

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
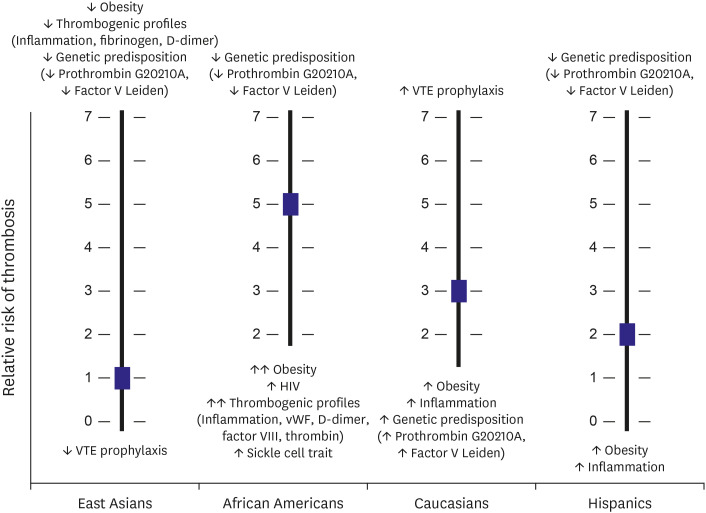
Multiple lines of clinical and epidemiologic evidence have suggested that the prevalence of atherosclerotic cardiovascular disease (ASCVD) and related mortality rates differ between patients of different races (Figure 1).1)2)3)4) Compared with East Asians, Caucasians have greater morbidity and mortality from coronary artery disease (CAD).2)3) Morbidity and mortality related to stroke are higher in East Asians than in Caucasians, which may be partly explained by a higher incidence of hemorrhagic stroke in East Asians and the different dominant type of ischemic stroke (i.e., lacunar stroke in East Asians vs. large thromboembolic stroke in Caucasians). Similarly, the incidence of venous thromboembolism (VTE) varies according to race (Figure 2), with African Americans having approximately fivefold greater incidence than individuals from Asian-ancestry populations, and an intermediate risk in Caucasians and Hispanics.4)
Figure 1
Age-adjusted death rates for CAD and stroke by race/ethnicity (deaths per 100,000 men of 35–74 years old). This figure was modified from the original version.2)
CAD = coronary artery disease; ICH = intracranial hemorrhage.
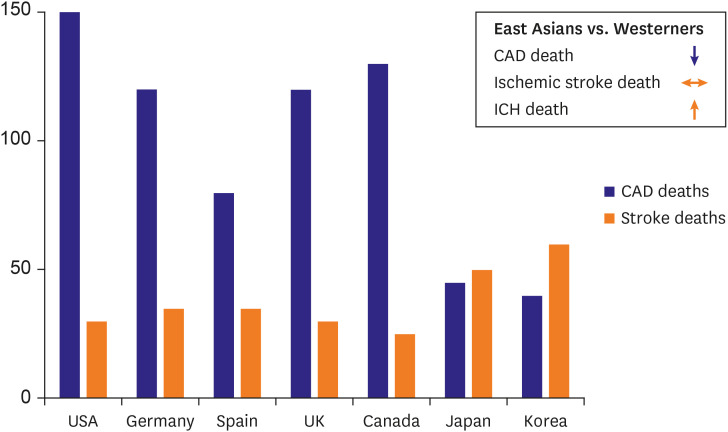
Figure 2
Risk of VTE across race & postulated mechanisms. This figure was modified from the original version.1)
HIV = human immunodeficiency virus; VTE = venous thromboembolism; vWF = von Willebrand factor.
The unusually low incidence and mortality associated with CVD in East Asians is important, since the dosage and strategy for cardiovascular (CV) therapies in the American and European guidelines were based on clinical evidence collected from a Western population.5) Differences in traditional CV risk factors may not completely account for this racial disparity, nor do known ethnic variations in environmental risk factors. These special phenomena are constantly observed, even in individuals of different ethnicities living within the same geographical location.3)6) In this review, we discuss the racial difference in thrombogenicity and its impact on atherothrombotic events and propose an ethnicity-tailored antithrombotic strategy in ASCVD patients.
INTRINSIC THROMBOGENICITY AND ITS RELATION TO ATHEROTHROMBOTIC EVENTS
Underlying mechanisms associated with the racial disparity in ASCVD incidence and mortality are complex and multifactorial.1)7) The ethnic differences in demographics, comorbidities, and disease patterns can influence clinical outcomes. In addition, the polygenic aspect of inherited thrombogenicity (hypercoagulability), and the complex interaction between genetic and epigenetic factors may in part explain the ethnic differences.
