

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Osteonecrosis of the femoral head (ONFH) is a condition in which part of the femoral head becomes necrotic associated with a disruption of the blood supply.1 The necrosis usually involves the weight-bearing dome of the femoral head. As the disease progresses, mechanical strength of the necrotic bone is reduced, leading to eventual collapse. This subsequently leads to secondary arthritis of the hip. One common cause of ONFH is trauma. A displaced femoral neck fracture or hip dislocation can injure the local blood vessels and lead to bone death. Non-traumatic risk factors for ONFH include the use of corticosteroids, excessive alcohol intake, excessive tobacco use, sickle cell disease, systemic lupus erythematosus, organ transplantation, human immunodeficiency virus infection, coagulopathies, a number of genetic factors, Caisson disease (deep-sea divers), myeloproliferative diseases (marrow packing diseases), and radiation necrosis.234
Non-traumatic ONFH usually affects adults younger than 50 years and frequently progresses to collapse of the femoral head. In the United States, about 10,000 new patients are estimated to be affected with the disease annually.5 The annual incidence rate in Japan was 1.91/100,000 and the annual incidence was estimated to be more than 2,400 in 2015.6 In South Korea, the estimated prevalence of ONFH increased from 9,870 in 2002 to 18,691 in 2006.7 In a recent large-scale epidemiological survey in China, the cumulative number of patients with non-traumatic ONFH reached 8.12 million among the Chinese population.8
There has been considerable progress made on our comprehension concerning the pathogenesis of the non-traumatic ONFH during the last 3 decades. However, most studies report fragmentary knowledge and an integrated explanation of the pathogenesis has not been established.9 Thus, the Association Research Circulation Osseous (ARCO) task force members have systematically reviewed the up-to-date knowledge with this report representing a consensus on the pathogenesis of ONFH.
ARCO TASK FORCE AND PREPARATION OF THE MANUSCRIPT
In April 2020, the ARCO task force was established including 4 members: 3 orthopedic surgeons and 1 rheumatologist. They thoroughly searched PubMed and reviewed of relevant articles about the pathogenesis of non-traumatic osteonecrosis of the femoral head. The search was done using the key search terms “osteonecrosis,” “avascular necrosis,” “aseptic necrosis,” “pathology,” and “pathogenesis” for entries from January 1, 1970 to March 31, 2020. After then, the task force prepared the first draft and circulated it to 14 ARCO members. The manuscript was repeatedly revised until all participants agreed and it was finalized in September 2020.
HISTOLOGIC CRITERIA OF ONFH
