

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since total body irradiation (TBI) was introduced in bone marrow transplantation, it has been established as an important part of the conditioning regimen for diverse diseases such as leukemia and lymphomas.12 It has been demonstrated that TBI may effectively eradicate chemotherapy-resistant malignant cells in the diseased marrow and reduce tumor burden even at sanctuary sites such as the central nervous system and testis where chemotherapy is relatively ineffective.3 In addition, TBI offers the elimination of lymphocytes to prevent rejection of donor hematopoietic stem cells and provides the physical space for engraftment. Although TBI has been associated with many acute and late adverse effects such as nausea, vomiting, pneumonitis, cataract, neurologic toxicities, and secondary malignancies, a fair number of these effects may be prevented with technical improvements such as restriction of maximally tolerated dose, the use of fractionation, organ shielding, and appropriate supportive cares.45678
The use of haploidentical hematopoietic stem cell transplantation (HSCT) has been growing over the past decades due to the increasing number of patients who lack a human leukocyte antigen (HLA)-matched sibling in developed countries and poor representation in donor registries in many developing countries.9 Despite the challenges of high incidences of graft rejection and graft-versus-host disease (GVHD), the use of haploidentical HSCT is increasing because of its nearly universal and rapid availability of donors and technical improvements in practice to reduce the risk of GVHD, such as the introduction of post-transplantation cyclophosphamide (PTCy).1011 However, the clinical role of TBI in haploidentical HSCT has not been fully identified in many hematologic malignancies.
In this article, we review previous studies and discuss the current use and future perspective of TBI in haploidentical HSCT.
CURRENT USE OF TBI IN HAPLOIDENTICAL HSCT
TBI in haploidentical stem cell transplantation in patients with acute myeloid leukemia (AML) and myelodysplastic syndrome (MDS)
Although AML is one of the most common hematologic malignancies for which TBI-containing regimens have been performed, the clinical benefit of TBI in allogeneic HSCT remains controversial.1213 In haploidentical HSCT in patients with AML and MDS, TBI-based conditioning has been expected to be beneficial in terms of disease control and relapse, but concerns for increased GVHD also have been suggested.14
Solomon et al.15 performed a phase II trial to evaluate TBI-based myeloablative conditioning in haploidentical HSCT in 2015, in which 16 patients with AML and 1 patient with MDS were included. The conditioning regimen consisted of TBI 150 cGy twice a day on days −4 to −1 with fludarabine 30 mg/m2/day for 3 days. PTCy 50 mg/kg/day on days 3 to 4 was used for post-graft immunosuppression. Although clinical outcomes were not presented separately for each disease, all patients achieved complete chimerism by day 30, and the estimated 2-year overall survival (OS) and disease-free survival (DFS) were 78% and 73%, respectively. Grade II to IV acute GVHD was significantly less frequent when compared with patients receiving myeloablative HLA-matched unrelated donor transplantation contemporaneously (43% vs. 63%, P = 0.049).
Expanded results from the same group were published in 2019, and included 42 patients with AML and 3 patients with MDS.16 The conditioning regimen was the same as in the previous study. In this retrospective study, the estimated 4-year OS and DFS were 67% and 60%, respectively. Grade II to IV acute GVHD and moderate to severe chronic GVHD occurred in 17% and 23% of patients, respectively, diagnosed with AML, MDS, acute lymphoblastic leukemia (ALL), chronic myelogenous leukemia, non-Hodgkin lymphoma, or other diseases. None of the patients had engraftment failure.
