

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
With the advancement of devices and technology in the field of percutaneous coronary intervention (PCI), its application has expanded into more complex lesions than before.1) However, the benefit of PCI in terms of hard endpoints in stable coronary artery disease is still under debate,2) and the recent ISCHEMIA trial could not demonstrate the benefits of ischemia-guided PCI in terms of ischemic cardiovascular events or all-cause death.3) Therefore, appropriate selection of target lesions and procedural optimization are still required to improve the outcomes after PCI.
The evidence of myocardial ischemia is a prerequisite for the benefit of coronary revascularization.4) Fractional flow reserve (FFR) has been a standard invasive method to define the ischemia-causing coronary stenosis.5) Non-hyperemic pressure ratios (NHPR) were recently developed and expanded the clinical application of coronary physiology in daily practice.6)7)8)9)10)11) However, the application of coronary physiologic assessment is much less used after stent implantation than before PCI despite accumulating data on the prognostic value of post-PCI physiologic assessment.12)13)14) The current review will cover previous data, current status, and the future perspectives of physiologic assessment after PCI.
WHY POST-PERCUTANEOUS CORONARY INTERVENTION PHYSIOLOGIC ASSESSMENT?
For decades, PCI results have been assessed based on coronary angiography with varying definitions of complete revascularization.15)16)17)18) However, coronary angiography provides only the 2-dimensional silhouette of the coronary lumen and has several limitations in determining the success of PCI. From the intracoronary imaging studies using intravascular ultrasound (IVUS) or optical coherence tomography (OCT), a substantial proportion of stented segments showed suboptimal PCI results, such as stent underexpansion, malapposition, edge dissection, or plaque protrusion19)20)21)22)23) which might lead to worse clinical outcomes after PCI.20)22) Even though coronary imaging can reveal these hidden problems after PCI, the images cannot judge whether there is remaining myocardial ischemia caused by suboptimal PCI or residual disease outside the stents. Given that up to one-fourth of patients may have physiologically unsuccessful PCI, as well as the association between post-PCI physiologic status and clinical outcomes, physiologic assessment after PCI may be an essential step for PCI optimization.24)25)26)
There can be several causes for physiologically suboptimal PCI results, such as stent underexpansion, incomplete lesion coverage, significant residual disease, and edge dissection.27) Hanekamp et al.28) demonstrated that stent malapposition, stent symmetricity, and in-stent cross-sectional area assessed by IVUS were highly correlated with post-PCI FFR. Ito et al.29) reported the inverse correlation between post-PCI FFR and residual peri-stent plaque volume index (r=−0.40, p<0.01) and residual peri-stent percent plaque volume (r=−0.68, p<0.01) in IVUS. From the OCT study, Wolfrum et al.27) demonstrated that suboptimal functional results (post-PCI FFR <0.90) were found in 60% of patients after conventional angiography guided-PCI, and among them, 61.9% of patients were associated with stent underexpansion or incomplete lesion coverage found from OCT. In cases of optimal stent implantation, inadequate results in the post-stent physiologic assessment are mainly due to the residual disease burden outside the stented segments (Figure 1).
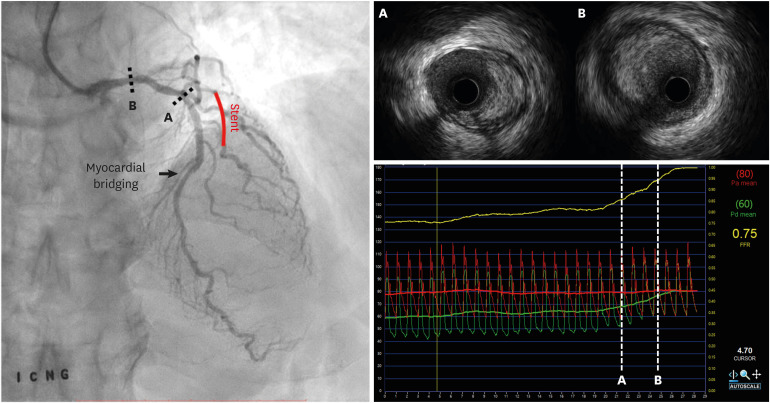
Figure 1
A case with residual ischemia after angiographically successful stent implantation. Fractional flow reserve measured after stent implantation at the distal LAD was 0.75. Pressure wire pullback under hyperemia showed a pressure step up at the proximal LAD, and there was no significant pressure change across the stented segment. Intravascular ultrasound showed diffuse atherosclerotic disease at the left main coronary artery and proximal LAD.