Arlet and Durroux described ONFH as a progressive disease involving the marrow space first, followed by the trabecular bone later. They classified necrotic lesions into 4 types10: Type 1 lesions show loss of hematopoietic cells in the marrow and fatty marrow conversion; Type 2 lesions demonstrate necrosis of the marrow; Type 3 lesions exhibit necrosis of the marrow and bone (death of osteocytes > 50%); and Type 4 lesions demonstrate necrosis of the marrow and bone with encapsulating fibrovascular tissue, which changes to sclerotic bone later by apposition of new bone. Type 2 lesions are non-specific for ONFH as they are seen in other pathologies including transient bone marrow edema syndrome (BMES),1112 the uninvolved femoral heads of patients who have unilateral ONFH,13 and the femoral heads of patients who are treated with corticosteroids.14151617 The presence of type 4 lesion is generally accepted as a histologic criterion to make a diagnosis of ONFH.161819
CURRENT CONCEPTS CONCERNING THE PATHOGENESIS OF ONFH
Currently, three theories are generally accepted in terms of the pathogenesis of ONFH. The first theory considers both the bone and intravascular mechanisms as the cause.2162021 The second theory considers only intravascular coagulation as the pathway to ischemia.2162021 The third theory promotes ONFH as having a multifactorial etiology.12345 In most cases, ONFH is associated with multiple factors including genetic predispositions as well as the exposure to risk factors. Any of the risk factors can play a role in the development of ONFH and contribute to its pathogenesis in most cases.2223242526272829 The hereditary predisposition explain why only some of the high-dose corticosteroids users and alcohol abusers acquire the disease, while others do not. Indeed, an ischemic event does not always lead to ONFH. The progression is generally dependent on the restoration of vascular perfusion and the creeping substitution of dead bone by new bone.2162021
In 1949, Chandler termed ONFH (then called avascular necrosis) as “coronary disease of the hip” because he thought that the cause was an abrupt vascular obstruction by thrombosis or embolism.30 However, unlike the coronary artery, the lateral epiphyseal vessels are housed within the closed chamber of the femoral head, which is filled with marrow cells. Therefore, femoral head osteonecrosis should be considered as a compartment syndrome of the femoral head due to intra-osseous hypertension rather than as a vascular obstructive disease, although this is debatable.10
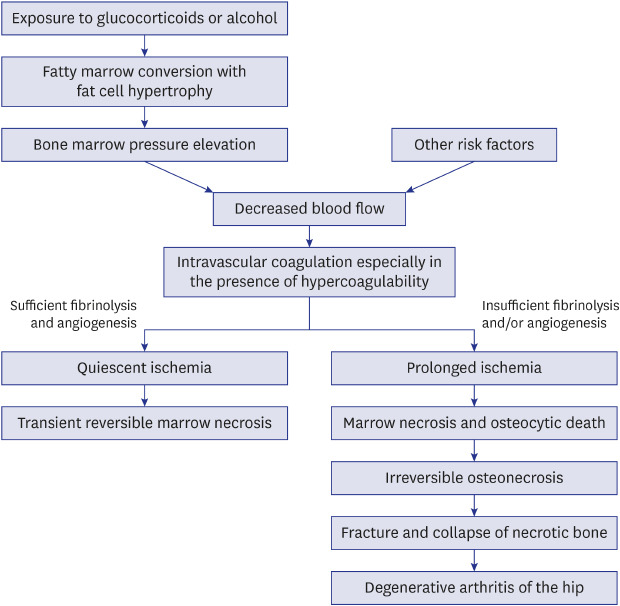
There are sufficient data to support such a pathophysiologic cascade: fat cell hyperplasia; intra-osseous hypertension; vascular compression and thrombosis; ischemia; marrow and bone necrosis; subchondral fracture; and collapse of the femoral head, particularly in corticosteroid - and alcohol- associated ONFH, while other risk factors may work through different mechanisms. This leads to subsequent secondary arthritis of the hip; the end-stage of ONFH (Fig. 1).1619