The processes of arterial and venous atherothrombosis are finely regulated and involve a highly complex interplay between blood components (vulnerable blood), the vessel wall (vulnerable vessel) and hemodynamic variables (stasis, turbulence) (Virchow's triad).8)9) There is insufficient evidence to support race-dependent differences in endothelial dysfunction and blood stasis. Hemostasis is a complex process composed of biochemical reactions involving both cellular elements (e.g., platelet and inflammatory cells) and plasma factors (inflammatory, procoagulant, anticoagulant and fibrinolytic factors). There are a lot of clinical evidence suggesting racial differences in coagulation, fibrinolysis and inflammation profiles.10)
VTE consisting of deep venous thrombosis (DVT) and pulmonary embolism is a common and potentially preventable entity of CVD.4) VTE occurrence may be associated with a complex interplay between genetic and environmental risk factors. The incidence varies by race: individuals from African and European ancestry have the highest risk and other ethnicities show a lower risk. Figure 2 suggests potential mechanism for racial differences in VTE incidence.1)4)6) Genetic variants with the two known polymorphisms associated with VTE risk (factor V Leiden and prothrombin gene polymorphism) found predominantly in European population are believed to account for up to 60% of VTE.11) Abnormalities in coagulation factors such as deficiencies in protein C, protein S and antithrombin, and elevated factors VIII and XI are at least partially heritable (heritability between 30% and 60%). Also, inflammation is an important risk factor for VTE.12) African Americans exhibit the highest levels of inflammation, and the lowest is in East Asians.
The thrombo-inflammatory axis, as well as residual lipid and diabetic risks, are important targets of key residual risk pathways in the secondary prevention of CAD.13)14) Atherosclerosis has been considered as a chronic inflammatory state induced by cholesterol. In patients with stable ASCVD, the balance between key drivers of atheroma progression can be modified over time.13) For example, an observational study in patients treated with carotid endarterectomy revealed important time-dependent changes in plaque morphology and composition, including the extent of inflammatory infiltrates and reductions in LDL-cholesterol.15) Diverse inflammatory pathways play critical pathologic roles in 1) driving the progression of atherosclerosis in the clinically stable phase of ASCVD; 2) inducing plaque destabilization thereby precipitating acute coronary syndromes (ACS); and 3) responding to cardiomyocyte death resulting from the thrombotic occlusion during myocardial infarction (MI).13)14)
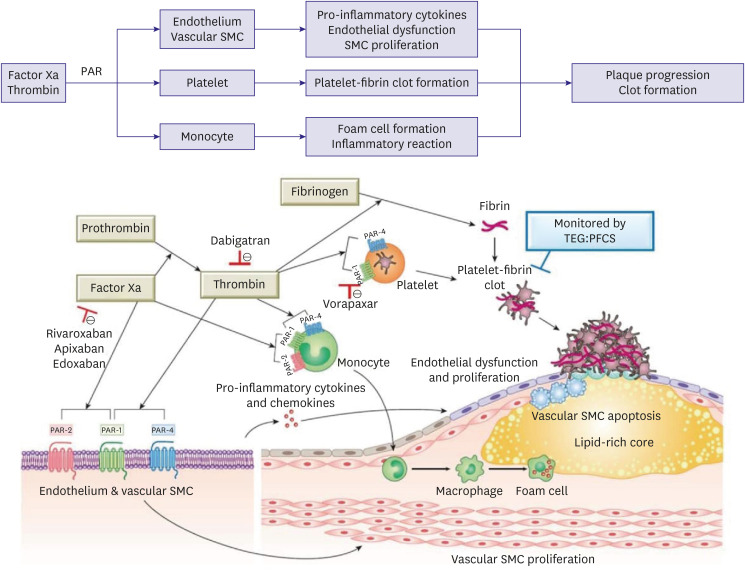
In addition to inflammation, the coagulation cascade also contributes to the progression of atherosclerosis and the occurrence of atherothrombotic events (Figure 3).16)17) Factor Xa and thrombin, via proteinase-activated receptors (PARs), can regulate the function of endothelial cells, leukocytes, and vascular smooth muscle cells (SMCs). PAR-mediated signaling is involved in endothelial cell activation and dysfunction, promoting the recruitment and migration of inflammatory cells into the atherosclerotic lesion, and proliferation and apoptosis of vascular SMCs. Sustained inflammation in the lesion induces plaque instability and promotes plaque rupture and thrombus formation. Thrombin is critical for platelet activation (via PAR1 and PAR4) and fibrin formation, which contribute to platelet aggregation and thrombus formation after plaque rupture. Several clinical studies indicated a close association between coagulation and the risk of CAD. In the Northwick Park Heart study (Caucasian men aged between 40 and 64; n=1,511), high levels of factor VII and fibrinogen were significantly associated with increased risk of CAD occurrence, especially for events occurring within 5 years of recruitment. The latter associations seemed to be stronger than the influence of cholesterol.18) In a combined meta-analysis, hemostatic genetic variants with factor V Leiden and prothrombin G20210A increased the risk of CAD occurrence by about 1.2- and 1.3-fold, respectively.19)
Figure 3
Role of coagulation cascade in progression of atherothrombosis. Factor Xa and thrombin contribute to atherothrombotic events through various mechanisms. Factor Xa (via PAR-1 and PAR-2) and thrombin (via PAR-1 and PAR-4) regulate the activation of endothelial cells, leukocytes, platelets, and vascular SMCs. PAR-mediated signaling are involved in endothelial cell activation and dysfunction, inflammatory process by production of pro-inflammatory cytokines and chemokines, and proliferation and apoptosis of vascular SMCs. Sustained inflammation in the lesion induces plaque instability and promotes plaque rupture. Thrombin is critical for platelet activation (via PAR-1 and PAR-4) and fibrin formation, which contribute to platelet-fibrin clot formation after plaque rupture. This figure was modified from the original version.17)
PAR = protease-activated receptor; PFCS = platelet-fibrin clot strength; SMC = smooth muscle cell; TEG = thromboelastography.
