

 PDF
PDF Citation
Citation Print
Print



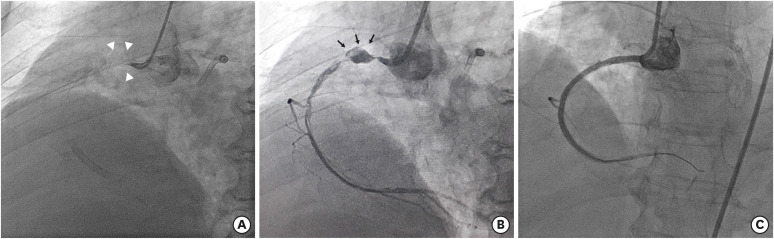
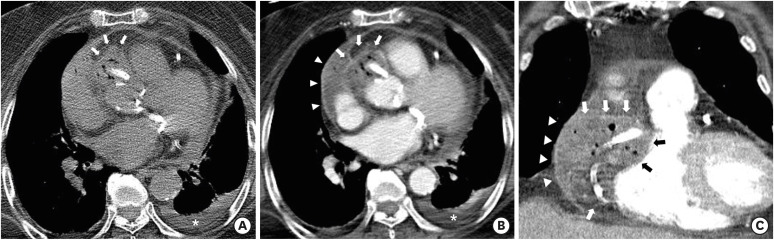
A 74-year-old female with a history of diabetes and multiple coronary stent insertion [right coronary artery (RCA) and left anterior descending coronary artery] presented to the emergency department (ED) with acute chest pain. Electrocardiogram (ECG) in the ED showed ST elevation in the II, III, and aVF leads as well as increase in the serum troponin T (0.312 ng/mL, normal range 0–0.1 ng/mL), indicating ST-segment elevation myocardial infarction. Occlusion of RCA at its origin was identified on immediate percutaneous coronary intervention (PCI). After balloon dilation of the occluded segment, a pseudoaneurysm was demonstrated at the proximal portion of the RCA, suggesting rupture (Figure 1). PCI was successfully performed although pseudo-aneurysm was developed during the procedure (Figure 1). On hospital day 8, the patient developed a fever (38.5°C). An epicardial coronary abscess with multiple air-pockets and rim-enhancement extending into the right atrioventricular (AV) groove and pericardium was identified on the chest computed tomography (CT) (Figure 2). Klebsiella pneumoniae was identified on blood cultures. Subsequent open heart surgery confirmed the CT findings, and removal of necrotic tissue and abscess with drainage catheter placement was done without extraction of RCA stent. After 6 weeks, the patient was improved and discharged.
Coronary stent infection has several risk factors (i.e., virulence of the pathogen, host response, device properties, and procedural difficulty). The most common cause of coronary stent infection is procedure-related infection from the skin or catheters, often due to Staphylococcus aureus (80%) followed by Pseudomonas aeruginosa (20%).1)2)3) In previous reports, the primary tool to identify coronary stent infection was the identification of pseudoaneurysm formation on coronary angiography.1)2)3) However, coronary angiography only visualizes a portion of the overall abscess pocket. In contrast, CT can evaluate the overall extent of coronary stent infection, facilitating proper therapeutic planning. In this regard, the case shows the value of CT in diagnosing complications of coronary stent infection and providing appropriate treatment planning.
 XML Download
XML Download