Fat cell hypertrophy in the marrow space and intra-osseous hypertension
Corticosteroids promote differentiation of pre-adipocytes and mesenchymal stem cells to mature adipocytes by stimulating the peroxisome proliferator-activated receptor-gamma (PPAR-γ) and suppressing run-related transcription factor 2 (RUNX2).313233343536 In addition, corticosteroids and alcohol induce adipocyte hypertrophy through increasing lipid synthesis of the marrow fat cell.313233343536
Several polymorphisms in genes involved in corticosteroid metabolism (adenosine triphosphate binding cassette B1, ABCB1) or in lipid metabolism (apolipoprotein B, ApoB) are associated with ONFH.3738
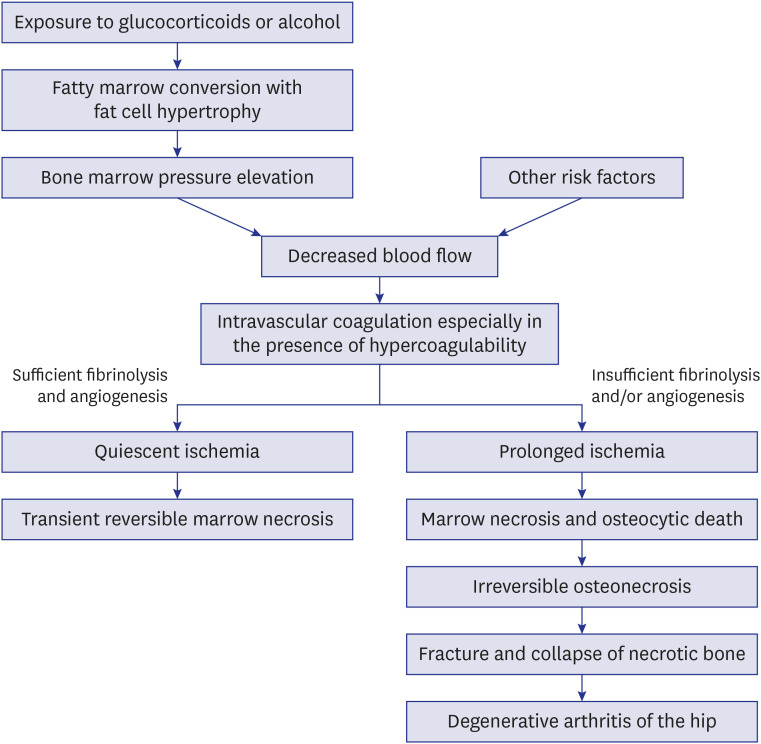
Hematopoietic cells are depleted and the marrow space is filled with large (> 10 µm) round to ovoid fat cells (Arlet and Durroux Type 1 lesion) (Fig. 2).333435
Fig. 2
The marrow space is filled with hypertrophied fat cells. However, osteocytes are seen in lacunae (Arlet and Durroux Type 1 lesion) (hematoxylin and eosin stain, original magnification ×200).
Due to the fatty marrow conversion, the proximal femoral metaphysis shows a high signal intensity on T1-weighted magnetic resonance images (MRIs).39 The increment of marrow fat cell volume and/or an increase in the number of fat cells induce intra-osseous hypertension in the proximal femur. The intra-osseous hypertension compresses venous sinusoids, leads to intravenous microvascular coagulation and subsequent impairment of blood flow to the femoral head.39404142
Marrow necrosis
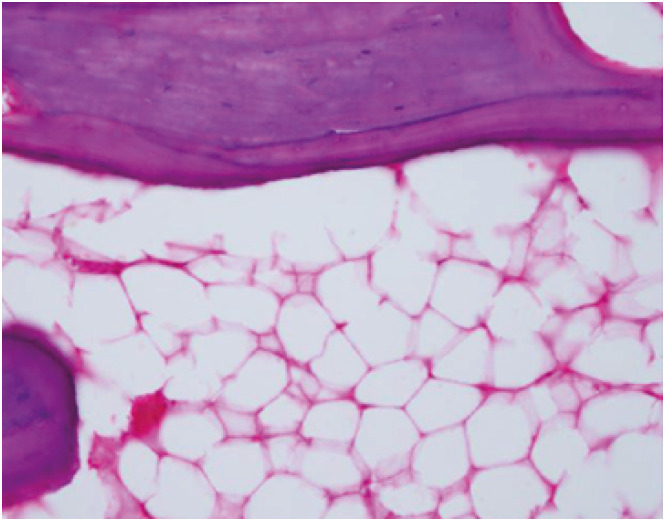
Intravascular coagulation leads to acute ischemia in the marrow of the femoral head. Normal marrow cavities are predominantly filled with two types of cells; bone marrow fat cells and hematopoietic cells. The marrow fat cell accounts for approximately 70% of the adult bone marrow volume. The number of hematopoietic cells gradually decreases with age. Each marrow cell has different tolerability for ischemia.43444546 The hematopoietic cells are sensitive to the ischemia and most of them will die within 12 hours after the ischemic event.46 The marrow fat cells subsequently die and their nuclei disappear within 48 hours of a complete ischemia. Thus, the initial microscopic signs of bone ischemia appear in the marrow space. The hematopoietic cells disappear and then the fat cells become necrotic (Arlet and Durroux Type 2 lesion) (Fig. 3).
Thrombophilia/hypofibrinolysis and impaired angiogenesis
Intravascular coagulation that occurs within the femoral head triggers fibrinolysis. The fibrinolytic system is built upon active enzymes, proplasmin, and a serine protease that degrades fibrin clots. Various genetic and hereditary conditions, which cause increased thrombosis and/or decreased fibrinolysis, accentuate and/or prolong the intravascular coagulation.
