

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Although surgical aortic valve replacement (AVR) has been accepted as the “gold standard” for the treatment of aortic valve (AV) disease since the last 50 years, advanced technology such as transcatheter aortic valve replacement (TAVR) has evolved rapidly, and its indication has been extended from patients at a high risk for conventional aortic valve replacement (CAVR) to patients at an intermediate risk. More recently, its role in low-risk patients is being investigated.123
Recent emergence of sutureless aortic valve replacement (SAVR) technology provides an alternative option that can overcome the limitations of both TAVR and CAVR. Its theoretical advantages include 1) short duration of aortic cross clamp (ACC) and cardiopulmonary bypass (CPB) by avoiding suture placement and tying the knots, 2) ease of implantation even in limited surgical fields, and 3) favorable hemodynamic properties.456 It is also expected that the SAVR could improve clinical outcomes after surgery because prolonged ACC and CPB times are associated with increased morbidity and mortality.789 Despite these advantages of SAVR, there are concerns regarding the high rate of permanent pacemaker (PPM) implantation and paravalvular leakage.410
Although, there has been many studies including European registry data, there has been no data regarding results of SAVR in Korea. Therefore, this study was conducted to evaluate the early and two-year outcomes after SAVR and to compare these outcomes with the results after CAVR, from the National Health Information Database of Korea.
METHODS
Data source and patient characteristics
Data for the present study was obtained based on the claims database from the Korean National Health Insurance Service (NIHS), which is a single insurer managed by the government, covering the entire Korean population. The NIHS provides healthcare insurance coverage to the vast majority (> 97%) of residents in Korea.1112 This database comprises a complete set of medical claims and health information, including demographic data (age, sex, and resident registration number), procedure and diagnosis codes, and survival information for inpatient and outpatient services. Diagnoses are coded on the basis of the International Classification of Diseases, 10th Revision, Clinical Modification.12
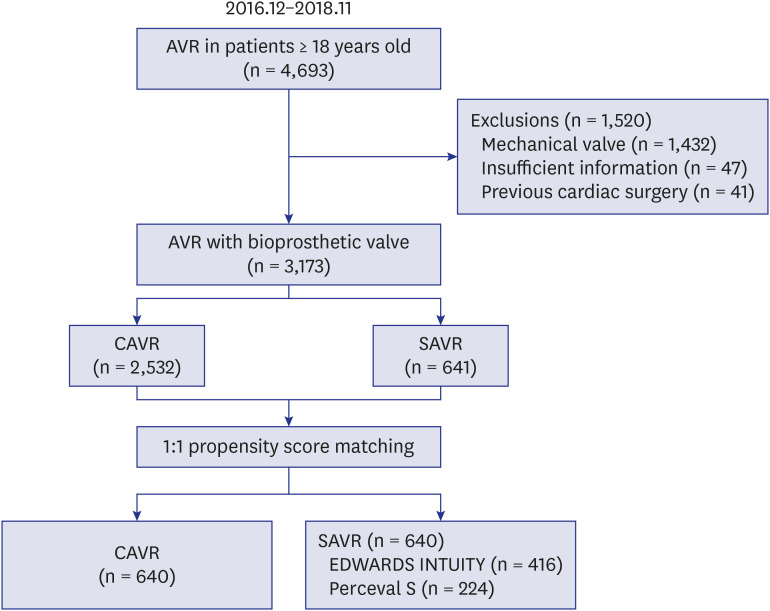
From December 2016, when SAVR was approved for insurance coverage, to November 2018, 4,689 adult patients (≥ 18 years old) who underwent AVR using conventional prosthetic valves or sutureless aortic prostheses were identified based on the procedure codes of Korea NIHS (O1793, aortic valve replacement; O1799, sutureless aortic valve replacement) and product codes for prosthetic aortic valves available in Korea. After excluding 1,432 patients with mechanical AVR, 41 patients with a history of cardiac surgery, and 47 patients with inadequate claims data pertaining to age and sex, 3,173 patients were enrolled in the present study. Conventional and sutureless AVRs were performed in 2,532 and 641 patients, respectively. In the SAVR group, EDWARDS INTUITY (Edwards Lifesciences, Irvine, CA, USA) and Perceval S (LivaNova PLC, London, UK) valves were used in 417 (65.1%) and 224 (34.9%) patients, respectively (Fig. 1).