RACIAL DIFFERENCES IN THROMBOGENICITY COMPONENTS
Various international societies have recently emphasized the unmet need for ethnicity-based CVD research. The comparison of major biologic pathways with biomarkers or surrogates provide important clues to explain the racial difference in ASCVD prognosis (Table 1).1)20) However, most CHD biomarker research has been conducted in Caucasians, and little is known regarding the actual generalizability of these biomarkers to other ethnic groups.7) Previous studies indicated that there are marked differences between the races in traditional CV risk factors and the linkage of risk score with observed clinical events,21)22) making it difficult to generalize the clinical data derived from current biomarkers and image criteria to all ethnicities. For example, Framingham risk scoring systematically overestimated the absolute CAD risk in the East Asian cohorts, up to about 7 times in men.23)24)25) The Coronary CT Angiography Evaluation for Clinical Outcomes: An International Multicenter (CONFIRM) registry evaluated the prognostic significance of CAD on coronary computed tomographic angiography according to ethnicity (n=16,451).26) The annualized incidence of death or MI comparing obstructive CAD (≥50% stenosis) to no obstructive CAD among Caucasians was 2.2% vs. 0.7% (adjusted hazard ratio [aHR], 2.77; 95% confidence interval [CI], 1.73–4.43; p<0.001), among Africans 4.8% vs. 1.1% (aHR, 6.25; 95% CI, 1.12–34.97; p=0.037), and among East Asians 0.8% vs. 0.1% (aHR, 4.84; 95% CI, 2.24–10.9; p<0.001). Compared to other ethnicities, East Asians had fewer events than expected (aHR, 0.25; 95% CI, 0.16–0.38; p<0.001).
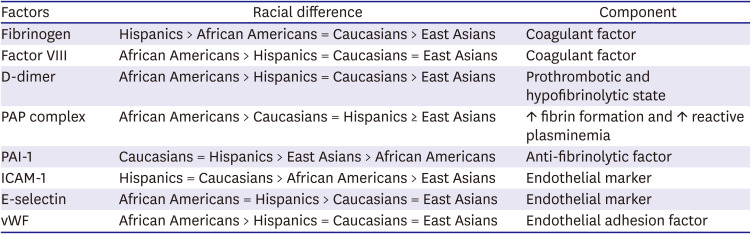
Table 1
Racial differences in thrombogenicity components
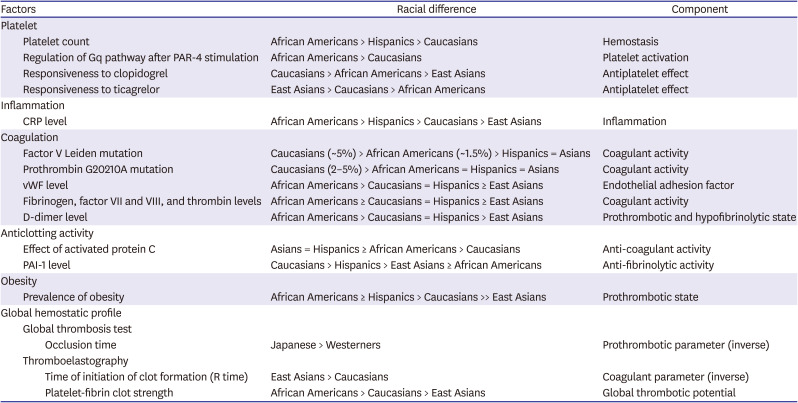
East Asians shows a lower level of intrinsic thrombogenicity compared with Caucasians,7) which may in part explain the lower morbidity and mortality associated with ASCVD in East Asians compared to Westerners. Several epidemiologic studies have suggested the different levels of inflammation (e.g., high-sensitivity C-reactive protein [hs-CRP]), hemostatic factors (e.g., fibrinogen, D-dimer, factor VIII) and plasma endothelial activation markers (e.g., von Willebrand factor, E-selectin) between the races.7)27)28) For example, in the Multi-ethnic Study of Atherosclerosis (MESA) study including healthy individuals living in the USA, African Americans generally had the most thrombogenic and endothelial dysfunction profiles, followed by Hispanics and Caucasians with similar levels and finally lowest in East Asians (Table 2).28)
Table 2
MESA cohort: racial differences in endothelial and hemostatic biomarkers (healthy American citizens)
This table was modified from the original version.28)
ICAM-1 = intercellular adhesion molecule-1; MESA = multi-ethnic study of atherosclerosis; PAI-1 = plasminogen activator inhibitor-1; PAP = plasmin-antiplasmin; vWF = von Willebrand factor.
