

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cardiac implantable electronic devices (CIEDs) can be programmed to monitor and identify atrial high-rate episodes (AHREs), also described as “subclinical atrial fibrillation (SCAF),” which is defined as asymptomatic atrial fibrillation (AF), atrial tachycardia (AT), and atrial flutter (AFL) of short duration. Individuals may benefit from using CIEDs to detect AHREs as increasing evidence indicates that AHREs are associated with stroke risk. However, the expected stroke risk in patients with AHREs was much lower than that in clinically documented AF patients with similar risk profile.1)2)3)4)5) Most studies used an episode duration longer than 5–6 min to define AHREs,3)6)7)8)9)10) although a reported false-positive rate of 17.3%, making physician review more essential compared with AHREs lasting >6 hours, a false-positive rate of 3.3%.11) Current guidelines on non-valvular AF recommend anticoagulation therapy in patients with CHA2DS2-VASc scores ≥2 and consideration of anticoagulation therapy in patients with CHA2DS2-VASc scores of 1.12)13) Recently, the European Heart Rhythm Association suggested consideration of anticoagulation therapy for patients with AHREs >5.5 hours and with two additional stroke risk factors.14) However, the optimal primary stroke prevention indication and strategy remain uncertain.
Previous studies have reported various predictors of AHREs in patients with CIEDs. In the ASSERT study,1) lower resting heart rate and sinus node disease were associated with the prediction of AHREs. Other studies reported that a history of heart failure predicted AHREs,9) while others reported that a history of recurrent transient ischemic attack (TIA) and heart failure (HF),15) increased age, increased left atrium (LA) size, and lower systolic blood pressure predicted AHREs.16) A meta-analysis including 10 studies found that baseline characteristics; diabetes mellitus (DM); old age; thromboembolism events; congestive heart failure, hypertension (HTN), age ≥75 years, DM, stroke, CHADS2 score; and coronary artery disease (CAD) were not associated with the prediction of AHREs.17) Therefore, AHREs predictors have not been well established and the optimal treatment for preventing stroke primarily in AHREs is uncertain. Thus, the aim of the present study was to prospectively investigate clinical predictors for AHREs and evaluate the clinical development of AF and cardiovascular events according to the presence of AHREs.
METHODS
Study design and methods
The evaluation of AF occurrence in sick sinus syndrome and atrioventricular node disease patients after pacemaker implantation (AF-Pacemaker Study) was a prospective, multicenter, observational study performed in patients with AF aged >18 years attending any of the 11 tertiary hospital centers comprising all geographical regions of Korea. The study enrollment period started in September 2017 and ended in July 2020.
The AF-pacemaker study aims to investigate the occurrence and management (including ablation therapy) of device-detected AF/AT episodes in patients with post-pacemaker implantation through a prospective, non-randomized, non-blinded, observational, multicenter design. The study is conducted in compliance with the ethical rules of the Declaration of Helsinki (2013) as a statement of ethical principles for medical research involving human subjects by The World Medical Association and approved by the Institutional Review Board of Yonsei University Health System (1-2017-0008). This study is registered at ClinicalTrials.gov (NCT03303872). The Ethics Committees of all 11 tertiary hospital centers (Severance Hospital, Seoul National University Bundang Hospital, Seoul National University Hospital, Donga University Medical Center, Keimyung University Hospital, Ewha Womans University Medical Center, Daegu Catholic University Medical Center, Korea University Medical Center, Eulji University Hospital, CHA Bundang Medical Center, and Kangneung Asan Medical Center) approved this study, and all patients provided informed consent for their inclusion.
Study population
The study population included patients 1) eligible for permanent pacemaker implantation based on the 2016 revised Korean indication guideline on cardiac pacemaker implantation, 2) with an estimated atrial pacing percentage >40% under sinus rhythm (Lower rate ≥60 bpm, close hysteresis, and rest rate), 3) estimated ventricular pacing percentage >40% under sinus rhythm (lower rate ≥40 bpm, dual chamber pacing, close hysteresis, and rest rate). Data collection was usually conducted by personnel with no clinical activity assigned to the project. Data were entered into a common electronic database to limit inconsistencies and errors and provided online help for key variables. Each center could see its data and those of the other participating centers.