Preoperative comorbidities were evaluated using the diagnosis codes within 1 year before the surgery (Supplementary Table 1). The Charlson comorbidity index was calculated using the diagnosis codes.13 The institutions were categorized into three groups based on the volumes of cases of surgical AVR per year (low, < 25 cases; medium, 25–100 cases; high, > 100 cases).
Evaluation of early and follow-up clinical outcomes
Operative mortality was defined as any death within 30 days after index admission. Postoperative acute renal failure (ARF) was defined as the administration of continuous renal replacement therapy or dialysis during the index hospitalization without any prior history of dialysis. Prosthetic valve endocarditis (PVE) was considered if the patient was newly diagnosed with infective endocarditis at least 3 months after index admission. Stroke was considered if the patients were newly diagnosed with stroke during the index hospitalization without any previous history of stroke or if the patients were rehospitalized with a diagnosis of stroke during follow-up. Data regarding overall survival (OS) and death from cardiovascular causes were obtained from the death certificates in Statistics Korea.
Clinical follow-up was closed on December 31, 2018. The median follow-up duration was 11.2 months (interquartile, 5.7–18.2 months).
Statistical analysis
Statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, NC, USA). Data were expressed as mean ± standard deviation, medians with ranges or proportions. Propensity score-matched analysis was performed to adjust for the differences in preoperative characteristics between the two groups. Propensity scores for being in a SAVR group were estimated using a multiple logistic regression model that included twenty preoperative and operative characteristics as described in Table 1. After calculating the propensity scores, 640 pairs of patients were matched using a nearest neighborhood (greedy matching) within a caliper width of 0.1 in propensity scores and with a ratio of 1:1. The balance of covariates between the groups were evaluated with standardized mean difference (SMD). SMD of less than 0.1 was considered as negligible difference between the groups. Before matching, comparisons between the two groups were performed using the χ2 test or Fisher's exact test for categorical variables and Student's t-test for continuous variables. Survival rates were estimated using the Kaplan-Meier method and were compared using the log-rank test. In the matched groups, the McNemar test and paired t-test were used for categorical and continuous variables, respectively, and survival rates were analyzed using the Cox proportional hazard model approach with robust sandwich covariance matrix estimates to account for the intracluster correlation. Cumulative incidences of cardiac death and the other clinical events were estimated considering non-cardiac death and any death, respectively, as a competing risk. Gray's test was used to test the equality of cumulative incidence between the groups in both all patients and matched data.14 If the follow-up clinical outcomes were significantly different between groups, landmark analyses were performed to minimize bias by including events that occurred in the early postoperative period. Subgroup analyses were performed to compare clinical outcomes between the EDWARDS INTUITY and Perceval S groups using χ2 test and Kaplan-Meier method. P value < 0.05 was considered statistically significant.
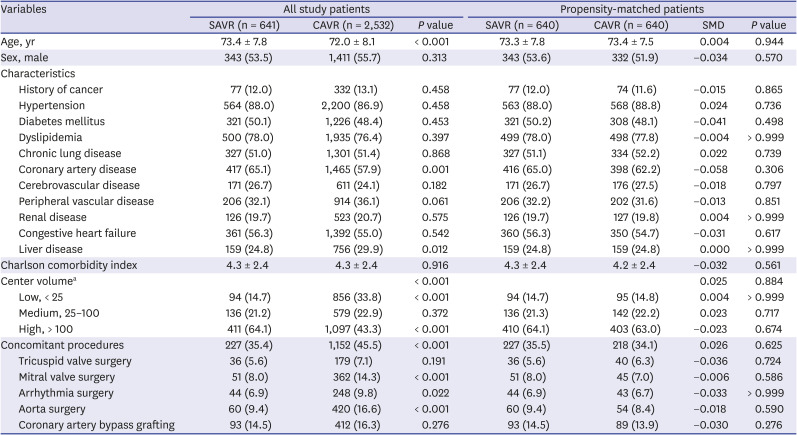
Table 1
Preoperative and operative characteristics of the study patients
Values are presented as mean ± standard deviation or number (%).
