

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Patients with rheumatoid arthritis (RA) are more susceptible to infection than other people.1 Patients treated with biologic disease-modifying antirheumatic drugs (bDMARDs), especially tumor necrosis factor (TNF) inhibitors, are at increased risk of developing tuberculosis (TB), predominantly via reactivation of latent tuberculosis infection (LTBI).2 LTBI is now recognized as an incipient phase of TB with a potential risk of progressing to active infection; consequently, it is seen as requiring treatment for greatest benefit.3 Accordingly, screening for LTBI is required to prevent TB infection in RA patients undergoing bDMARDs treatment.4
There are two widely used methods for diagnosing LTBI: the tuberculin skin test (TST) and the interferon gamma release assay (IGRA). The TST has long been used in LTBI diagnosis, and while it is very cost effective, it requires two clinic visits to get results. Also, false positivity caused by Bacillus Calmette–Guérin (BCG) vaccination and nontuberculous mycobacteria (NTM) infection and false negativity in immunosuppressed patients are drawbacks.5 On the other hand, the IGRA has relatively high specificity and is not affected by BCG vaccination status.6 Thus, it is more useful in countries with a high rate of BCG vaccination such as Korea though it is more expensive than the TST and requires a well-equipped laboratory and skilled technicians.7
The World Health Organization (WHO) published updated guidelines for LTBI management in 2018, recommending the TST and IGRA equally for LTBI diagnosis.8 In the Korean guidelines, the TST alone, IGRA alone, or a two-step TST/IGRA protocol are recommended for diagnosing LTBI in immunocompetent people.9 However, in immunocompromised patients, TST alone is not recommended; rather, IGRA alone or the two-step TST/IGRA is recommended.9 According to the 2017 Korean guidelines for TB, immunocompromised patients who are recommended to undergo LTBI treatment include patients with human immunodeficiency virus (HIV) and those who are initiating or using immunosuppressive drugs and TNF inhibitors.9 Apart from TNF inhibitors, bDMARDs are not discussed in the Korean guidelines; however, the American College of Rheumatology (ACR) recommends screening all RA patients for LTBI if they are being considered for receiving bDMARDs or tofacitinib10; in addition, IGRA test is recommended for patients with a history of BCG vaccination rather than TST.10
Tofacitinib is the first oral Janus kinase (JAK) inhibitor to be released. Studies have suggested that its administration leads to increased TB reactivation.1112 Thus, as with TNF inhibitor, LTBI screening and treatment are recommended prior to starting tofacitinib.1112 However, there is a lack of information about how LTBI screening and treatment affect the positivity rate and incidence of active TB in patients about to start tofacitinib treatment compared with patients about to start TNF inhibitors or other bDMARDs.
In this study, we examined whether the diagnosis and treatment of latent TB in RA patients are effective in Korea. We also estimated the risk of TB development by calculating the incidence rate of active TB among RA patients receiving targeted therapy.
METHODS
Data extraction and study population
We analyzed data from two prospective cohort studies. Data were extracted from two registries of patients receiving bDMARDs and JAK inhibitors, respectively, at a single academic referral hospital in Seoul, Korea. Patients with RA who started bDMARDs between July 2011 and May 2019 and those who started JAK inhibitors between March 2017 and August 2019 were included in this study. New starters for each targeted therapy were selected after exclusion of patients who had previously received any bDMARD or JAK inhibitor treatment before. Hence, all participants were bDMARD-naïve and JAK inhibitor-naïve RA patients. We divided the patients into three groups: those receiving TNF inhibitor, non-TNF inhibitor, and JAK inhibitor.
Positivity of LTBI screening tests and treatment
Three kinds of tests were used for LTBI screening: the TST and two different IGRAs: the QuantiFERON-TB Gold In-Tube (QFT-GIT; Cellestis, Carnegie, Victoria, Australia) and the T-SPOT.TB test (Oxford Immunotec, Abingdon, United Kingdom). A positive TST was defined as an induration ≥10 mm after 48–72 hours regardless of BCG vaccination in accord with the Korean National Guidelines913 because the effect of BCG vaccination on TST results is controversial.1415 We compared the rates of LTBI screening, and LTBI prevalences for each group: TNF inhibitor, non-TNF inhibitor, and JAK inhibitor, and calculated the LTBI positivity rates from the individual test results. We also used the combination of two tests to develop a composite rule for patients with discordant test results: patients who were positive on either TST or IGRA were classified as LTBI positive and patients with two negative test results were classified as LTBI negative. Patients whose IGRA result was indeterminate were classified as indeterminate if their TST result was negative. We also investigated whether the LTBI was treated and which treatment was used.