Another phase II study in which 80 patients with AML received haploidentical HSCT with a conditioning regimen consisting of 200 cGy twice a day on days −9 to −8 with fludarabine (30 mg/m2/day on days −7 to −3) and busulfan (3.2 mg/kg/day on days −6 to −5), and rabbit antithymocyte globulin (1.25 mg/kg/day on days −4 to −1) was conducted.17 In this study, all patients achieved full donor chimerism without delayed engraftment failure. The cumulative incidence of grade III to IV acute GVHD and moderate to severe chronic GVHD was 11.2% and 26.3%, and the 2-year OS and cumulative incidence of relapse were 66.0% and 26.6%, respectively. It is worth noting that cytomegalovirus (CMV) reactivation requiring pre-emptive therapy and/or CMV disease occurred in 72% of patients despite the use of intravenous ganciclovir prophylaxis during the conditioning period, considering previously reported highly positive rate of seropositivity for CMV immunoglobulin G in Korean patients and donors.18
Recently, European group published retrospective analysis in which TBI-based conditioning was compared to chemotherapy-based regimen in 1008 AML patients who underwent haploidentical HSCT with PTCy.14 The median dose of TBI was 1,200 cGy in 89 patients, while others received chemotherapy-based myeloablative conditioning, mostly thiotepa, busulfan, and fludarabine (n = 518). Although PTCy was applied for all patients, TBI-based conditioning showed a significantly higher rate of chronic GVHD (hazard ratio [HR], 1.95; P < 0.01) compared to chemotherapy-based regimen, which did not impact non-relapse mortality (NRM) and GVHD-free, relapse-free survival. Conversely, TBI-based conditioning group presented fewer veno-occlusive disease-related mortality and lower incidence of graft failure. In another registry data from the European MDS group, patients who received TBI-based conditioning haploidentical HSCT revealed no significant effects on prognosis (HR, 1.20; P = 0.44 for OS and HR, 1.12; P = 0.61 for progression-free survival [PFS]).19 Overall, TBI-based conditioning presented relatively comparable survival rates in AML/MDS patients who received haploidentical HSCT with insufficient evidentiary data. The results of GVHD were variable but in most studies it revealed acceptable outcomes. In addition to the role of TBI in these populations, the appropriate strategy to prevent GVHD should be assessed together to improve the survival outcome and quality of life in haploidentical HSCT for patients with AML and MDS.20
TBI in haploidentical stem cell transplantation in patients with ALL
ALL has traditionally been considered the representative hematologic malignancy for which TBI-based conditioning has an established role in allogeneic HSCT.21 In 2018, Kebriaei et al.22 reported that TBI-based conditioning showed superior outcomes compared with busulfan-based regimens in terms of relapse. A number of previous studies have demonstrated that TBI-based regimens are associated with survival benefits in adult patients with ALL, although there were no randomized trials.2324
Solomon et al.16 conducted a retrospective study with 27 adult patients with ALL who received haploidentical HSCT with TBI-based myeloablative conditioning. In that study, the 4-year OS, DFS, and cumulative incidence of relapse were 62%, 51%, and 35%, respectively, which showed no significant difference between patients with AML/MDS and ALL.
In 2014, Fu et al.25 compared TBI (700 cGy)/cyclophosphamide/simustine plus ATG with busulfan/cytarabine/simustine with ATG in haploidentical HSCT. Among the 38 patients in the TBI group, 22 had B-cell ALL and 10 had T-cell ALL. Although TBI-based regimen did not demonstrate superiority in 2-year OS and DFS (60.2% vs. 57.0%, P = 0.937 for OS; 57.9% vs. 56.6%, P = 0.845 for DFS), it was associated with significantly less toxicity of the liver and hemorrhagic cystitis than busulfan-based conditioning.
Srour et al.26 performed a multicenter observational study in which 109 adult patients with ALL received haploidentical HSCT with PTCy. Of all the patients, 57 were treated with TBI-based conditioning. One-year DFS was 51%, and chronic GVHD occurred in 32% of all patients. Although the clinical outcomes of TBI-based regimens were not analyzed separately, there were no statistically significant differences according to preparative regimens for DFS.
The role of TBI-based conditioning in haploidentical HSCT has primarily been explored in patients with acute leukemia, and the wider clinical impact of TBI remains to be established. The H. Lee Moffitt Cancer Center is currently recruiting for a single-arm, phase II trial of haploidentical HSCT using reduced intensity conditioning (RIC) with fludarabine, melphalan, and TBI, in which patients with all hematologic malignancies, including acute leukemias, MDS, and lymphomas, will be included (ClinicalTrials.gov: NCT04191187). Further studies are needed to evaluate the role of TBI in haploidentical HSCT.