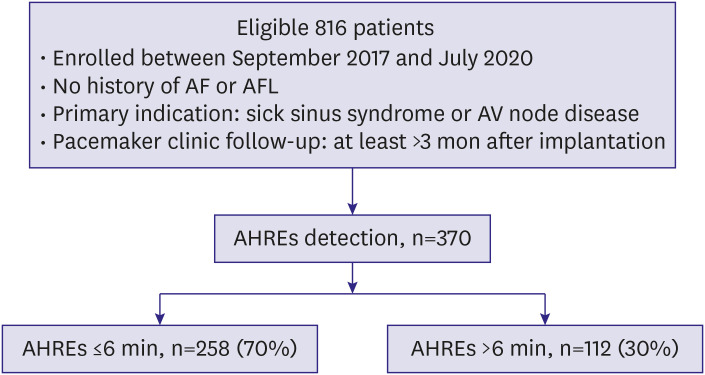
A total of 816 consecutive patients were enrolled at 11 tertiary centers and implanted with a St. Jude Medical dual-chamber rate-adaptive pacemaker (Assurity PM2240) with stored electrogram capabilities for sick sinus syndrome (sinus bradycardia, sinus pause ≥3 seconds, tachy-brady syndrome, sinus node dysfunction, and chronotropic incompetence) or atrioventricular block (high degree/complete atrioventricular block). Patients were eligible for inclusion in the study if they were at least 19 years of age and were available for periodic observation after pacemaker implantation. We excluded patients with severe liver dysfunction (aspartate transaminase/alanine transferase ≥3 times the normal upper limit), severe renal dysfunction (serum creatinine ≥3.5 mg/dL or creatinine clearance ≤30 mL/min) including dialysis, pregnant, lactating, or with malignant cancer, dilated cardiomyopathy, hypertrophic cardiomyopathy, severe valvular heart disease, or life expectancy ≤12 months from enrollment. Patients were also excluded if they had AF at baseline before pacemaker (Figure 1).
Baseline assessment and patient follow-up
We collected data on each patient's baseline demographic characteristics, clinical information, 12-lead electrocardiogram (ECG), laboratory examination, medications, Holter monitoring, treadmill test, and transthoracic echocardiography before pacemaker implantation. The baseline AF rhythm for patient exclusion was reviewed from documented AF on surface ECG/Holter/treadmill test. Device interrogation information was obtained from a clinic visit at 6, 12, and 18 months after pacemaker implantation. There was allowed up to 3 months before and after each clinic visit interval. The AHREs were interrogated to compare ECG traces and pacemaker AHREs data at the end of the ambulatory monitoring period. The clinicians were blinded to the results of the atrial diagnostic data. A Clinical Events Committee classified causes of death and adjudicated all suspected clinical events with blinding to indications of pacemaker implantation. An ECG Core Laboratory reviewed the ECGs and confirmed AF diagnoses.
Pacemaker programming and AHREs detection
The pacemakers incorporated bipolar atrial and ventricular leads (Tendril MRI LPA1200M, Isoflex Optim 1944/1948, Tendril ST Optim 1888TC) in all patients. The atrial and ventricular leads were placed in the right atrial appendage and right ventricular apex, respectively. An AHREs detection rate of 220 beats/min was programmed and storage of up to four atrial electrograms of 12-second duration on automatic detection of AHREs was activated. At every visit, the longest durations of all AHREs were ascertained. The longest AHREs durations were classified >15 vs. ≤15 seconds, >6 vs. ≤6 minutes, and >6 vs. ≤6 hours. Clinical events including cerebrovascular accidents (CVAs), major/minor bleeding, myocardial infarction (MI), and all-cause deaths were recorded.
Statistical analysis
Continuous variables were presented as mean±standard deviations for normally distributed values or medians and interquartile interval (IQI) for non-normally distributed values and categorical variables as numbers and percentages in each group. The baseline characteristics of the two groups were compared using Student's t- or Mann–Whitney U-tests for continuous variables and Pearson's χ2 or Fisher's exact tests for categorical variables. We used a logistic regression model for multivariate analysis to assess predictors of AHREs after adjusting for other clinical events. Based on age, sex, and body mass index (BMI), we built a multivariate logistic model by adding variables that were p values <0.10 into the univariate models. Logistic regression analysis was also used to confirm the statistical significance between AHREs predictors and longest duration. Associations were presented as odds ratios (ORs) with 95% confidence intervals (CIs). All analyses were performed using SAS version 9.4 (SAS Institute) and R version 3.5.2 (R Foundation for Statistical Computing, Vienna, Austria). Two-tailed p values <0.05 indicated statistical significance.