LAD = left anterior descending artery.
CLINICAL DATA ON THE POST-PERCUTANEOUS CORONARY INTERVENTION PHYSIOLOGIC ASSESSMENT
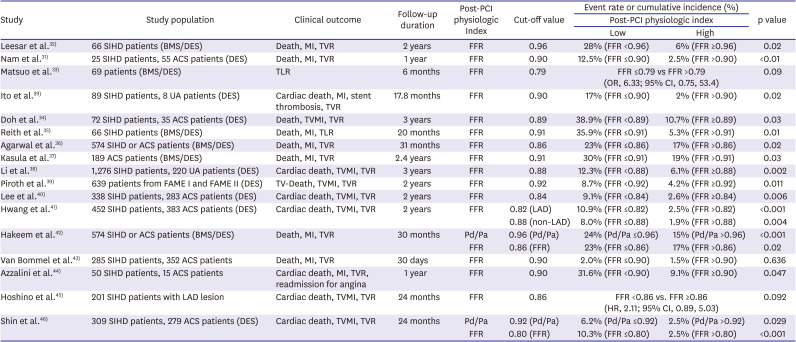
Since Bech et al.30) reported the prognostic value of FFR after balloon angioplasty, many studies, including meta-analyses, demonstrated the association between post-PCI FFR and clinical outcomes after bare-metal stent (BMS) or drug-eluting stent (DES) implantation (Table 1).29)31)32)33)34)35)36)37)38)39)40)41)42)43)44)45)46) Pijls et al.47) reported that post-PCI FFR after BMS implantation was an independent predictor of clinical events at 6 months. Along with the introduction of DES, the prognostic value of post-PCI FFR was validated in various studies with consistent results. Nam et al.31) evaluated 80 patients after PCI with DES and showed that the rates of major adverse cardiac events (MACE) at 1 year were 12.5% in patients with post-PCI FFR below 0.90 and 2.5% in patients with post-PCI FFR over 0.90 (p value<0.01). Another study from Doh et al.34) reported post-PCI FFR 0.89 as a cut-off value for predicting target vessel failure (TVF) at 1 year and demonstrated lesions with post-PCI FFR over 0.89 had a better TVF-free survival rate than those with post-PCI FFR below 0.89 at 3 years (89.3% vs. 61.1%, p value=0.03). The DK-CRUSH VII study by Li et al.38) evaluated 1,476 patients undergoing DES implantation and suggested post-PCI FFR of 0.88 as a cut-off value for predicting TVF at 1 year and 3 years. The study-level meta-analysis by Rimac et al.14) evaluated 7,470 patients from 105 studies, and meta-regression analysis showed the inverse relationship between post-PCI FFR and the rates of repeat revascularization (p value<0.0001) and MACE (p value=0.0013). This study reported post-PCI FFR of 0.90 as a cut-off value for predicting repeat revascularization and MACE.