Hemostasis is a finely regulated process composed of ~80 biochemical reactions including both cellular elements and plasma proteins. However, routine coagulation tests and biomarkers are mostly focused on a specific pathway and ignore the interaction of cellular elements and plasma proteins including procoagulant and endogenous anticoagulant factors.29) Global hemostatic assays can reflect the interaction between these factors, better indicate intrinsic hemostatic capacity, and assist in differentiating the mechanism(s) associated with clot generation and finally in predicting clinical outcomes.
Platelet count and function
Platelets are implicated in hemostasis, arterial thrombosis, and also other physiological and pathophysiological processes.30) At the site of an inflamed vessel wall, platelets interact with leukocytes and the coagulation system, thereby mediating thrombo-inflammation and promoting atherosclerosis progression and vascular remodeling. Therefore, platelet counts and functions are significantly associated with the risk of ASCVD and related mortality.30)31)32)
There are significant differences in platelet count and functions across the races. After controlling for age and sex, African Americans had significantly higher platelet counts than Caucasians, with Hispanic Americans having intermediate counts.33) Platelet gene polymorphisms may be associated with variable platelet reactivity that may vary by race. Platelet aggregation induced by the PAR-4 thrombin receptor agonist was significantly greater in African Americans than in Caucasians.34)35) In addition, African Americans showed a higher prevalence of high on-treatment platelet reactivity (HPR), and reduced responsiveness to aspirin and P2Y12 receptor inhibitors compared with to Caucasians.36)37) These findings suggest that African Americans exhibit reduced response to dual antiplatelet therapy (DAPT), which may in part explain the worse clinical outcomes after coronary stenting.38)39)
Inflammation
Coronary and systemic inflammation may both precipitate atherothrombosis and myocardial necrosis following MI.40) Early clinical studies demonstrated associations between hs-CRP and serum amyloid A with in-hospital adverse CV events among ACS patients. Subsequent studies evaluated diverse pro-inflammatory mediators such as cytokines (interleukins, tumor-necrosis factor alpha), adhesion molecules (intercellular adhesion molecule-1, vascular cellular adhesion molecule-1), and acute phase reactants (CRP, fibrinogen).13) Most studies have observed a close relationship between the level of hs-CRP and the occurrence of CV events in primary and secondary prevention of ASCVD.41)42)43) In ACS patients treated with percutaneous coronary intervention (PCI), hs-CRP levels appear to predict recurrent CV events beyond markers of infarct size even in patients on statin treatment.41)42)
There are significant racial differences in inflammatory activity. Overall, African Americans exhibit the highest, and East Asians appear to have the lowest levels of inflammation.27)44)45) In a recent meta-analysis (n=221,287),46) geometric mean CRP was 2.60 mg/L (95% CI, 2.27–2.96) in African Americans; 2.51 mg/L (95% CI, 1.18–2.86) in Hispanics; 2.34 mg/L (95% CI, 1.99–2.8) in South Asians; 2.03 mg/L (95% CI, 1.77–2.3) in Caucasians; and 1.01 mg/L (95% CI, 0.88–1.18) in East Asians, which were persisted after adjustment for age and body mass index.
A large-scale Korean registry from a health screening program (n=268,803) demonstrated low hs-CRP level in Koreans and its linear association with both CVD and all-cause mortality (p<0.001).43) Since hs-CRP is dynamically changed during the acute phase in ACS patients, its persistent elevation during the stabilized period may be a more reliable risk marker for clinical outcomes. In PCI-treated patients, persistent high inflammation (hs-CRP >2 mg/L at baseline and follow-up with ≥4-week interval) was observed in 37.8% of the American cohort (n=7,026)47) and only 17.9% of the Korean cohort (n=5,115).48) In both races, persistent high inflammation was related to a significant increase in the risk of ischemic event compared to persistent low inflammation (HR, 1.72 and 2.01, respectively). Therefore, the different inflammation levels may contribute to diverse ischemic outcomes between the races in high-risk CAD patients.