The active TB incidence rate during first-line targeted therapy
The active TB incidence rate during first-line targeted therapy was calculated for each treatment group. The observation period included the time until the patient stopped treatment, switched to another bDMARD or JAK inhibitor, or active TB was diagnosed. When none of these occurred, observations were terminated in May 2019 for bDMARDs and August 2019 for JAK inhibitors. The clinical characteristics of patients who developed TB were examined in detail. We reviewed previous studies of LTBI prevalence and TB incidence in RA patients using bDMARDs in Korea, and compared their findings with our study findings.
Statistical analyses
Categorical variables are presented as frequencies and percentages, and continuous variables are presented as means with standard deviations or medians with interquartile ranges. The χ2 test or Fisher's exact test was performed to assess the significance of differences in categorical variables, and the Kruskal-Wallis test was performed for continuous variables. The Bonferroni correction was used for multiple comparisons between the three groups for categorical variables, and the Dwass-Steel-Critchlow-Fligner test for continuous variables. After evaluating the positivity of each LTBI test and the two-test combinations, we used Cohen's kappa to assess agreement between the TST and IGRA in patients who received both tests. We calculated crude TB incidence rates during the observation period and active TB incidence rates were calculated per 100,000 person-years (PYs) with 95% confidence intervals (CIs). All analyses were performed using SAS 9.4 (SAS Institute, Cary, NC, USA). P values < 0.05 were considered statistically significant.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of the Hanyang University Hospital (IRB No. HYUH 2020-08-051). We used the existing prospective cohort data for patients using bDMARDs (IRB No. HYUH 2011-05-008-029) or JAK inhibitor (IRB No. HYUH 2016-08-037-001), and informed consent was obtained from all patients enrolled in each registry. The information on the subjects could not be identified directly or through identifiers linked to the subjects.
RESULTS
Baseline characteristics of the study population
A total of 765 RA patients who started their first bDMARD or JAK inhibitor treatment (TNF inhibitors: n = 574, non-TNF inhibitors: n = 132, and JAK inhibitor: n = 59) were included in this study (Fig. 1). Baseline characteristics are described in Table 1. The mean age of the study population at the start of treatment was 51.8 (± 13.2) years, and 85.9% of the patients were female. Duration of RA was significantly longer in the JAK inhibitor group (12.0 [4.0–19.0] years) than in the TNF inhibitor group (5.0 [1.0–11.0] years; P < 0.001) or the non-TNF inhibitor group (3.0 [1.0–10.0] years; P < 0.001).
Fig. 1
Flow diagram of patient selection.
RA = rheumatoid arthritis, bDMARDs = biologic disease-modifying antirheumatic drugs, TNF = tumor necrosis factor, JAK = Janus kinase.