Table 1
Clinical data for post-PCI physiologic assessment after DES implantation
| Study | Study population | Clinical outcome | Follow-up duration | Post-PCI physiologic Index | Cut-off value | Event rate or cumulative incidence (%) | p value | |
|---|---|---|---|---|---|---|---|---|
| Post-PCI physiologic index | ||||||||
| Low | High | |||||||
| Leesar et al.32) | 66 SIHD patients (BMS/DES) | Death, MI, TVR | 2 years | FFR | 0.96 | 28% (FFR <0.96) | 6% (FFR ≥0.96) | 0.02 |
| Nam et al.31) | 25 SIHD patients, 55 ACS patients (DES) | Death, MI, TVR | 1 year | FFR | 0.90 | 12.5% (FFR ≤0.90) | 2.5% (FFR >0.90) | <0.01 |
| Matsuo et al.33) | 69 patients (BMS/DES) | TLR | 6 months | FFR | 0.79 | FFR ≤0.79 vs FFR >0.79 (OR, 6.33; 95% CI, 0.75, 53.4) | 0.09 | |
| Ito et al.29) | 89 SIHD patients, 8 UA patients (DES) | Cardiac death, MI, stent thrombosis, TVR | 17.8 months | FFR | 0.90 | 17% (FFR ≤0.90) | 2% (FFR >0.90) | 0.02 |
| Doh et al.34) | 72 SIHD patients, 35 ACS patients (DES) | Death, TVMI, TVR | 3 years | FFR | 0.89 | 38.9% (FFR <0.89) | 10.7% (FFR ≥0.89) | 0.03 |
| Reith et al.35) | 66 SIHD patients (BMS/DES) | Death, MI, TLR | 20 months | FFR | 0.91 | 35.9% (FFR ≤0.91) | 5.3% (FFR >0.91) | 0.01 |
| Agarwal et al.36) | 574 SIHD or ACS patients (BMS/DES) | Death, MI, TVR | 31 months | FFR | 0.86 | 23% (FFR ≤0.86) | 17% (FFR >0.86) | 0.02 |
| Kasula et al.37) | 189 ACS patients (BMS/DES) | Death, MI, TVR | 2.4 years | FFR | 0.91 | 30% (FFR ≤0.91) | 19% (FFR >0.91) | 0.03 |
| Li et al.38) | 1,276 SIHD patients, 220 UA patients (DES) | Cardiac death, TVMI, TVR | 3 years | FFR | 0.88 | 12.3% (FFR <0.88) | 6.1% (FFR ≥0.88) | 0.002 |
| Piroth et al.39) | 639 patients from FAME I and FAME II (DES) | TV-Death, TVMI, TVR | 2 years | FFR | 0.92 | 8.7% (FFR <0.92) | 4.2% (FFR ≥0.92) | 0.011 |
| Lee et al.40) | 338 SIHD patients, 283 ACS patients (DES) | Cardiac death, TVMI, TVR | 2 years | FFR | 0.84 | 9.1% (FFR <0.84) | 2.6% (FFR ≥0.84) | 0.006 |
| Hwang et al.41) | 452 SIHD patients, 383 ACS patients (DES) | Cardiac death, TVMI, TVR | 2 years | FFR | 0.82 (LAD) | 10.9% (FFR ≤0.82) | 2.5% (FFR >0.82) | <0.001 |
| 0.88 (non-LAD) | 8.0% (FFR ≤0.88) | 1.9% (FFR >0.88) | 0.004 | |||||
| Hakeem et al.42) | 574 SIHD or ACS patients (BMS/DES) | Death, MI, TVR | 30 months | Pd/Pa | 0.96 (Pd/Pa) | 24% (Pd/Pa ≤0.96) | 15% (Pd/Pa >0.96) | <0.001 |
| FFR | 0.86 (FFR) | 23% (FFR ≤0.86) | 17% (FFR >0.86) | 0.02 | ||||
| Van Bommel et al.43) | 285 SIHD patients, 352 ACS patients | Death, MI, TVR | 30 days | FFR | 0.90 | 2.0% (FFR ≤0.90) | 1.5% (FFR >0.90) | 0.636 |
| Azzalini et al.44) | 50 SIHD patients, 15 ACS patients | Cardiac death, MI, TVR, readmission for angina | 1 year | FFR | 0.90 | 31.6% (FFR <0.90) | 9.1% (FFR ≥0.90) | 0.047 |
| Hoshino et al.45) | 201 SIHD patients with LAD lesion | Cardiac death, TVMI, TVR | 24 months | FFR | 0.86 | FFR <0.86 vs. FFR ≥0.86 (HR, 2.11; 95% CI, 0.89, 5.03) | 0.092 | |
| Shin et al.46) | 309 SIHD patients, 279 ACS patients (DES) | Cardiac death, TVMI, TVR | 24 months | Pd/Pa | 0.92 (Pd/Pa) | 6.2% (Pd/Pa ≤0.92) | 2.5% (Pd/Pa >0.92) | 0.029 |
| FFR | 0.80 (FFR) | 10.3% (FFR ≤0.80) | 2.5% (FFR >0.80) | <0.001 | ||||
ACS = acute coronary syndrome; BMS = bare-metal stent; CI = confidence interval; DES = drug-eluting stent; FFR = fractional flow reserve; HR = hazard ratio; LAD = left anterior descending artery; MI = myocardial infarction; OR = odds ratio; PCI = percutaneous coronary intervention; SIHD = stable ischemic heart disease; TLR = target lesion revascularization; TVMI = target-vessel myocardial infarction; TVR = target vessel revascularization.