Several coagulopathies have been implicated in causing this intravascular coagulation. Protein C has an anticoagulant capacity by corrupting procoagulant factors Va and VIIIa. Protein S serves as cofactor for triggered protein C.41 Proteins C and S deficiencies,4748495051 as well as mutations in the factor V Leiden or the prothrombin 20210A gene,51 increase thrombosis.
Polymorphisms of the plasminogen activator inhibitor-1 gene (PAI-1) are associated with a hypercoagulable state.495253 Antiphospholipid antibodies,5455 inflammatory bowel disease,5657 and sickle cell disease5859 also increase the risk of microvascular thrombi. Moreover, a recent genome-wide association study from Japan identified long intergenic non-protein coding RNA 1370 (LINC01370) as a candidate risk gene in Japanese patients who have idiopathic ONFH, and stratified their analysis by risk factors suggested that the 12q24 locus was associated with the disease through drinking capacity.60
This intravascular coagulation leads to local hypoxia, nutrient deficiency, and marrow necrosis, which ultimately activates angiogenesis. Compromised angiogenesis has been considered as a contributing factor for the development of ONFH. Nitric oxide, a known vasodilator, advances angiogenesis and bone formation. Polymorphism in the endothelial nitric oxide synthase (eNOS) gene has been related to ONFH in patients who have no acquired risk factors.2429 Vascular endothelial growth factor (VEGF), which is prompted by hypoxia, is a known angiogenic protein that also promotes cartilage and bone regeneration. Genetic polymorphisms of VEGF are related to the progression of corticosteroid-associated ONFH.2628 Corticosteroids also inhibit angiogenesis by suppressing the production of VEGF.61
If complete fibrinolysis and adequate angiogenesis occur within the critical ischemic period, the duration of ischemia can be brisk and the blood perfusion can be restored. Although the marrow space remains fatty, the lesion is reversible and does not progress to definite osteonecrosis.16 Most osteocytes (> 50%) remain viable (Arlet and Durroux type 2 or 3 lesion). The ischemia does not produce a sequestrum and there is no fibrovascular reparative zone around the necrotic marrow. The reactive band, which is the earliest diagnostic magnetic resonance (MR) finding for ONFH,62 is not seen. The only nonspecific MR finding is an increase in signal intensity of the proximal femoral metaphysis on T1-weighted images, which indicates an increase of fat substance in the marrow space.
Osteocytic death and formation of a sequestrum
In the presence of thrombophilia/hypofibrinolysis and/or impaired angiogenesis, prolonged damage due to ischemia occurs and definite ONFH develops.
Reparative process at the margin of the sequestrum