CAVR = conventional aortic valve replacement, SAVR = sutureless aortic valve replacement, SMD = standardized mean difference.
aAnnual number of surgical aortic valve replacement cases.
![]()
RESULTS
Preoperative characteristics
The preoperative characteristics are summarized in Table 1. There were significant differences in age, institutional surgical volume, and concomitant surgery between the SAVR and CAVR groups. Concomitant procedures were less frequently performed in the SAVR than in the CAVR group (35.4% vs. 45.5%, P < 0.001), and 64.1% of SAVR procedures were performed in the high volume centers whereas 43.3% of CAVR procedures were performed in these centers. There were no differences in the preoperative and operative characteristics between the two groups after matching.
Early clinical outcomes
The operative mortality rate was 3.9% (122 out of 3,173 patients) in the entire patient chohort. There was no significant differences in operative mortality between the SAVR and CAVR groups (3.4% vs. 4.0%, P = 0.486). Postoperative complications included ARF (n = 159, 5.0%), bleeding reoperation (n = 158, 5.0%), stroke (n = 67, 2.1%), PPM implantation (n = 50, 1.6%) and AV reoperation (n = 9, 0.3%). There were no significant differences in the rates of ARF, bleeding reoperation, stroke and AV reoperation between the two groups. However, the rate of PPM implantation was significantly higher in the SAVR group than in the CAVR group (3.9% vs. 1.0%, P < 0.001). The length of hospital stay (LOS) was shorter in the SAVR group than in the CAVR group (18.8 ± 11.9 days vs. 19.9 ± 12.6 days, P = 0.045).
After matching, there were no significant differences in operative mortality, postoperative complication rates, and LOS between the 2 groups, except a higher rate of PPM implantation in the SAVR than in the CAVR group (3.8% vs. 0.9%, P = 0.001) (Table 2).

Table 2
Early clinical outcomes of CAVR and SAVR
Values are presented as mean ± standard deviation or number (%).
CAVR = conventional aortic valve replacement, SAVR = sutureless aortic valve replacement.
![]()
Survival rates during the follow-up
Major events after CAVR and SAVR during the Follow-up were summarized in Table 3. Late death occurred in 206 patients including 173 cardiac deaths. One- and two-year OS rates were 89.1% and 87.5%, respectively. There were no significant differences in the one- and two-year OS rates between the 2 groups (SAVR group vs. CAVR group = 89.1% and 87.5% vs. 89.9% and 87.2%, respectively; P = 0.759). The cumulative incidences of cardiac death at one and two years were 5.7% and 6.0%, respectively, without intergroup differences (P = 0.649). OS and cumulative incidences of cardiac death were not significantly different between the propensity score-matched groups (P = 0.475 and 0.649, respectively) (Fig. 2).
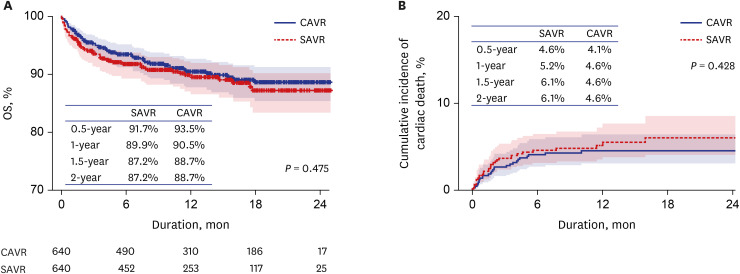
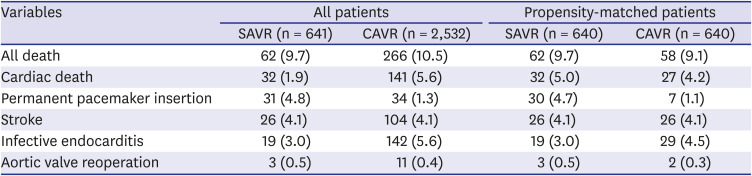
Fig. 2
Comparison of OS and cumulative incidence of cardiac death between the SAVR and CAVR groups after propensity score matching.