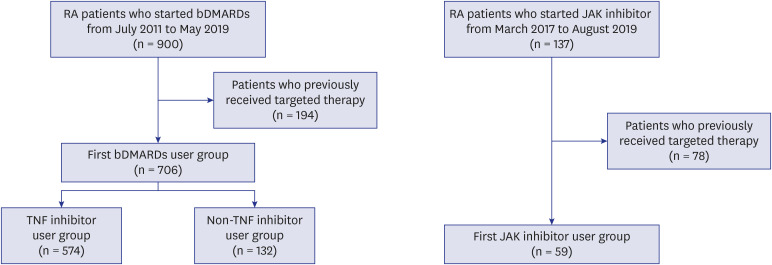
Table 1
Baseline characteristics of the RA patients according to targeted therapy
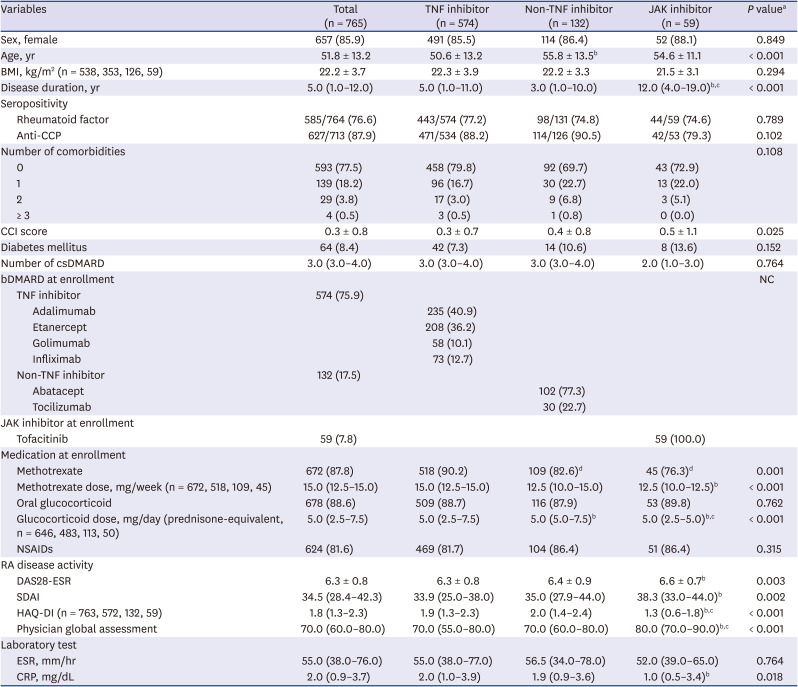
Values are presented as means ± standard deviations, medians (interquartile ranges) or numbers (%).
NC = not calculated, RA = rheumatoid arthritis, TNF = tumor necrosis factor, JAK = Janus kinase, BMI = body-mass index, Anti-CCP = anti-cyclic citrullinated peptide, CCI = Charlson comorbidity index, csDMARDs = conventional synthetic disease-modifying antirheumatic drugs, bDMARDs = biologic DMARDs, NSAIDs = nonsteroidal anti-inflammatory drugs, DAS = disease activity score, ESR = erythrocyte sedimentation rate, SDAI = simple disease activity index, HAQ-DI = health assessment questionnaire-disability index, CRP = C-reactive protein.
aComparison among three groups: the χ2 test or Fisher's exact test for categorical variables and Kruskal-Wallis test for continuous variables; bSignificantly different compared with TNF inhibitor group by the Dwass-Steel-Critchlow-Fligner test as a post-hoc comparison; cSignificantly different compared with non-TNF inhibitor group by the Dwass-Steel-Critchlow-Fligner test as a post-hoc comparison; dSignificantly different compared with TNF inhibitor group as a post-hoc comparison after χ2 test (Bonferroni correction).
In the TNF inhibitor group, adalimumab (40.9%) was the most common treatment followed by etanercept (36.2%), infliximab (12.7%), and golimumab (10.1%). In the non-TNF inhibitor group, abatacept (77.3%) was administered as a first-line therapy more frequently than tocilizumab (22.7%). All patients in the JAK inhibitor group received tofacitinib (100.0%).
RA disease activity was higher in the JAK inhibitor group than the TNF inhibitor group, as measured by the Disease Activity Score 28 with ESR (DAS28-ESR) (P = 0.003), and the Simple Disease Activity Index (SDAI) (P = 0.002). However, the Health Assessment Questionnaire-Disability Index (HAQ-DI) was lower in the JAK inhibitor group than the others (P < 0.001). Visual analogue scale scores by physician's global assessment were higher in the JAK inhibitor group than the TNF inhibitor group (P < 0.001) or the non-TNF inhibitor group (P = 0.001) with significant differences.
Performance of LTBI screening tests
All 765 patients underwent at least one LTBI screening test. The QFT-GIT test was the most commonly used method of screening. Of the 765 patients, 758 (99.1%) had the IGRA test and 423 (59.9%) had the TST. The numbers of IGRA alone, TST alone, and the TST/IGRA two-step test are given in Table 2. There were 342 patients who received the QFT-GIT test only, 7 patients who received TST only, and 416 patients who received both. Only one patient received the T-SPOT.TB test, and this patient also received the QFT-GIT test in combination with the TST. The IGRA alone has most often been used for LTBI screening since 2017, so the JAK inhibitor group did not receive the TST.