Necrotic bone, when recognized as a foreign body by the host's immune system, induces an immune reaction. The histocompatibility antigens of dead bone are the glycoproteins on cell surfaces. These matrix proteins may or may not elicit a foreign body reaction. The host response to dead bone depends on the concentration and total dose of the antigen of the dead bone.26 Necrotic bone is a composite material, which has many antigens of glycoproteins and potentially could elicit varying immune responses. Hydroxyapatite in the trabeculae elicits a minimal immune response. Extracellular composites such as type I collagen and non-collagenous matrix proteins (i.e., proteoglycans, osteocalcin), induce a mild immune reaction. However, byproducts from dead bone marrow cells can elicit a more marked immune response.61 The necrotic bone is encapsulated by a fibrous membrane, defined histologically as a reactive zone. On MRIs, this appears as a band of low-signal intensity. A definite diagnosis of ONFH is made at this stage, which is characterized by the formation of a focal sequestrum surrounded by a fibrous membrane.1319
Marrow edema can be associated with the viable portion around the sequestrum. The edema increases the bone marrow pressure, which may lead to symptomatic pain in the patient's hip.66 Capillaries infiltrate into the fibrotic capsule. However, this angiogenesis is stopped at the margin of the sequestrum. The reparative fibrovascular tissue cannot penetrate into the dead marrow space of the sequestrum and little to no biological repair occurs in the necrotic portion of the femoral head.67 The fibrotic capsule is progressively ossified and appears as a sclerotic rim on radiographs. Bone turnover in this step is also affected by some genetic predisposition such as matrix metalloproteinases, osteoprotegerin (OPG), and receptor activator of NF-κB ligand (RANKL).686970
Saponification of necrotic bone and subsequent fracture
There is no biological reaction in the necrotic portion due to the absence of blood supply. However, dead marrow undergoes a chemical change, initiated by dead adipocytes releasing fatty acids.71 These fatty acids saponify with extracellular calcium to form insoluble soaps.7273 Saponified marrow shows up as a Mitchell class D lesion with a dark signal on MRIs.74
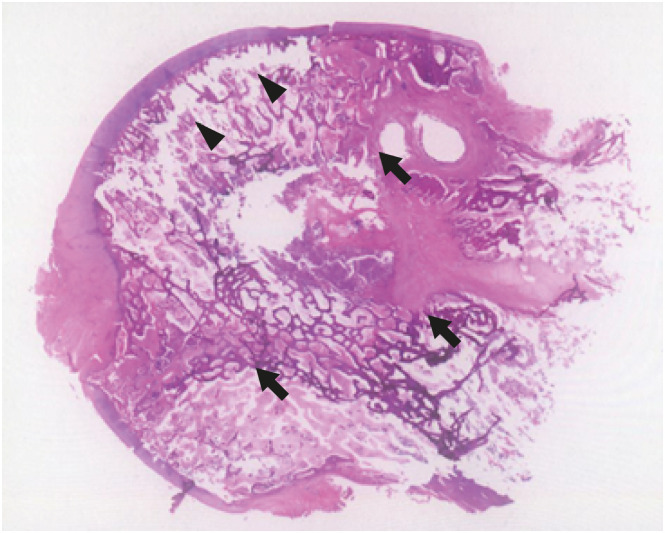
The dead trabeculae and saponified marrow do not achieve the same mechanical strength and structural integrity of previously healthy bone. Fatigue fractures occur at the subchondral portion of the joint due to this loss of structural integrity. These fractures appear on radiographs as the “crescent” sign. Fractures also form at the necrotic margin inside the ossified reactive region. The subchondral fracture leads to collapse of the femoral head and subsequent arthritis of the hip (Fig. 5).