OS = overall survival, SAVR = sutureless aortic valve replacement, CAVR = conventional aortic valve replacement.
![]()
Table 3
Major events after CAVR and SAVR during the follow-up
Values are presented as number (%).
CAVR = conventional aortic valve replacement, SAVR = sutureless aortic valve replacement.
![]()
PPM implantation rates
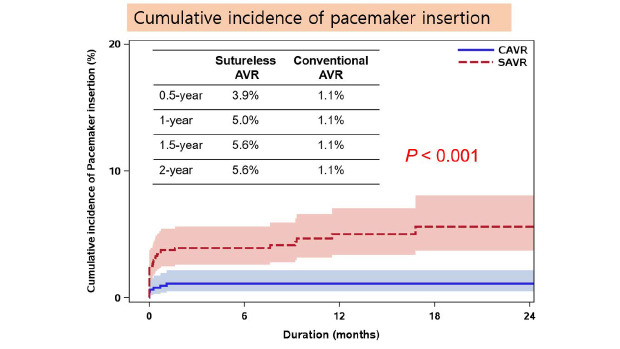
PPM implantation was required in 65 patients during the index hospitalization or follow-up period. The cumulative incidences of PPM implantation at one year and two years were 5.2% and 5.8%, respectively, in the SAVR group and 1.3% and 1.9%, respectively, in the CAVR group. There were significant differences in PPM implantation rate between two groups (P < 0.001) (Fig. 3A). There were only few cases of PPM implantation beyond 6 months after index surgery in the CAVR group. However, the cumulative incidence gradually increased after surgery in the SAVR group.
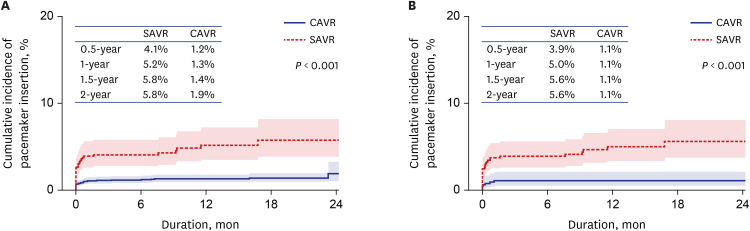
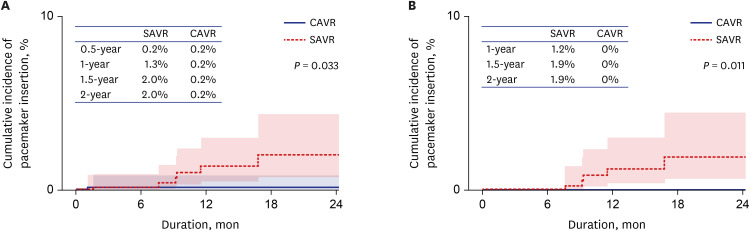
In matched patients, the cumulative incidence of PPM implantation at 6 months in the CAVR was 1.1%, and no patient required PPM implantation beyond 6 months after surgery. However, in the SAVR group, the cumulative incidences of PPM implantation at 0.5, one, and two years were 3.9%, 5.0% and 5.6%, respectively, and the PPM implantations rate increased by 1.5 years. The significant difference in PPM implantation between two groups was sustained after matching (P < 0.001) (Fig. 3B). In landmark analyses from 1 and 6 months after surgery, there were still significant differences in cumulative incidences of PPM implantation between the two groups (P = 0.033 and P = 0.011, respectively; Fig. 4A and B).
Other adverse events during the follow-up
Stroke occurred in 130 patients during the index hospitalization or follow-up period. The cumulative incidences of stroke at one year and two years were 4.2% and 5.2%, respectively. There were no significant differences in the rates of stroke between the two groups before and after propensity score matching (P = 0.649 and P = 0.428, respectively; Fig. 5A and B).