Previous studies consistently demonstrated the prognostic value of post-PCI FFR. However, various cut-off values were proposed for the decision of additional procedures, and some studies raised the concern regarding the low predictive value of post-PCI FFR as a surrogate marker of clinical outcome.33)39) Piroth et al.39) evaluated 639 patients from FAME 1 and FAME 2 studies and insisted that a discrete post-PCI FFR value could not be used due to the low likelihood ratio (<1.4) to predict the risk for clinical events. In contrast, a recent study showed that post-PCI FFR is still a crucial element for patient outcomes (Figure 2). From the International Post-PCI FFR registry (2,200 patients), Hwang et al.12) developed a risk model incorporating clinical, angiographic, and post-PCI FFR data (Figure 3). They found that total stent length and post-PCI FFR were the most important factors for TVF at 2 years, and there was incremental predictability by incorporating clinical, angiographic, and post-PCI FFR data for the risk model construction.
Figure 2
Rate of TVF according to post-PCI FFR. The rates of TVF at 2 years decreased along with the increase of post-PCI FFR from the International Post-PCI FFR registry.
FFR = fractional flow reserve; PCI = percutaneous coronary intervention; TVF = target vessel failure.

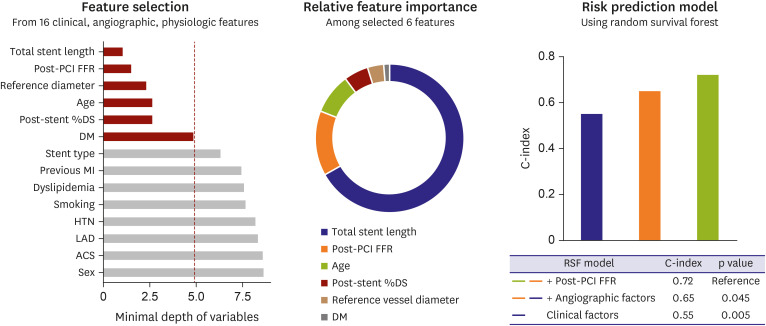
Figure 3
Risk prediction model based on machine learning after coronary stenting. From the International Post-PCI FFR registry, the risk prediction model after coronary stenting was developed using a machine learning technique by incorporating clinical, angiographic, and post-PCI FFR data. Six important features were identified, and total stent length and post-PCI FFR were the most important features for predicting target vessel failure at 2 years. Post-PCI FFR had an additive value for risk prediction in addition to clinical and angiographic data.
ACS = acute coronary syndrome; C-index = concordance index; DS = diameter stenosis; DM = diabetes mellitus; FFR = fractional flow reserve; HTN = hypertension; LAD = left anterior descending artery; MI = myocardial infarction; PCI = percutaneous coronary intervention.
Along with the recent introduction of NHPR, several studies investigated the clinical and prognostic implications of NHPR after stent implantation. From the DEFINE PCI study, Jeremias et al.48) reported that one-fourth of the patients with angiographically successful PCI showed residual ischemia by assessing the instantaneous wave-free ratio (iFR). Among them, 81.6% of patients had untreated focal disease with the potential to improve post-PCI iFR by additional PCI. Shin et al.46) and Hakeem et al.42) showed that post-PCI resting Pd/Pa had incremental prognostic value over post-PCI FFR. These study results support the use of NHPR after stent implantation. However, while applying NHPR after stent implantation, the operators need to recognize that NHPR requires true resting status for its measurement. Pain, anxiety, or peri-procedural myocardial injury associated with PCI can cause false-positive results in the post-PCI physiologic assessment with NHPR.