TRANSIENT BMES
Transient BMES is an uncommon disease of the hip, which commonly recovers spontaneously within several months.12757677787980 Its etiology and pathogenesis remain unknown. However, ischemia has been suggested as a cause of the disease as the histologic findings of BMES are similar to those seen in the marrow of the early stages of ONFH,127677 and therefore it is briefly discussed here together with ONFH.
Some pregnant women develop BMES in their third trimester7578 and an association with hypofibrinolysis was reported in familial BMES.7980 However, most BMES patients do not have risk factors for ONFH.126667727374757677
Intravascular coagulation and marrow necrosis may occur in the absence or paucity of risk factors. In BMES, the fate of the femoral head after the ischemic event is quite different from ONFH. Complete fibrinolysis and reactive vasodilatation occur.81 There is only a short period of subthreshold ischemic hypoxia, which is not severe enough to induce complete bone death. The marrow necrosis induces reactive hyperemia and increased vascular permeability leading to interstitial edema in the marrow space. Although the marrow space is necrotic, most osteocytes remain viable and most lacunae are filled with osteocytes. There is no sequestrum formation and no reactive zone around the necrotic lesion.1277
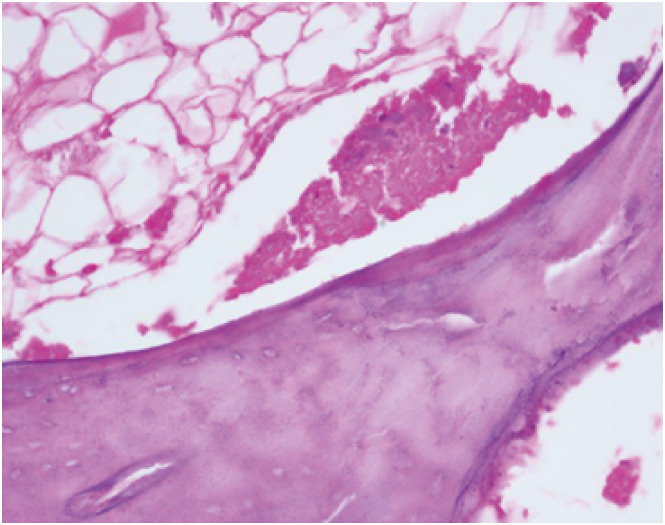
The marrow space is filled with liquid. By the Arlet and Durroux classification, these lesions are type 2 or type 3 lesions (Fig. 6). During the edema period, bone marrow pressure is raised. Most patients suffer severe hip pain and they are diagnosed at this stage. The bone marrow edema appears as a low-signal on T1 weighted MRIs and a high-signal on T2 weighted images.82
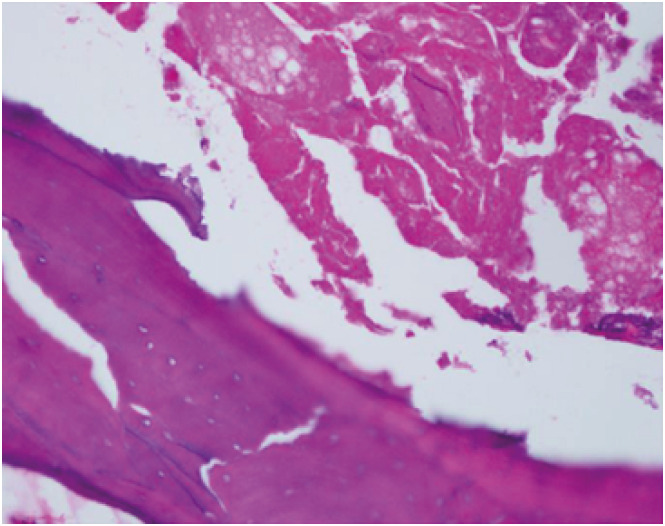
Fig. 6
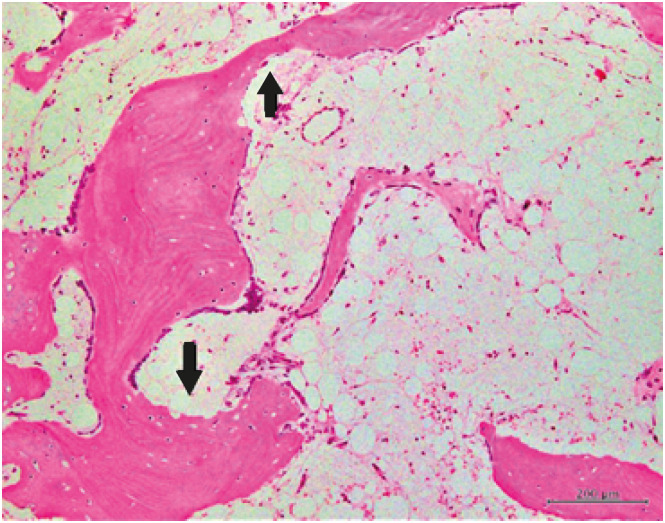
Bone trabeculae are thin and lined by osteoblasts. Focal bone resorption is seen at some areas (arrows). However, active osteoclasts are not seen and there is no creeping bone substitution. Marrow space is filled with serosanguinous materials, chronic inflammatory cells, vascular channels, and fibrosis (hematoxylin and eosin, ×100).
Angiography indicates arterial dilatation and bone scans show increased uptake in the proximal femur. The increased perfusion induces transient demineralization of the trabeculae and cortical bone of the proximal femur. When the demineralization is marked, the radiodensity of the proximal femur is diminished; this has been referred to as “transient osteoporosis of the hip”.12 However, the volume of bone mass is maintained and only the mineral content in the bone is decreased. Thus, the term “osteoporosis” is a misnomer. Wilson et al.82 proposed to use the term “transient BMES” instead of “transient osteoporosis.”