Coagulation
Factor V Leiden and prothrombin G20210A are the most common single nucleotide polymorphisms associated with inherited thrombophilia, and have been associated with DVT and CAD.4)19) ASCVD patients have higher thrombin generation compared with those without ASCVD.16) In addition, the level of coagulation activity reflected by fibrinogen and D-dimer is closely related to the increased risk of atherothrombotic events in high-risk ASCVD patients, including patients with ACS or coronavirus disease 2019 (COVID-19) infection.49)50)51)
There are significant racial differences in coagulation. Factor V Leiden allele is present in about 5% of Caucasians, about 1.5% of African Americans, and is virtually absent in Asians. Due to this mutation, activated protein C (APC, an anticoagulant protein) is not able to bind normally to Factor V, leading to a hypercoagulable state. Prothrombin G20210A mutation is present in 2–5% of Caucasians, whereas it is rare in other groups.4) Meanwhile, African Americans exhibit a trend toward having higher levels of von Willebrand factor, factor VIII, thrombin generation, and D-dimer.4)52) Compared to subjects from other ethnic background, East Asians have the lowest levels of fibrinogen, factor VIII and D-dimer.7)28)
Anticlotting activity (anticoagulant and fibrinolytic mechanisms)
Activation of the coagulation cascade leads to the thrombin generation (factor IIa) which then converts fibrinogen (factor I) to fibrin. Physiological anticoagulant mechanisms act to reduce thrombin generation or reduce the effects of thrombin: 1) antithrombin–glycosaminoglycan pathways; 2) protein C, protein S, and thrombomodulin; and 3) tissue factor pathway inhibitor (TFPI). A fibrin clot is broken down by fibrinolytic cascade. Its main enzyme, plasmin, cuts the fibrin mesh at various places, leading to the generation of fibrin degradation products.53) Tissue plasminogen activator (t-PA) and urokinase convert plasminogen to the active plasmin. Activities of t-PA and urokinase are inhibited by plasminogen activator inhibitor-1 (PAI-1) and PAI-2. Therefore, inhibition of PAI-1 could lead to clot degradation, whereas activation of PAI-1 could accelerate clot formation. In terms of PAI-1 rs1799889 4G/5G polymorphism, decreased plasma PAI-1 level was detected in patients carrying 5G5G genotypes. PAI-1 rs1799889 4G/5G polymorphism (4G vs. 5G) has been associated with an increased risk of DVT, MI and ischemic stroke.54)55)56)
Impaired endogenous fibrinolysis may be another important mechanism responsible for progression of atherosclerotic lesions and thrombotic events despite conventional antithrombotic therapy.53) In a sub-study of the PLATelet inhibition and patient Outcomes (PLATO) study (n=4,354),57) a turbidimetric assay was employed to evaluate maximum turbidity (an indicator of clot density) and plasma clot lysis time (CLT) in ACS patients. The CLT correlated with CV death and MI at 1 year after adjusting for CV risk factors (HR, 1.17; 95% CI, 1.05–1.31, p<0.01) and correlated with CV death after adjustment for known prognostic biomarkers (leukocyte count, hs-CRP, troponin T, cystatin C, N-terminal pro-B-type natriuretic peptide, and growth differentiation factor-15) (HR, 1.20; 95% CI, 1.01–1.42; p=0.042). Maximum turbidity was associated with increased CV death (HR, 1.24; 95% CI, 1.03–1.50; p=0.024), but not after adjustment for known prognostic biomarkers.