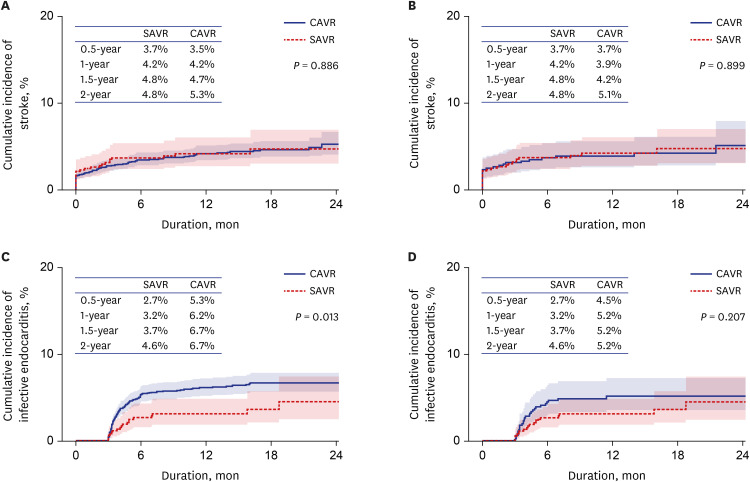
PVE occurred in 161 patients during index hospitalization or follow-up. The cumulative incidence of PVE at one year and two years were 5.6% and 6.3%, respectively. This was significantly lower in the SAVR group than in the CAVR group before matching (P = 0.013). However, there were no significant differences in the cumulative incidence of PVE in the matched patient groups (P = 0.207) (Fig. 5C and D).
Fourteen patients underwent AV reoperation during the index hospitalization or follow-up. All reoperations were performed within 6 months after the index surgery. There were no significant differences in AV reoperation between the 2 groups before and after propensity score matching (P = 0.902 and P = 0.314, respectively).
Comparisons between EDWARDS INTUITY and Perceval S groups
When comparing the outcomes between the EDWARDS INTUITY and Perceval S valves, there were no significant differences in early and follow-up results between the two valve types (Table 4).
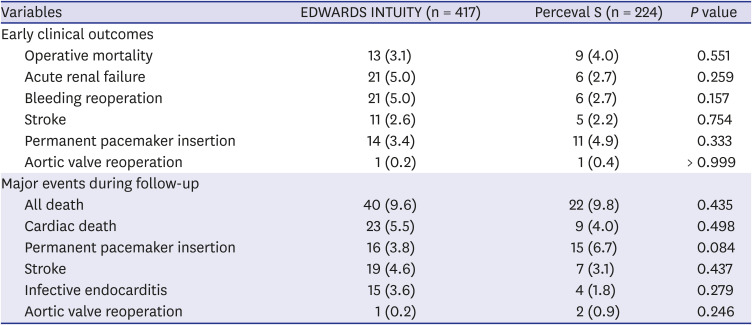
Table 4
Comparisons of EDWARDS INTUITY and Perceval S valves
![]()
DISCUSSION
This study demonstrated that early and 2-year clinical outcomes after AVR using sutureless valves were not different from those after AVR using conventional bioprosthetic AVR, except for higher rates of PPM implantation early after surgery and during the follow-up, in the SAVR group.
After the introduction of sutureless aortic valve systems, many studies have demonstrated the safety and efficacy of SAVR. However, previous studies in large populations were conducted as a single-arm design demonstrating early clinical outcomes after SAVR.15161718192021 Though Ensminger et al.10 reported a study comparing the early outcomes between SAVR and CAVR in 2,042 propensity score-matched patients, the study reported only early clinical outcomes. The present study included 3,173 patients and compared the early and 2-year clinical outcomes of SAVR and CAVR in 1,280 propensity score-matched patients.
One of theoretical advantages of SAVR is that it can reduce the duration of ACC, and this can result in improved clinical outcomes because the duration of ACC is a significant factor associated with clinical outcomes after cardiac surgery. Previous studies quantified that the duration of ACC was an independent predictor of mortality or morbidity after AVR with a 1.4% to 2% increase in the risk per minute of ACC duration.78 Although previous studies consistently demonstrated that SAVR could reduce the duration of ACC and CPB,42223 these were not translated into improved clinical outcomes, and there were no differences in the surgical outcomes such as operative mortality424 and survival rates up to 3 years after surgery25 between SAVR and CAVR. The findings of the present study were in agreement with those of previous studies; there were no differences in the operative mortality, OS up to 2 years after AVR, and cumulative incidence of cardiac death in both overall and matched patient groups.