PHYSIOLOGIC PERSPECTIVES OF POST PERCUTANEOUS CORONARY INTERVENTION FRACTIONAL FLOW RESERVE OR NON-HYPEREMIC PRESSURE RATIOS
Post-PCI physiology is determined by complex interactions of the stented segment and residual disease in non-stented segments, subtending myocardial mass, and microvascular function. Therefore, the implications of post-PCI physiologic assessment cannot be fully represented by one measured number of physiologic index. Lee et al.40) introduced the concept of percent FFR increase, which can be calculated as (post-PCI FFR − pre-PCI FFR)/pre-PCI FFR × 100. They demonstrated that more than 15% of percent FFR increase was associated with a lower risk of TVF at 2 years (hazard ratio, 4.33; 95% confidence interval [CI], 1.21, 15.59) and had additive prognostic value over post-PCI FFR.40) Another study by Hamaya et al.49) evaluated the importance of pre-PCI FFR in association with post-PCI FFR using mediation analysis. They evaluated a total of 1,488 patients with available pre-and post-PCI FFR data and demonstrated that there were both direct and indirect effects of pre-PCI FFR on TVF at 2 years. These studies support the importance of baseline physiologic status on clinical outcomes, even after stent implantation, and suggest that comprehensive clinical and physiologic assessment of both pre-and post-PCI status can more appropriately assess patient and lesion risk after PCI.
Subtending myocardial mass also influences the value of post-PCI physiologic assessment as pressure-derived physiologic indices are affected not only by disease severity but also by the amount of coronary flow or subtending myocardium.50) Hwang et al.41) investigated the prognostic relevance of post-PCI FFR according to the target vessel location. They evaluated 603 lesions in left anterior descending artery (LAD) and 232 lesions in non-LAD. The distributions and optimal cut-off values for post-PCI FFR were different in LADs and non-LADs, and different cut-off values (0.82 for LAD and 0.88 for non-LAD) could better differentiate the risk for TVF than a single value. This result showed that the effect of target vessel location on post-PCI FFR is one of the reasons for various cut-off values reported from previous studies, and applying different cut-off values according to the target vessel might be needed.
For the association with microvascular dysfunction, Murai et al.51) evaluated the association between post-PCI FFR and the presence of microvascular dysfunction. From the evaluation of 104 vessels, they demonstrated that coronary flow decreased, and post-PCI FFR increased along with the increase of the index of microcirculatory resistance. Underlying severe microvascular dysfunction or myocardial injury during PCI can cause underestimation of residual disease after PCI when assessed by physiologic indices based on coronary pressure.
In summary, the above findings suggest that the operators need to acknowledge the influence of complex interactions among disease burden in stented and non-stented segments, pre-existing disease burden, subtending myocardium, and microvascular dysfunction on post-PCI physiology to understand the value of physiologic index adequately, and then select the appropriate assessment and treatment strategies accordingly.
HOW TO MANAGE CASES WITH THE LOW VALUE OF THE POST-PERCUTANEOUS CORONARY INTERVENTION PHYSIOLOGIC INDEX
In clinical practice, we frequently encounter patients with low-post PCI physiologic index, even after angiographically successful PCI.36)48) Agarwal et al.36) demonstrated that additional intervention for patients with suboptimal PCI improved post-PCI FFR value from 0.78±0.07 to 0.87±0.05, and Jeremias et al.48) reported that about 80% of lesions that had suboptimal post-PCI iFR values had untreated focal stenoses potentially amenable to PCI. However, a step-by-step approach for detailed physiologic investigations followed by physiology-guided treatment decision is mandatory for patients with angiographically successful but physiologically suboptimal PCI results (Figure 4).
Figure 4
PCI optimization strategy with post-PCI physiologic assessment.
FFR = fractional flow reserve; NHPR = non-hyperemic pressure ratio; PCI = percutaneous coronary intervention.

The first and most crucial step in the physiologic assessment is to perform a meticulous pressure wire pullback, either under maximal hyperemia or at rest for FFR or NHPR, respectively. The presence of drift and subsequent falsely low value should be checked before any additional procedures for the low value of the physiologic index. If the drift is found, the pressures between the wire and aorta should be re-equalized, and FFR or NHPR should be measured again. After excluding drift, the pullback pressure curve can reveal the culprit segment for a significant pressure drop. A recent technology that can co-register the angiogram and the pullback tracing of iFR can make this process easier and more straightforward. If the significant pressure step-up occurs in the stented segment, additional coronary imaging might help to define the causes of suboptimal PCI such as stent underexpansion, edge dissection, or significant uncovered plaque around the stented segment. Recent studies showed that the cause of physiologically suboptimal PCI occurs in the non-stented segments in 70–80%.43)48)52) If the pressure drop is mainly due to residual disease in the non-stented segment, a further treatment plan should be made based on the physiologic pattern of residual disease. The focal disease can be treated with additional stent implantation. However, additional PCI for the physiologically diffuse disease does not warrant the additional benefit and can be harmful.