There are few clinical studies to compare directly the level of fibrinolytic activity between the races. In the Insulin Resistance Atherosclerosis Study (IRAS) study,58) PAI-1 levels differed amongst patients from different ethnic backgrounds (non-Hispanic whites > Hispanics > blacks, p<0.0001). The significant linkage of PAI-1 rs1799889 polymorphism (4G vs. 5G) to the risks of DVT, CAD and ischemic stroke was more prominent in the Asian population.55)56) Limited studies have also identified lower levels of circulating protein C and protein S, and endogenous anticoagulants in African Americans.59)60)
Obesity
Obesity is a major risk factor for death in patients with ASCVD.61) Obesity is characterized by systemic oxidative stress and chronic low-grade inflammation, consequently associated with endothelial dysfunction, platelet aggregation, hypercoagulability indicated by thrombin activation, and impaired fibrinolysis due to increase in PAI-1 and TAFI, and finally progression to ASCVD (Figure 4).62)63) Recent pre-clinical data also showed that obesity was associated with VTE mediated by thrombo-inflammation cascade including von Willebrand factor.64) The prevalence of obesity varies according to race and geography. Mostly, African Americans and Caucasians have higher rates of obesity compared with Asians.4)61)

Global hemostatic assay
A specific biomarker assessment may only show a part of hemostasis and does not provide quantitative information on platelet function, thrombin generation, and the kinetics of clot formation.53) Some of these limitations can be overcome by assessment with a global viscoelastic hemostatic assay (e.g., thromboelastography [TEG], rotational thromboelastometry [ROTEM], or global thrombosis test [GTT]).29)65) The latter assays reflect the interaction between cellular elements and plasma proteins, which can better represent hemostatic capacity and assist in evaluating the mechanism(s) associated with clot generation and ischemic and bleeding outcomes.1)53)66)
The TEG assay is a whole blood ex vivo assay that provides dynamic viscoelastic properties of the clot from the time of initial plasmatic thrombin generation to platelet-fibrin dependent clot formation to clot strengthening to clot lysis (Figure 5A).29) TEG parameters reflect platelet function and coagulation, the response to antiplatelet and anticoagulant agents, and fibrinolytic activity.66) Maximal amplitude (MA: an indicator of platelet-fibrin clot strength [PFCS]) is considered to be a reflection of the absolute strength of the final hemostatic plug and is a whole reflection of the dynamic properties of fibrin, platelet number, and their functional status.67) A recent report showed close associations between PFCS and several conventional coagulation parameters (prothrombin time, r=0.154; fibrinogen, r=0.334; hemoglobin, r=−0.279; platelet count, r=0.301) (all p values ≤0.001).29)
Figure 5
(A) TEG parameter and (B) the level of platelet-fibrin clot strength (MA) across the races.
ANOVA = analysis of variance; CAD = coronary artery disease; MA = maximal amplitude; TEG = thromboelastography.

Several studies have compared the TEG measurement between the races. In patients with known or suspected CAD on clopidogrel therapy (n=924), African American patients showed greater level of PFCS than European Americans (67.8±7 vs. 66.4±6 mm, p=0.005) (Figure 5B), but there was no difference in platelet aggregation between the races.68) In a multivariate analysis, sex, race, diabetes, platelet count, and hemoglobin were independently associated with the level of PFCS. In age- and sex-matched East Asians vs. Caucasians with stable CAD (n=249 each), TEG measurement demonstrated delayed initiation of clot formation (R time), lower clot strength (MA: 61.8±7.9 vs. 65.4±5.0 mm, p<0.001), and relatively greater clot lysis (LY30).29) During three-year follow-up, high PFCS (≥68 mm) was significantly associated with the occurrence of ischemic events (odds ratio [OR], 6.27; 95% CI, 2.41–16.30; p<0.001), and East Asians had lower prevalence of high PFCS than Caucasians (OR, 0.50; 95% CI, 0.27–0.93; p=0.028). Taken together, African Americans exhibit the highest and the East Asians exhibit the lowest thrombogenic tendency. This observation may explain in part the ethnic disparity in clinical outcomes among CAD patients.1)
EMERGING ISSUES RELATED WITH THROMBOGENICITY
Racial differences of clinical outcomes in coronary artery disease patients
Significant clinical data show the racial differences in clinical outcomes in CAD patients. Comparative clinical data from high-risk ASCVD patients have indicated that East Asians have lower rates of atherothrombotic events compared with Westerners. The Reduction of Atherothrombosis for Continued Health (REACH) registry (n=49,602) enrolled outpatients with CVD or multiple CV risk factors.69) The use of CV medical therapies was comparable to reduce risk among all groups. At 2-year follow-up, the rate of CV death was significantly higher in Blacks (6.1%) compared with all other ethnic/racial groups (3.9%; p=0.01). CV death rates were significantly lower in all Asian racial group (2.1%) compared with the other groups (4.5%; p<0.001).70) In the Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management, and Avoidance (CHARISMA) study (n=15,603; a median of 28 months),71) compared to other races, Asian patients had numerically the lowest prevalence of ischemic events (Asians vs. Hispanics Whites vs. Blacks: 6.2% vs. 6.8% vs. 7.1% vs. 8.6%, respectively) and a greater tendency for serious bleeding (Asians vs. Hispanics vs. Whites vs. Blacks: 2.5% vs. 1.2% vs. 1.7% vs. 3.5%, respectively) during antiplatelet therapy.
Another analysis from the National Cardiovascular Data Registry (NCDR) database (n=423,965 American citizens) also supported the favorable clinical outcomes in Asians following PCI.72) Asian patients exhibited a lower prevalence of death and MI compared with Caucasians (HR, 0.989; 95% CI, 0.822–0.963; p=0.004). The occurrence of stent thrombosis following implantation of first-generation drug-eluting stent increased concerns about interethnic differences: annually 0.2% and 0.6% risk in East Asian and European registries, respectively.73)74)75) A recent large pooled database of 10 randomized clinical trials (RCTs) (n=22,638) assessed the race-based difference of ischemic endpoint (death, MI and ischemia-driven revascularization) in PCI-treated patients.39) Five-year major CV event rates were 18.8% in white patients (reference group), compared with 23.9% in black patients (p=0.0009), 11.2% in Asian patients (p=0.0007), and 21.5% in Hispanic patients (p=0.07). Multivariate analysis demonstrated an independent association between black race and CV event occurrence (HR, 1.28; 95% CI, 1.05–1.57; p=0.01).