Table 2
Rates of execution and positivity of LTBI screening tests, and rates of treatment in RA patients according to targeted therapy
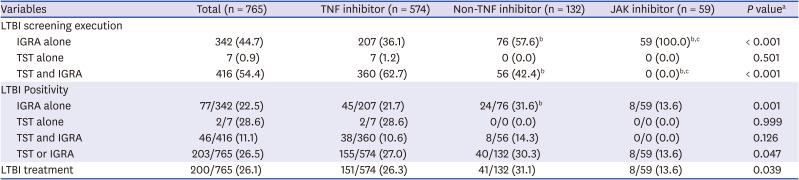
Values are presented as numbers (%).
LTBI = latent tuberculosis infection, RA = rheumatoid arthritis, TNF = tumor necrosis factor, JAK = Janus kinase, IGRA = interferon gamma release assay, TST = tuberculin skin test.
aComparison among three groups: the χ2 test or Fisher's exact test; bSignificantly different compared with TNF inhibitor group as a post-hoc comparison after χ2 test (Bonferroni correction); cSignificantly different compared with non-TNF inhibitor group as a post-hoc comparison after χ2 test (Bonferroni correction).
Positivity for LTBI tests among all the patients based on at least one test was 26.5% (203/765). Positivity rates for the individual LTBI tests were 21.8% (165/758) for QFT-GIT and 19.9% (84/423) for TST. Positivity for IGRA in patients who received only IGRA was 21.7% in the TNF inhibitor group, 31.6% in the non-TNF inhibitor group, and 13.6% in the JAK inhibitor group.
The IGRA results were indeterminate in 18 of the 416 patients who received both TST and IGRA. After excluding those 18 patients, we assessed the agreement between TST and IGRA and found moderate agreement (Cohen's κ = 0.432, Table 3). Of the RA patients with positive IGRA results, 52.3% (46/88) were positive for the TST. In contrast, only 10.6% (33/310) of those with negative IGRA results were positive on TST.

LTBI treatment for RA patients initiating targeted therapy
A total of 189 patients (93.1%) of the 203 patients who tested positive on LTBI screening test received LTBI treatment. Of the 14 patients who did not receive treatment despite their positive LTBI tests, 5 had a history of active TB and completion of anti-TB medication, and 5 patients tested positive on the TST and negative on the IGRA. The other 4 patients tested positive on IGRA alone but did not receive any LTBI treatment; no reason was recorded.
In contrast, 7 patients who were negative for LTBI screening received treatment; 3 patients presented with TB scarring on chest radiography but did not have a definite history of active TB; 3 patients had a previous positive IGRA, and 1 patient had an induration of 9 mm on the TST.
All patients receiving LTBI treatment were given isoniazid (INH) except one who received rifampin after developing urticaria on INH. In accordance with the guidelines, INH was used for 9 months and rifampin for 4 months.9
Risk of TB development during first targeted therapy
During the 1,573.2 PYs of follow-up, only one patient in the TNF inhibitor group developed active TB (1,255.2 PYs); none developed active TB in the non-TNF inhibitor (264.7 PYs) and JAK inhibitor (53.3 PYs) groups. The incidence rate was 63.6 per 100,000 PYs (95% CI, 3.2–313.5). The patient who developed TB was diagnosed with pulmonary TB after 7 months of adalimumab use. She did not receive LTBI treatment because her IGRA result was negative, though her induration result for TST was 10 mm.
DISCUSSION
In this study, we estimated that 26.5% of RA patients initiating bDMARD or JAK inhibitor treatment had LTBI. There was no significant difference in LTBI prevalence among the RA patients starting TNF inhibitors, non-TNF inhibitors, or JAK inhibitors. Most patients were appropriately treated according to the guidelines, and LTBI treatment was mainly with INH. Consequently, the active TB incidence rate during the first targeted therapy was low (63.6/100,000 PYs).