The necrotic marrow triggers creeping substitution; blood vessels begin to penetrate the necrotic marrow. Immature woven bone is deposited on the surface of trabecular bone. As the intraosseous vascularity and perfusion return to normal, the marrow edema resolves and the osteoid is mineralized. Therefore, transient BMES, unlike ONFH, is a self-limiting disease and does not progress to ONFH (Fig. 1).83
DISCUSSION
Our understanding of ONFH and the effects of trauma, medications, as well as genetic and patient factors have changed over the past 3 decades. Recent studies have demonstrated that corticosteroids and alcohol promote adipogenesis in the marrow space, but inhibit osteogenesis and angiogenesis.353684 Genetic factors including thrombophilia, hypofibrinolysis, and impaired angiogenesis also play critical roles in the pathogenesis of ONFH.29 However, the pathophysiology of ONFH is multifactorial and poorly understood. The multisystemic effects of hereditary and acquired risk factors and their interactions make the pathological mechanisms more complicated.
A uniform concept of the pathophysiology of osteonecrosis is vascular occlusion and ischemia of bone leading to bone death. The mechanical interruption of circulation to the femoral head after hip dislocations or femoral neck fractures is the most obvious patho-mechanism. Cellular or gas embolization in the sinusoids probably plays the central role of blood supply occlusion in Gaucher's disease, hemoglobinopathies, and dysbaric disorders. However, the pathogenesis of alcohol- or corticosteroid-associated osteonecrosis is less clear. Marrow fat cell hypertrophy was suggested to contribute to the pathogenesis by compression of the sinusoidal vascular bed, which causes venous stasis and elevated intraosseous marrow pressure.34 Since the marrow cavity is a compartment encased by a non-expandable shell of bone, attention has been focused on elevated intraosseous pressure (IOP) as a pathogenic mechanism. An elevated IOP within the osteonecrotic femoral head and decreased venous drainage and stasis have been shown.40 Other observers have not found IOP measurements to be reproducible, specific, or sensitive for the diagnosis of osteonecrosis.14858687 Elevated IOP is observed not only in osteonecrosis, but also in osteoarthritis and can also be related to elevations in intra-articular pressure and compressive loads.8889 Thus, elevated IOP does not seem to be causally related to the pathogenesis of osteonecrosis and is a nonspecific and secondary, but potentially contributory, factor in the pathogenesis of osteonecrosis. Further studies are necessary in order to identify not only the precise mechanisms of the disease, but also patients at risk for developing ONFH, leading to early prevention and treatment.
Subchondral fracture seems to be the point of no return in the disease progression of ONFH,19 but needs to be differentiated from insufficiency fracture and transient bone marrow edema syndrome. MRI is useful to rule out these conditions. Various pharmacological treatments; enoxaparin, statins, bisphosphonates, iloprost, and acetylsalicylic acid have been given to prevent ONFH in patients at risk or to retard the disease progression in early-stage disease without subchondral fracture or collapse of the femoral head. However, their effectiveness remains controversial and none of them were proven to be effective by high-level studies. At this moment, no pharmacological prevention or treatment of ONFH is recommended.90
Core decompression has been performed to treat ONFH under the assumption that it reduces intraosseous pressure, allows restoration of blood flow, regenerates necrotic bone, and thus can control or reverse the disease process. Grafting of concentrated bone marrow mononuclear cells (BMMC) has been combined to core decompression to treat the early stage of ONFH, and several studies showed promising results.91929394959697 Given that size and location of the necrotic lesion are the major determinants of further collapse of the femoral head and collapse does not occur in small lesions even without any intervention,199899 there is limited evidence to confirm the effectiveness of BMMC therapy in well-designed studies. Thus, a large-scale randomized controlled trial to verify the efficacy of core decompression with/without BMMC is warranted.
In summary, the exact pathogenesis of ONFH is still unknown. Most investigators agree that ONFH has a multifactorial etiology but progression of the disease occurs through one final common pathway, which is decreased blood flow to the femoral head that leads to ischemia and cell death. Attention has been given to the interplay between individual genetic predispositions and associated risk factors that can potentially lead to the final common pathway, but an important knowledge gap persists in terms of when and how those factors interact to lead to tissue ischemia and necrosis. Therefore, well-designed basic science studies and hypothesis-driven, prospective, randomized, controlled, large scale clinical trials are needed.
 XML Download
XML Download