RESULTS
Between September 2017 and July 2020, this study enrolled 816 patients with a median follow-up of 18 months. The median patient age was 73 (65, 79) years and 60% were women. Atrioventricular block (58.1%) was the most common indication for CIEDs implantation, followed by sick sinus syndrome (41.9%). The median CHA2DS2-VASc score was 3 (2, 4); 677 (83.0%) of patients had scores ≥2 and 66.9% had hypertension. The median LA diameter was 40 mm (36, 45), the left ventricular ejection fraction (LVEF) was 65% (60, 70) by transthoracic echocardiography, and the PR interval was 184 ms (164, 204) by electrocardiography. Fifty-five (7.1%) showed atrial premature contraction (APC) at >1% per 24 hours. Overall, 358 (43.9%) patients were taking renin-angiotensin-aldosterone system inhibitors (Table 1).
Table 1
Baseline characteristics of the overall population (n=816)
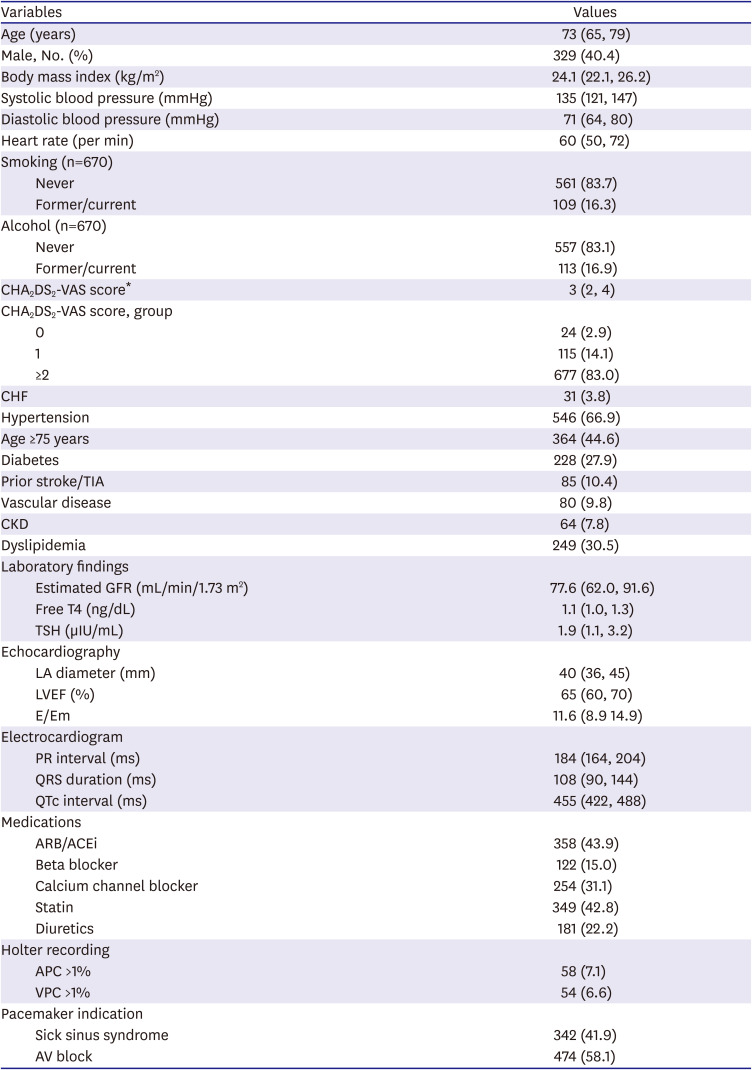
The data are presented as number (%), mean±standard deviation, or median (interquartile interval). Non-parametric continuous variables, as assessed using the Kolmogorov–Smirnov method, were analyzed using the Mann–Whitney U test.