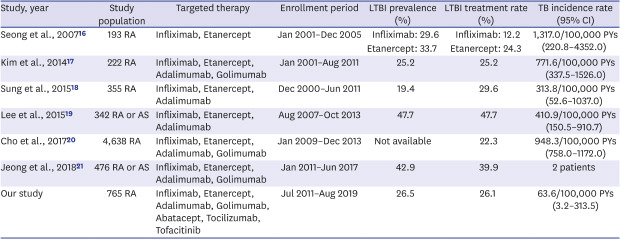
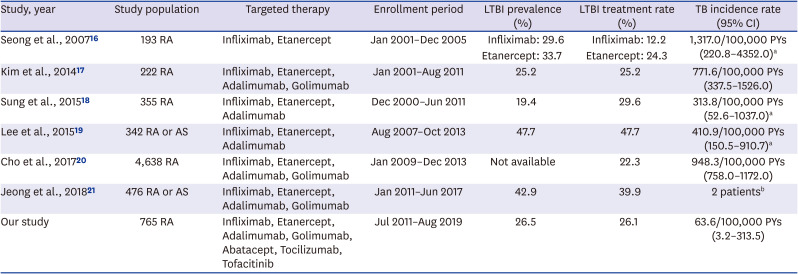
There have been 6 previous studies of LTBI prevalence and TB incidence in RA patients using bDMARDs in Korea,161718192021 and we conducted a literature review of those studies (Table 4). LTBI prevalence in RA patients ranged from 19.4% to 47.7% in those studies, compared with our 26.5% prevalence among all patients. TB incidence rates in previous studies (313.8–1,317.0 per 100,000 PYs) were higher than in our study in point estimates (63.6 per 100,000 PYs). It is possible that this low incidence, even with the relatively large numbers of patients, was because the study population was limited to first users of targeted therapy or because our institution screened and treated LTBI rigorously in accordance with clinical practice guidelines. It is important to note that the TB incidence rate has not increased recently, even though only IGRA has been used since the Korean guidelines for TB were released in 2017.
Table 4
Literature review on LTBI prevalence and TB incidence in patients with RA receiving targeted therapy in Korea
| Study, year | Study population | Targeted therapy | Enrollment period | LTBI prevalence (%) | LTBI treatment rate (%) | TB incidence rate (95% CI) |
|---|---|---|---|---|---|---|
| Seong et al., 200716 | 193 RA | Infliximab, Etanercept | Jan 2001–Dec 2005 | Infliximab: 29.6 | Infliximab: 12.2 | 1,317.0/100,000 PYs (220.8–4352.0)a |
| Etanercept: 33.7 | Etanercept: 24.3 | |||||
| Kim et al., 201417 | 222 RA | Infliximab, Etanercept, Adalimumab, Golimumab | Jan 2001–Aug 2011 | 25.2 | 25.2 | 771.6/100,000 PYs (337.5–1526.0) |
| Sung et al., 201518 | 355 RA | Infliximab, Etanercept, Adalimumab | Dec 2000–Jun 2011 | 19.4 | 29.6 | 313.8/100,000 PYs (52.6–1037.0)a |
| Lee et al., 201519 | 342 RA or AS | Infliximab, Etanercept, Adalimumab | Aug 2007–Oct 2013 | 47.7 | 47.7 | 410.9/100,000 PYs (150.5–910.7)a |
| Cho et al., 201720 | 4,638 RA | Infliximab, Etanercept, Adalimumab, Golimumab | Jan 2009–Dec 2013 | Not available | 22.3 | 948.3/100,000 PYs (758.0–1172.0) |
| Jeong et al., 201821 | 476 RA or AS | Infliximab, Etanercept, Adalimumab, Golimumab | Jan 2011–Jun 2017 | 42.9 | 39.9 | 2 patientsb |
| Our study | 765 RA | Infliximab, Etanercept, Adalimumab, Golimumab, Abatacept, Tocilizumab, Tofacitinib | Jul 2011–Aug 2019 | 26.5 | 26.1 | 63.6/100,000 PYs (3.2–313.5) |
LTBI = latent tuberculosis infection, TB = tuberculosis, RA = rheumatoid arthritis, CI = confidence interval, AS = ankylosing spondylitis.
aSource: Own calculation. Open source statistics for public health was used (https://www.openepi.com/PersonTime1/PersonTime1.htm); bObservation period was not available.