A possible explanation might be that the association between duration of ACC and clinical outcomes is not linear. A recent retrospective study including 16,272 patients from Japan Cardiovascular Surgery Database reported that the operative mortality was higher only in the group in which the duration of ACC was ≥ 150 minutes than the other groups with duration of ACC of < 60 minutes, 60 to 90 minutes, 90 to 120 minutes, and 120 to 150 minutes.9 In this situation, a reduction of few minutes of ACC time might not improve clinical outcomes after AVR.
The present study also demonstrated a higher rate of PPM insertion after SAVR compared with that after CAVR as in previous studies,41024 and this high rate of PPM insertion has been suggested as one of the concerns after SAVR. The different subannular design of sutureless valves can affect the higher incidence of PPM insertion compared to conventional valves.2627 The subannular skirt might create radial pressure on the atrioventricular node or bundle. The EDWARDS INTUITY's balloon-expandable frame can make a greater radial force to the left ventricular outflow tract and the Perceval S valve also have a subannular skirt that can press the left ventricular outflow tract, especially if the valve was oversized. Notably, the need for PPM is higher not only in the early postoperative period but during the follow-up period up to 2 years after SAVR, whereas no patient required PPM insertion beyond 6 months after surgery in the CAVR group in our study. In the landmark analysis after 1 and 6 months, there were still significant differences in cumulative incidence of PPM between the two groups. Possible explanations for these findings included followings; 1) late rhythm disturbance could be occurred by chronic inflammatory reaction caused by subannular structure of sutureless valves in the SAVR group, and 2) watchful waiting strategy for patients with tolerable heart rates despite postoperative 2nd or 3rd degree atrioventricular block might result in delayed insertion of PPM in the SAVR group patients. Regardless of the underlying mechanisms, the higher rate of PPM insertion in the early and late period after surgery could be another reason that SAVR did not result in improved clinical outcomes despite reduced duration of ACC, because PPM insertion after AVR could reduce long-term survival.2829
The present study failed to demonstrate any advantages of sutureless AVR compared to conventional AVR in terms of early and 2-yaer clinical outcomes. However, when considering the characteristics of sutureless valves, the sutureless AVR has the potential to reduce the risk of surgery in high-risk patients with left ventricular dysfunction, history of previous aortic valve surgery, severe aortic root calcification and narrow sinnotubular junction. In addition, previous studies showed that this technique could facilitate minimally invasive surgery.1730 Further studies with longer-term follow-up might be needed to elucidate the strengths and weaknesses of sutureless AVR.
The present study has several limitations. First, this was a retrospective observational study using the claims data. Therefore, the data regarding preoperative rhythm, echocardiographic data such as preoperative pathophysiology and pressure gradient, and detailed surgical data such as prosthetic valve sizes and duration of ACC and CPB and the proportion of minimal invasive surgery could not be assessed. Although a large patient population was included and propensity score matching was performed to overcome the retrospective nature of the study, unadjusted confounders could affect study results. Second, there might be some underestimation or overestimation of co-morbidities and clinical outcomes because most of preoperative variables and clinical outcomes were drawn on the basis of diagnosis codes or procedure codes. In particular, the stroke rate might be overestimated because it was evaluated based on the diagnosis codes without matching with another codes such as imaging tests. Third, the early morbidities during index hospitalization were treated as the events occurred at the same day because it was impossible to find the occurrence date of morbidities using the claims data. Fourth, data regarding paravalvular leak, which might be an important outcome variable after AVR, could not be drawn from the claims data. Fifth, the follow-up duration was relatively short to show the 2-year survival rates. However, even though 2-year survival rates were estimated from small numbers at risk, the estimated 2-year survival rates had 95% confidence intervals whose width is about 6%–7% in the matched patients, which is not too wide.
 XML Download
XML Download