ACEi = angiotensin-converting-enzyme inhibitor; AF = atrial fibrillation; APC = atrial premature complex; ARB = angiotensin receptor blocker; AV = atrioventricular; BUN = blood urea nitrogen; CHF = congestive heart failure; CKD = chronic kidney disease; E/Em = the ratio of the early diastolic mitral inflow velocity (E) to the early diastolic mitral annular velocity (Em); GFR = glomerular filtration rate; LA = left atrium; LVEF = left ventricular ejection fraction; QTc = corrected QT; TIA = transient ischemic attack; TSH = thyroid-stimulating hormone; VPC = ventricular premature complex.
*The CHA2DS2-VAS score is a measure of the risk of stroke in patients with atrial fibrillation, with scoring ranging from 0 to 9 and higher scores indicating greater risk. Congestive heart failure, hypertension, age 75 years or older (doubled), diabetes, stroke (doubled), vascular disease, age 65 to 74 years, sex category (female).
AHRE duration criteria
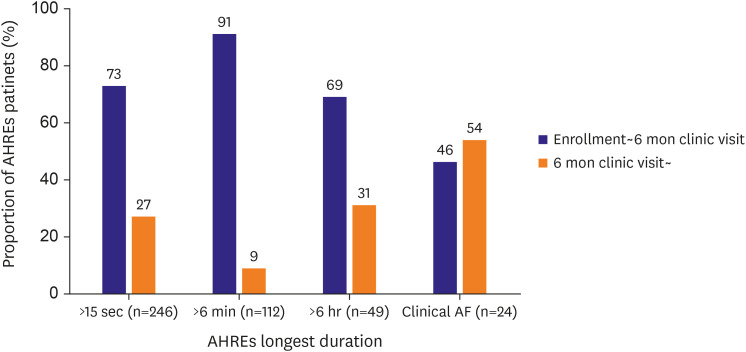
Analysis of the longest AHREs durations showed large variability (Supplementary Table 1). Using the AHREs cut-off, AHREs >6 minutes were identified in 102 (12.5%) patients between enrollment and the 6-month follow-up and 112 (13.7%) patients during the entire study period. Longest AHREs lasting >6 hours were found in 34 (4.2%) patients between enrollment and the 6-month follow-up, and 49 (6.0%) patients during the entire study period. Overall, 24 (2.9%) of the 816 patients experienced newly developed AF, as documented by 12-lead ECG during the follow-up period. In patients with confirmed AHRE, the most AHRE was observed within 6 months after pacemaker implantation. In contrary, more than half of the patients diagnosed with newly detected AF were identified more than 6 months after implantation (Figure 2).
Patient characteristics: longest AHREs duration >6 minutes versus ≤6 minutes
Comparison of the baseline characteristics at the time of CIEDs implantation between the groups with AHREs ≤ or >6 minutes is shown in Table 2. These patients did not differ significantly with respect to age, sex, BMI, estimated glomerular filtration rate, thyroid function, LVEF, E/Em, PR interval, history of smoking, alcohol consumption, proportion of congestive heart failure, HTN, DM, prior stroke/TIA, vascular disease, CHA2DS2-VAS score, chronic kidney disease, and dyslipidemia. Medication use including renin-angiotensin-aldosterone system inhibitors, calcium channel blockers, statins, and diuretics also did not differ significantly between patients with longest AHRE durations >6 and ≤6 minutes. Patients with the longest AHREs durations >6 minutes had larger LA diameter, a higher proportion of APC >1% on Holter monitoring, beta-blockade use, and sick sinus syndrome among CIEDs implantation indications compared to patients with longest AHREs duration ≤6 minutes. Comparison based on a longest AHREs duration cut-off of 6 hours showed relatively differences in LA diameter and proportion of prior stroke/TIA, APC >1% on Holter monitoring, beta-blockade use (Table 3).