In high-risk ASCVD patients such as the PCI-treated cohort, East Asians have shown the best clinical outcomes, followed by Hispanics and Caucasians with similar levels, with the worst outcomes observed in African Americans. This trend appears very similar to the order of thrombogenic profile (Table 1), but more research is needed to show a strong connection between race, thrombogenicity and clinical outcomes.
Optimal antithrombotic strategy in East Asian patients (‘East Asian Paradox’)
Multiple experimental and clinical data have shown that East Asians have a lower level of intrinsic thrombogenicity compared with Caucasians (Tables 1 and 2). The relative contribution of platelet reactivity and coagulation to ischemic and bleeding events may be race-specific. In addition, East Asians have a greater tendency for gastrointestinal bleeding and intracranial hemorrhage (ICH), compared with Caucasians.1)76)77)78) Therefore, the therapeutic target for optimal antithrombotic effect may be relatively different between East Asians and Caucasians. In addition, East Asians have different responses to antithrombotic regimens compared to Caucasians. Most antithrombotic agents show enhanced pharmacokinetic and pharmacodynamic profiles in East Asian vs. Caucasian subjects, except for clopidogrel and edoxaban (Table 3).1)
Table 3
Level of active metabolite concentration in East Asians vs. Caucasians

| P2Y12 receptor inhibitors | Direct oral anticoagulants | ||
|---|---|---|---|
| Clopidogrel | ↓↓ | Dabigatran | ↑ (20–30%) |
| Prasugrel | ↑↑ (30–47%) | Rivaroxaban | ↑ (20–30%) |
| Ticagrelor | ↑↑ (40–48%) | Apixaban | ↔ |
| Edoxaban | ↓ (20–25%) | ||
This table was modified from the original version.1)
The concept of the ‘East Asian Paradox’ was first described to explain the racial difference in the therapeutic window for on-clopidogrel platelet reactivity.79) In addition, the unique feature of East Asians for ischemia-bleeding trade-off was also observed with newer antithrombotic treatments such as potent P2Y12 inhibitors and direct oral anticoagulants (DOACs). The recent consensus document updated this concept into the development of a unique antithrombotic strategy for East Asians,1) with different pharmacodynamic profiles of antithrombotic agents, low benefit in reducing ischemic events, and high risk in increasing bleeding events during antithrombotic treatment.
In high-risk patients treated with PCI, duration, and potency of DAPT should be determined depending on the balance between clinical efficacy and hazard. The unique balance between ischemic benefit and bleeding risk in East Asian patients may influence the optimal DAPT strategy. A meta-analysis including PCI-treated patients (7 RCTs, n=16,518) suggested a different level of ischemic risk and bleeding during aspirin monotherapy or DAPT (Figure 6).80) Ischemic events occurred more frequently in Western patients (0.8% vs. 1.8%, p<0.001), while major bleeding occurred more frequently in East Asians (0.6% vs. 0.3%, p<0.001). Furthermore, the proportion of patients with a higher probability of bleeding than ischemia during DAPT was elevated in East Asian vs. Western patients (32.3% vs. 0.4%, p<0.001).80)81)
Figure 6
Ischemic and bleeding events according to prolonged- vs. short-term DAPT in East Asians vs. Westerners. This figure was modified from the original version.81)
DAPT = dual antiplatelet therapy.

The duration of DAPT to achieve superior clinical benefit may be shorter in East Asian patients compared with Western patients, which has been supported by the results of recent large-scale RCTs performed in East Asian countries.82)83)84) Likewise, standard-dose potent P2Y12 inhibitors (i.e. prasugrel, ticagrelor) showed increased bleeding risk and limited anti-ischemic benefit compared with clopidogrel in East Asian patients with ACS.85)86)87) A large-scale RCT88) and consensus documents5)77) suggested the clinical benefit of reduced-dose prasugrel and ticagrelor in East Asian patients presenting with ACS.