PREDICTION OF POST-PERCUTANEOUS CORONARY INTERVENTION PHYSIOLOGY WITH NOVEL TECHNIQUES
As the post-PCI physiologic status is an important prognostic indicator, its prediction before PCI can help select the proper treatment strategy and prevent unnecessary PCI. In the catheterization laboratory, this can be estimated from physiologic assessment before PCI. Kikuta et al.53) demonstrated that iFR pullback tracing before PCI could predict post-PCI iFR well with 1.4±0.5% error. Recently, automatic co-registration of iFR pullback tracing with coronary angiogram was introduced and provided an intuitive method to decide and plan coronary revascularization.54)55) In addition to iFR pullback, Omori et al.56) evaluated the ability of pre-PCI NHPR pullbacks in predicting post-PCI results. They demonstrated that predicted post-PCI resting full-cycle ratio (RFR) and diastolic pressure ratio (dPR) from pullback pressure tracings before PCI also highly correlated with actual RFR (r=0.84, p<0.001) and dPR (r=0.84, p<0.001) like iFR (r=0.83, p<0.001) measured after PCI.56)
Even though FFR has some disadvantages in predicting post-PCI physiologic status, recent studies proposed novel methods to define the pathophysiological pattern of coronary artery disease and predict the post-PCI FFR. Völz et al.57) studied motorized FFR pullback curves and developed a concept of the pullback pressure gradient (PPG) index, which can depict the magnitude of FFR drop and the length of diseased coronary artery segments. The study demonstrated that coronary angiography could not sufficiently define the pattern of coronary artery disease, and motorized FFR pullbacks reclassified 36% of the disease pattern with increasing the interobserver agreement. Lee et al.58) developed an automated algorithm that analyzes the instantaneous FFR gradient per unit time (dFFR(t)/dt).dFFR(t)/dt showed significant correlations with percent FFR increase and post-PCI FFR. This result suggests that this algorithm can be applied to predict patients with suboptimal post-PCI physiologic status.
Recently, with the advances in computational science, the clinical application of computational fluid dynamics or mathematical assumptions has enabled the estimation of coronary physiologic status using coronary anatomy from imaging modalities. The first innovation was coronary computed tomography-based computation of FFR (CT-FFR).59)60)61)62)63) Based on these technologies, recent studies focused on how to plan a treatment strategy and how to expect the outcome of revascularization using the so-called virtual PCI concept. Kim et al.64) first introduced the possibility of CT-FFR for treatment planning. In their study, CT-FFR values before and after PCI were highly correlated with invasive FFR values, and the mean difference between FFR and CT-FFR was 0.006 (95% CI, −0.27, 0.28) before PCI and 0.024 (95% CI, −0.08, 0.13) after PCI. The results were also reproduced in a recent study.65) Quantitative flow ratio (QFR) is a 3-dimensional QCA-based computation of FFR, and previous studies have reported excellent correlations and diagnostic agreements with FFR.66) Recently, several studies investigated the prognostic value of post-PCI QFR.52)67) Furthermore, there is an effort to estimate post-PCI FFR using pre-PCI coronary angiograms. From the DOCTORS study population, Rubimbura et al.68) analyzed the residual QFR and found that residual QFR was similar to post-PCI FFR (residual QFR 0.92±0.05 vs. post-PCI FFR 0.93±0.05, p value>0.05). Another study from Dai et al.69) reported the feasibility of the PPG index from QFR virtual pullback curves in stratifying the disease patterns.
All of these efforts focused on how to predict the post-PCI physiologic status, both invasively and non-invasively (Figure 5). Applying these novel technologies in daily practice will help select the patients who will achieve maximal benefit with PCI and improve overall PCI outcomes.

CONCLUSION
Post-PCI coronary physiologic status is one of the key prognostic factors for patients undergoing PCI. Physiologic assessment after PCI can reveal the residual disease that needs additional procedures and enables better risk stratification than angiographic assessment. Therefore, greater adoption of post-PCI physiologic assessment can improve patient outcomes after stent implantation and maximize the benefit of PCI. In addition, novel technologies to predict the post-PCI physiology before PCI will help physicians select the appropriate treatment strategy. Now is the time for all interventional cardiologists to remember what American baseball legend Yogi Berra said in 1973: “It ain't over, till it's over.”
 XML Download
XML Download