Table 2
Baseline characteristics for longest AHRE duration ≤6 min (n=258) versus >6 min (n=112)
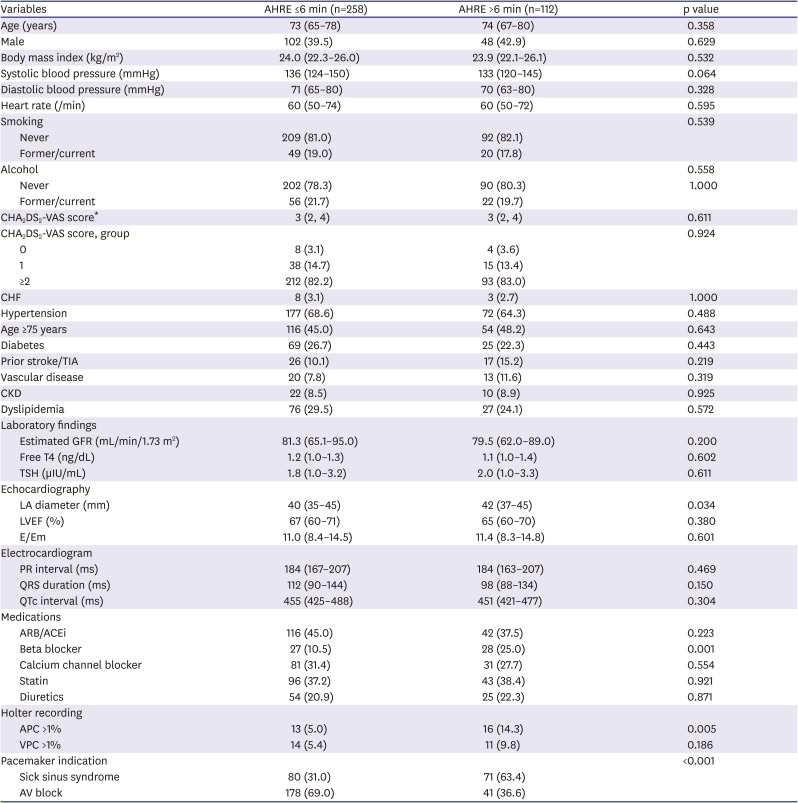
The data are presented as number (%) or median (interquartile interval). Non-parametric continuous variables, as assessed using the Kolmogorov–Smirnov method, were analyzed using the Mann-Whitney U test.
ACEi = angiotensin-converting-enzyme inhibitor; AHREs = atrial high rate episodes; APC = atrial premature complex; ARB = angiotensin receptor blocker; AV = atrioventricular; BUN = blood urea nitrogen; CHF = congestive heart failure; CKD = chronic kidney disease; E/Em = the ratio of the early diastolic mitral inflow velocity (E) to the early diastolic mitral annular velocity (Em); GFR = glomerular filtration rate; LA = left atrium; LVEF = left ventricular ejection fraction; QTc = corrected QT; TIA = transient ischemic attack; TSH = thyroid-stimulating hormone; VPC = ventricular premature complex.
*The CHA2DS2-VAS score is a measure of the risk of stroke in patients with atrial fibrillation, with scoring ranging from 0 to 9 and higher scores indicating greater risk. Congestive heart failure, hypertension, age 75 years or older (doubled), diabetes, stroke (doubled), vascular disease, age 65 to 74 years, sex category (female).
Table 3
Baseline characteristics for longest AHRE duration ≤6 hours (n=321) versus >6 hours (n=49)
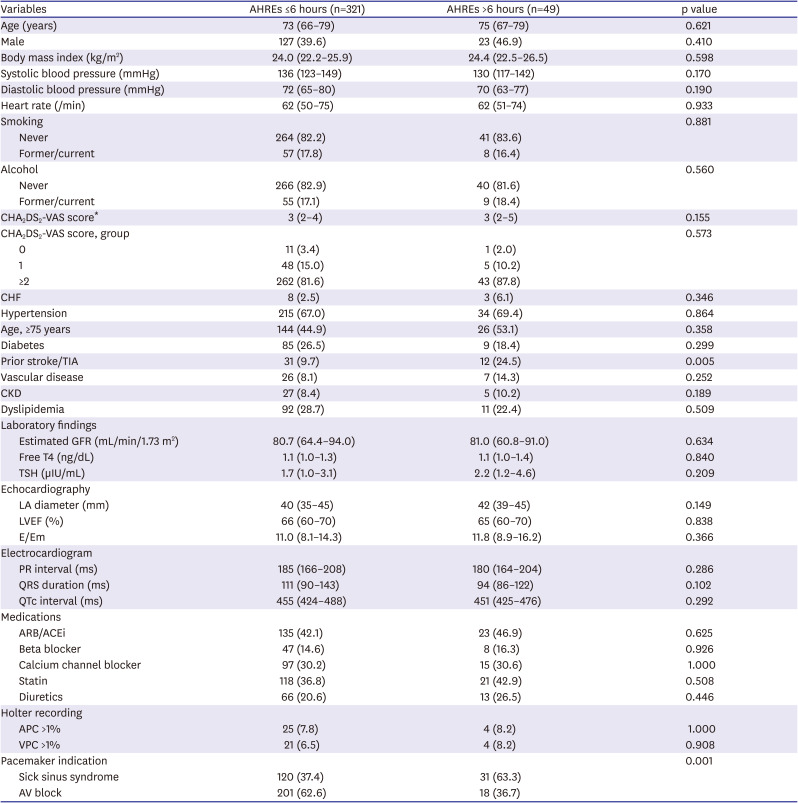
The data are presented as number (%) or median (interquartile interval). Non-parametric continuous variables, assessed using the Kolmogorov–Smirnov method, were analyzed using Mann-Whitney U tests.