There was one case of active TB development in the TNF inhibitor group; this can be explained in two ways.
First, using a TNF inhibitor might create a higher risk of TB activation than using a non-TNF inhibitor or a JAK inhibitor, because there were no instances of active TB development in the latter groups. TNF inhibitors are known to facilitate LTBI progression to active TB by inhibiting phagosome maturation and inducing T-cell apoptosis, complement-dependent cytotoxicity, and antibody-dependent cell-mediated cytotoxicity, all increasing susceptibility to TB reactivation.22 On the other hand, it is not yet clear how JAK inhibitors increase the incidence of TB or other infections.23 However, non-TNF inhibitors or JAK inhibitors cannot be considered safer than TNF inhibitors based on our study because of the differences in LTBI positivity and follow-up duration between the groups. The positivity rates for IGRA test on its own were 21.7% (TNF inhibitor group), 31.6% (non-TNF inhibitor group), and 13.6% (JAK inhibitor group), indicating that RA patients who had been IGRA positive were more likely to have been treated with non-TNF inhibitors and least likely to have been treated with JAK inhibitors. Moreover, the follow-up duration for JAK inhibitor use was only 53.3 PYs, while that for bDMARDs was 1,519.9 PYs. Therefore, further long-term study of treatment safety is required to elucidate the risk of active TB development in JAK inhibitor users.
Second, the diagnostic performance of each LTBI screening test should be considered. One patient who developed active TB was negative on the IGRA and equivocal on the TST with an induration of 10 mm. This raises the question of whether it is appropriate to not treat LTBI in patients who are shown to be negative by IGRA alone. According to the current Korean guidelines for TB published in 2017, patients initiating TNF inhibitors can be diagnosed with LTBI by the TST/IGRA two-step test or IGRA alone, which is the same as for immunocompromised patients.9 As many studies continue to confirm the efficiency of the IGRA, an increasing number of patients undergo IGRA alone for LTBI screening.1619 Although the agreement between TST and IGRA results is moderate or low,24252627 LTBI screening based on IGRA can sufficiently lower TB incidence, as this study demonstrates. Further research is needed regarding screening for LTBI with the TST/IGRA two-step test versus IGRA alone. There should also be renewed debate regarding the need to repeat LTBI screening to identify newly developed TB infection in patients using TNF inhibitors, non-TNF inhibitors, and JAK inhibitors for long durations.28
Of the 197 patients who received LTBI treatment, 196 received INH monotherapy. INH is a major drug in LTBI treatment, but the long regimen duration (6–9 months) reduces compliance.2930 Although INH treatment is associated with liver-function test abnormalities, our previous work showed that it does not lead to discontinuation of bDMARDs.31 In the present study, none of the patients who received INH monotherapy developed active TB. This means that INH monotherapy is effective as an LTBI treatment, but further research is needed on the long-term effects in patients receiving targeted therapy, especially patients who received sequential treatment with bDMARDs and JAK inhibitors.
Our study has several limitations. First, the observation period was limited to the period when the first bDMARD or JAK inhibitor was used. A short observation period, especially for JAK inhibitors, might have resulted in measuring a low active TB incidence. However, in previous studies, the median times between TB infection and treatment with bDMARDs and JAK inhibitors in RA patients were 7.9 months (95% CI, 4.0–36.1) and 64 weeks (range, 15–161), respectively.1129 Thus, the results from this study are still valuable. The safety of JAK inhibitors should be evaluated in a future study where long-term data are collected. Second, patients often receive more than one bDMARD or JAK inhibitor, but that was not reflected in this study. Further research is needed on how sequential treatment with bDMARDs and JAK inhibitors and continuous exposure to these substance affects TB activation. Third, it is difficult to generalize from our results because data were collected from a single institution, which may have introduced a selection bias that influenced active TB incidence.
In conclusion, TB incidence in RA patients receiving TNF inhibitor, non-TNF inhibitor, or JAK inhibitor treatment was low. LTBI screening and treatment with INH according to the Korean guidelines are appropriate. However, further study is needed to evaluate the efficacy of IGRA on its own for screening LTBI, and to evaluate the long-term risk of TB development in patients who use JAK inhibitors.
 XML Download
XML Download