life events were not directly associated with suicidal ideation, and the effect was fully mediated by depressive mood or cognitive style,42 most studies have reported that the relationship between stress and suicidal ideation is partially mediated. For example, stressful life events, stress due to schoolwork, and stress from the college environment exert an indirect influence on suicidal ideation with insomnia,72 depression,73 and depressive symptoms,43 respectively, as partial mediators. A study on Korean college students presented a similar result.44 Further, characteristics of stress itself affect suicidal ideation in various ways. Stress unrelated to interpersonal relationships does not affect suicidal ideation; in stress stemming from interpersonal relationships, only chronic stress has an indirect effect on suicidal ideation by increasing perceived burdensomeness—episodic stress does not affect suicidal ideation.74 In sum, how stress influences suicidal ideation is partly determined by characteristics of the group and characteristics of stress. For instance, according to a Korean study on individuals receiving health screening and examination (a non-clinical sample), the male and female average score of the SQ for KNHANES-SF is 16.01 (SD = 5.92) and 18.01 (SD = 7.08), respectively.75 Considering the average score for suicidal non-victims and victims of ET (Table 2), our participants appeared to experience a higher level of stress than the non-clinical health examination group (although a formal difference analysis was not performed). Our findings that the effect of recent stress on suicidal ideation is fully mediated by either depressive symptoms or anxiety symptoms is the consequence of the combined influences of characteristics specific to the study sample—people with suicidality—and to the stress—a considerably high degree of recent stress during the recent month.
In addition to the limitations mentioned previously, this study has other limitations. First, because it was cross-sectional, reverse causality cannot be excluded. Second, the retrospective study design may have introduced forgetfulness bias.76 Third, all the participants were Korean women, and thus generalization to other ethnicities or genders should be performed with caution. Fourth, the time frames of the measurement tools used in this study were not the same (the recent one month for the SQ for KNHANES-SF and the C-SSRS and the last two weeks for the PHQ-9 and the BAI). Despite the limitations, this study has several strengths that warrant more detailed comment. This is the first study to comprehensively investigate the contribution of variables well-established as risk factors of suicidal ideation according to the presence or an absence of a history of ET. Further, by using clinical and non-clinical samples together, we minimized selection bias.
In conclusion, we showed that recent stress can contribute to suicidal ideation by increasing the level of anxiety symptoms for victims of ET and depressive symptoms for non-victims of ET as full mediators. The clinical implications of this study for treating patients with suicidality are two-fold. To effectively reduce such patients' suicidal ideation, it will be helpful to choose prioritized target psychopathology for tailored intervention according to the presence or absence of a history of ET. Further, aiming to decrease anxiety symptoms for women with a history of ET, and depressive symptoms for other women, is essential. Clinicians should go beyond educating those patients in simple stress-management techniques, taking into consideration that stress does not exert a direct influence on their suicidal ideation. Further studies are required to examine the effects of reducing anxiety and depressive symptoms on suicidal ideation in people with and without a history of ET.
Go to :
 XML Download
XML Download