ACEi = angiotensin-converting-enzyme inhibitor; AHREs = atrial high rate episodes; APC = atrial premature complex; ARB = angiotensin receptor blocker; AV = atrioventricular; BUN = blood urea nitrogen; CHF = congestive heart failure; CKD = chronic kidney disease; E/Em = the ratio of the early diastolic mitral inflow velocity (E) to the early diastolic mitral annular velocity (Em); GFR = glomerular filtration rate; LA = left atrium; LVEF = left ventricular ejection fraction; QTc = corrected QT; TIA = transient ischemic attack; TSH = thyroid-stimulating hormone; VPC = ventricular premature complex.
*The CHA2DS2-VAS score is a measure of the risk of stroke in patients with atrial fibrillation, with scoring ranging from 0 to 9 and higher scores indicating a greater risk. Congestive heart failure, hypertension, age 75 years or older (doubled), diabetes, stroke (doubled), vascular disease, age 65 to 74 years, sex category (female).
Predictors of longest AHREs duration >6 minutes
During the follow-up period, 112 of the 816 (13.7%) patients had AHREs with a longest duration >6 min. Univariate logistic regression analysis showed that LA diameter >41 mm (OR, 2.05; 95% CI, 1.29–3.28; p=0.003), APC >1% on Holter monitoring before CIEDs implantation (OR, 3.14; 95% CI, 1.46–6.78; p=0.004), and sick sinus syndrome for CIEDs implantation (OR, 3.85; 95% CI, 2.42–6.14; p<0.001) predicted a higher probability of longest AHREs duration >6 minutes. The sensitivity analysis of atrial pacing ratio rather than the diagnosis of sick sinus syndrome demonstrated consistent findings (Supplementary Table 2).
Multivariable logistic regression analysis demonstrated that LA diameter >41 mm (OR, 2.08; 95% CI, 1.25–3.45; p=0.005), and prior sick sinus syndrome (OR, 3.22; 95% CI, 1.91–5.43; p<0.001) were significantly associated with the probability of AHREs with a longest duration >6 minutes (Table 4). Comparison of AHREs with a longest duration cut-off of 6 hours showed that prior stroke/TIA (OR, 1.62; 95% CI, 1.08–2.43; p=0.021), LA diameter >41 mm (OR, 1.96; 95% CI, 1.00–3.85; p=0.050), and sick sinus syndrome for CIEDs implantation (OR, 2.52; 95% CI, 1.27-4.99; p=0.008) were independently associated with longest AHREs duration >6 hours (Table 5).
Table 4
Logistic regression analysis of factors associated with longest AHRE >6 min
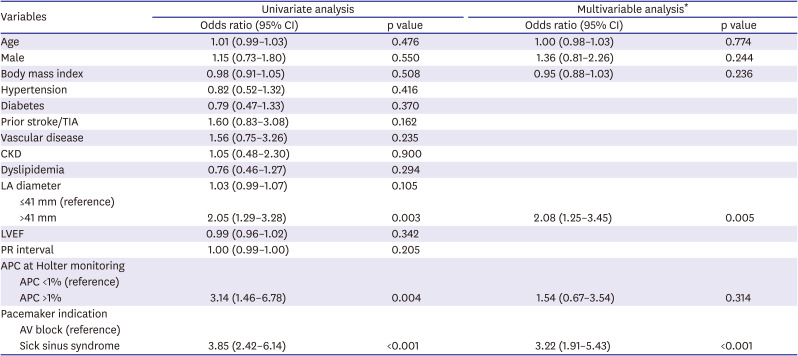
AHREs = atrial high rate episodes; APC = atrial premature contraction; AV = atrioventricular; CI = confidence interval; CKD = chronic kidney disease; ECG = electrocardiogram; LA = left atrium; LVEF = left ventricular ejection fraction; TIA = transient ischemic attack.