In patients with atrial fibrillation (AF), DOACs are the preferred oral anticoagulants over warfarin, but ICH risk in Asian patients on the same dose of DOAC appeared relatively higher compared with non-Asian patients.89) DOACs demonstrate differing pharmacokinetic profiles between East Asians compared to Caucasians (Table 3).1) Similar to the case with P2Y12 inhibitors, Asian patients have an increased risk of major bleeding and ICH with relatively lower DOAC concentrations compared with non-Asians.90) There are increasing numbers of patients with AF who undergo PCI for CAD, where combination therapy comprising of DOAC and antiplatelet therapy is mandatory. Western guidelines recommend full dose DOAC even in AF patients undergoing PCI.91) However, East Asian patients with AF undergoing PCI or transcatheter aortic valve replacement were mostly treated with reduced-dose DOACs.92)93) For example, the Atrial Fibrillation and Ischemic Events With Rivaroxaban in Patients With Stable Coronary Artery Disease (AFIRE) trial performed with Japanese patients used 54% of 15-mg rivaroxaban and 46% of 10-mg rivaroxaban, respectively.92) Therefore, there is an unmet need to evaluate the best combination strategy with DOAC and antiplatelet therapy in these patients with respect to dose and duration.
Racial differences of clinical outcomes in coronavirus disease 2019 patients
COVID-19 infection appears to progress in 3 phases: 1) initial illness caused by active infection; 2) a second pulmonary phase; and 3) a third severe phase characterized by hyper-inflammation, cytokine storm, high cardiac injury biomarker levels, and significant morbidity and mortality.94) This disease predisposes patients to thrombosis with arterial and venous blood clots (COVID-19 coagulopathy).95)96) The mechanisms underlining COVID-19 coagulopathy are not fully understood and likely due to multiple processes including inflammation, oxygen demand injury, and plaque rupture triggered by the infection. Platelets may be hyperactivated, have an increased prothrombotic potential, and contribute to the elevated inflammatory cytokine pool that underlines the fatal course of COVID-19.97) Severe systemic inflammation results in enhanced activation of coagulation and thrombosis (thrombo-inflammatory syndrome). Therefore, the prothrombotic state may play a central role in the prognosis of COVID-19 patients with increased coagulopathy.
Severe COVID-19 is associated with high levels of D-dimer, fibrinogen and von Willebrand factor, and low level of antithrombin.98) Individuals of African descent living in the United States or European countries have worse outcomes with COVID-19 than Caucasians and Asians.52) Their vulnerability is not fully explained by the differences in social and economic factors.20) Activity of coagulation-inflammation cascade and predisposition to the development of coagulopathy varies between the races, with African Americans trending toward a more prothrombotic state (Tables 1 and 2).1)4)20)99) Low level of thrombo-inflammatory activity in East Asians may be related to the better outcomes following COVID-19 infection,29) but this hypothesis needs more supportive experimental data.
D-dimer is the most widely used biomarker to assess COVID-19 severity and outcomes, with an escalation of antithrombotic therapy recommended in patients with very high D-dimer levels.100) However, there are several limitations of this biomarker to monitor COVID-19 coagulopathy. Despite observed elevation in D-dimer in patients with severe COVID-19, VTE was not evident in the majority.20) High D-dimer in COVID-19 may be associated with a prothrombotic state, a hypofibrinolytic state, or both. Whole blood viscoelastic analysis can be rapidly performed by TEG or ROTEM, which measure the whole blood capability to make and sustain clot formation including the dynamics of coagulation, platelet function and fibrinolysis. This assay can quantitate the response to both anticoagulant and antiplatelet therapy. The current data have demonstrated a hypercoagulable and hypofibrinolytic state in patients with COVID-19 infection.66) Compared with D-dimer and fibrinogen levels, fibrinolysis shutdown determined by TEG (defined as LY30 < 0.8%) showed the strongest power to predict occurrence of VTE events in severe COVID-19 infection.101) Several ongoing trials including the Evaluation of Hemostasis by Thromboelastography, Platelet Function Testing, and Biomarker Analysis in Hospitalized COVID-19 Patients (TARGET-COVID: NCT04493307) study will investigate the influence of the early detection in hypercoagulability on COVID-19 outcomes.
CONCLUSION
It is common practice that most countries follow western CV treatment guidelines that are based on the results from major clinical trials mainly including Caucasian patients. Recent research studies strongly indicate racial differences in intrinsic thrombogenic properties and response to antithrombotic agents. The level of thrombogenicity (or thrombo-inflammatory axis) is closely related to progression of atheroma and the clinical manifestation of atherothrombotic events, with African Americans trending toward the most thrombogenic state and East Asians having the lowest thrombogenic milieu.1) Moreover, East Asian patients have are more prone to bleeding. There is a unique balance between ischemia and bleeding during antithrombotic treatment in these populations. The best choice of combination regimen and DAPT strategy (potency and duration) in the latter population should more focus on reducing severe bleeding events.
The time has come to recognize and develop the “thrombogenicity-tailored CV treatment strategy” based on specific biomarkers or functional assays. Future studies should focus on establishing a particular footprint of these properties in ASCVD patients based on race and ethnicity to help tailor treatment strategy for achieving maximum net clinical benefits.
 XML Download
XML Download