*Adjusted covariates include age, sex, body mass index, LA diameter >41 mm, APC >1% on Holter monitoring, pacemaker indication.
Table 5
Logistic regression of factors associated with AHREs (>6 hours)
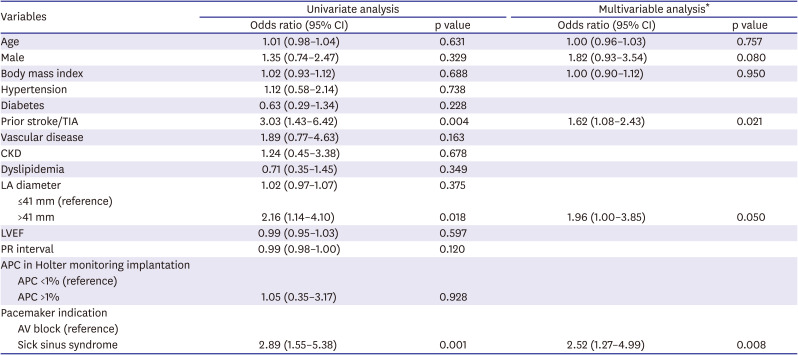
AHREs = atrial high rate episodes; APC = atrial premature contraction; AV = atrioventricular; CI = confidence interval; CKD = chronic kidney disease; ECG = electrocardiogram; LA = left atrium; LVEF = left ventricular ejection fraction; TIA = transient ischemic attack.
*Adjusted covariates include age, sex, body mass index, prior stroke/TIA, LA diameter >41 mm, pacemaker indication.
Associations between AHREs and clinical outcomes
Total of four CVA events were observed during the study period. The incidence rates (IRs, percent per person-year) of CVA, major/minor bleeding, MI, and all-cause death were 2.30%, 2.30%, 0%, and 0%, respectively, in patients with AHREs >6 minutes. For patients with AHREs ≤6 minutes, these IRs were 0.31%, 0.95%, 0.31%, and 0.31%, respectively. For the AHREs cut-off 6 hours, similar trends were observed (Supplementary Tables 3 and 4).
DISCUSSION
This study observed a substantial incidence in AHREs among patients 19 years of age or older with a history of sick sinus syndrome or atrioventricular node disease who had undergone pacemaker implantation and were free of clinical AF. AHREs with a longest duration >6 minutes were detected in 12.5% of patients within 6 months after implantation and were detected at least once during a median follow-up period of 18 months in 13.7% of patients. Episodes of subclinical atrial tachyarrhythmias were almost five times as common as episodes of clinical AF. During the course of the study, AHREs detection was confirmed in all clinical AF patients. Clinical AF developed in 21.4% (24/112) of patients with longest AHREs duration >6 minutes and 48.9% (24/49) of patients with longest AHREs duration >6 hours, suggesting that there can be a gap between subclinical events and clinical detection. Larger LA size (>41 mm) and sick sinus syndrome for CIEDs implantation were significant predictors of longest AHREs duration >6 minutes. By means of longest AHREs duration >6 hours, prior history of stroke or TIA, larger LA size (>41 mm), and sick sinus syndrome were significant predictors. However, we did not demonstrate a meaningful relationship between AHREs and clinical events including CVA, bleeding, MI, and all-cause death.
Most studies of patients with CIEDs have shown a high incidence of CIEDs-detected AHREs.1)3)4)6)8)9)11)18)19) A growing body of clinical data supports the hypothesis that AHREs are associated with an elevated risk of developing further clinical AF and stroke; however, the stroke risk is relatively lower than that in patients with clinical AF due to the short and rare nature of AHREs.14) Data from ASSERT trial1) showed that AHREs lasting more than 6 min in the first 3 months after CIED implantation were associated with a 5.6-fold increased hazard of clinical AF during a mean 2.5-year follow-up. Similar results were reported in the MOST trial,3) in which AHREs lasting at least 5 minutes were associated with a 5.9-fold increased hazard of clinical AF during median 2.3-year follow-up. Clinical atrial tachyarrhythmias on surface ECG occurred in 25.7% of patients in the MOST trial, 15.8% of patients in the ASSERT trial, and 28.9% of patients in the ASSERT II trial, which investigated patients ≥65 years of age.1)3)20) In subsets of ASSERT patients, older age, higher BMI, and longer AHRE episodes were associated with AF progression.21) In our study, 21.4% and 48.9% of patients with AHREs >6 minutes and >6 hours were confirmed to have clinically documented AF during follow-up. As the number of patients was small, we could not proceed with further analysis. Although AHREs are more likely to allow detection of ECG-documented AF, about 80% of patients with AHREs >6 minutes never develop ECG-documented AF in the subsequent years, probably due to the infrequent and short nature of AHREs in most patients and missing link that we have not proven yet.
We detected four CVA events during the median 18-month follow-up. Our findings did not demonstrate an increased risk of CVA in patients with CIEDs developing AHREs. However, a meta-analysis of seven studies22) showed that AHREs were associated with a 2.4-fold increased risk of stroke. Although the definitions of AHREs duration varied significantly between studies, subsequent stratified analyses showed that most events occurred in patients with >24-hours AHREs.23) Therefore, the predominant evidence suggests a dose-response relationship between longest AHREs duration and stroke risk. Long-term follow-up is necessary to determine the relationship between AHREs and stroke risk in this registry.
The increased risk associated with developing AHREs may be similar to that for AF, reinforcing the concept that AHREs and AF are likely to represent a clinical continuum in the spectrum of atrial tachyarrhythmias. Some predictors for AHREs have been identified in patients with CIEDs. In the ASSERT trial,1) sinus node dysfunction and decreased resting heart rate were associated with the prediction of AHREs. Gonzales et al.9) reported that previous HF predicted AHREs, while Cheung et al.24) found that sinus node disease and a higher proportion of ventricular pacing were associated with AHREs. A meta-analysis of 28 dual-chamber device studies showed that the clinical variables related to AF including increasing age, HTN, DM, CAD, embolic events, and CHADS2 were not associated with the prediction of AHREs. In our study, the independent predictors of AHREs with longest duration >6 minutes were larger LA size (>41 mm), and sick sinus syndrome before CIED implantation. Between patients who developed AHREs and those who did not, an LA size of 41 mm was a useful threshold to identify patients who would develop AHREs. Although total APC >1% on Holter monitoring showed predictive value for AHREs development in univariate analysis, this variable was not associated in the multivariate analysis. Prior stroke/TIA, LA diameter >41 mm, and sick sinus syndrome were the predictors for longest AHREs duration >6 hours. These differences may be explained in part by differences in the definitions of AHREs duration. Therefore, our data indicate new predictors including prior stroke/TIA and LA diameter >41 mm before CIEDs implantation.
This study has several limitations. First, although this was a prospective and multicenter study, the study design was non-randomized and observational. The study duration was relatively short compared to that in previous studies, the enrolled population was small, and additional potential confounding factors may have significantly affected the results. Second, the study population was limited to patients with pacemakers with generally normal LV systolic function. Therefore, the results cannot be directly applied to implantable cardioverter-defibrillator or cardiac resynchronization therapy populations, whose prevalence of CIEDs-detected AF may be higher. Third, although AHREs lasting >6 hours can improve the positive predictive value,11) current guidelines12) consider AHREs lasting >5 minutes as clinically relevant, and the majority of studies3)6)7)8)9)10)used an episode duration of AHRE longer than 5–6 minutes. Therefore, it may be reasonable to analyze the results based on AHREs lasting >6 minutes. Finally, very few clinical events were observed during the follow-up period, including four cases of stroke. Patients are being enrolled and the follow-up period is relatively short; therefore, analysis of long-term data is required.
AHREs occurred frequently in patients with pacemakers who had a history of prior stroke/TIA, LA diameter >41 mm, and sick sinus syndrome before CIEDs implantation but no prior diagnosis of clinical AF. However, there was a lack of data regarding whether AHREs increased the stroke risk. More long-term follow-up data are required to determine the clinical impact of AHREs.
 XML Download
XML Download