TBI in haploidentical stem cell transplantation in patients with lymphoma
Autologous HSCT is usually preferred over allogeneic HSCT as a salvage option for both Hodgkin and non-Hodgkin lymphomas.2728 Allogeneic HSCT has been performed less frequently than salvage chemotherapy or autologous HSCT because it is generally associated with high treatment-related mortality (TRM) despite the relatively strong possibility of being completely cured.2829303132
In a previous retrospective study, Burroughs et al.33 included 28 patients who were diagnosed with Hodgkin lymphoma and received a non-myeloablative (NMA) regimen and haploidentical bone marrow graft. The conditioning regimen consisted of TBI 2 Gy on day -1, cyclophosphamide, and fludarabine. PTCy was administered for the selective depletion of alloreactive T cells. Although these patients were heavily treated (median 5 previous lines, previous autologous HSCT failure in 89%), they showed generous survival outcomes (2-year OS, 58% and PFS, 51%). Interestingly, they revealed a significantly lower risk of relapse (40%) compared with recipients who were grafted from HLA-matched related (56%, P = 0.01) and unrelated (63%, P = 0.03) donors.
In another retrospective study performed at Johns Hopkins University to identify the role of allogeneic transplantation for peripheral T-cell lymphoma, 18 patients received haploidentical transplantation with TBI-based RIC conditioning.34 The conditioning regimen consisted of fludarabine and cyclophosphamide with 200 cGy of TBI, and PTCy was used to prevent GVHD. The estimated 1-year cumulative incidence of NRM was 11%, and relapse occurred in 34% of patients during the same period. Two-year OS and PFS for RIC-based transplantation, of which 6 HLA-identical recipients were included, were 44% and 37%, respectively, suggesting the possibility of long-term survival in the subset of patients with peripheral T-cell lymphoma.
In 2015, the Johns Hopkins group presented the results of a phase II study evaluating post-transplantation rituximab and non-HLA-based donor selection in patients with B-cell lymphoma.35 PTCy was used, and rituximab 375 mg/m2 IV was administered weekly for 8 weeks from 30 days after infusion. Among 69 haploidentical transplantation recipients whose conditioning consisted of fludarabine, cyclophosphamide, and 200 cGy TBI, the 2-year PFS, OS, and cumulative rate of relapse were 63%, 73%, and 23%, respectively, suggesting that post-transplantation rituximab may improve the clinical outcome along with the use of TBI-based NMA conditioning in this population. One year after HSCT, the incidence of grade III to IV acute and chronic GVHD was 6% and 13%, respectively.
TBI in haploidentical stem cell transplantation in patients with multiple myeloma (MM)
Allogeneic HSCT has traditionally been considered a last option for patients with MM who are aged younger than 65 due to relatively excessive NRM.36 Most previous studies were performed in patients who had relapsed or progressed after autologous HSCT, and suggested clinical efficacy with matched related or unrelated donors.373839 However, data on the use of haploidentical donors in MM are still limited, with a lack of randomized studies. In 2019, the European Society for Blood and Marrow Transplantation and CIBMTR reported a retrospective analysis of the outcomes of haploidentical HSCT in 96 MM patients.40 With a median follow-up of 24.0 months, 2-year OS and PFS were 48% and 17%, respectively. Among 75 patients who received RIC/NMA before HSCT, 50 (66.7%) were treated with a TBI (2 Gy)-based regimen, compared with 4 of 17 (23.5%) with MAC. However, there was no significant difference according to the intensity of conditioning. In that study, the use of PTCy and bone marrow source were associated with improved OS.
Castagna et al.41 analyzed 30 MM patients who received haploidentical HSCT with PTCy in 6 different European institutions. In this study, 14 patients who received an NMA (fludarabine/cyclophosphamide/TBI 2 Gy for 13, treosulfan/fludarabine/TBI 2Gy for 1) regimen were included. Although TBI itself was not included in the analysis of risk factors, patients with NMA showed non-inferior outcomes for OS (34% vs. 31%, P = 0.63), PFS (57% vs. 69%, P = 0.28), NRM (7% vs. 12%, P = 0.32), and relapse or progression (38% vs. 46%, P = 0.70) during 18 months compared with patients with MAC, of whom only 2 patients received TBI-based conditioning. Although this study did not focus on the role of TBI in MM, the overall results were encouraging considering heavily pretreated patients with median previous lines of therapy of 3 (range, 1–7).
In 2019, the Chinese group retrospectively compared the clinical outcomes of haploidentical HSCT with those of transplantation with matched-related donors (MRD) in 97 patients with MM.42 All patients received MAC, and TBI was conducted significantly more in haploidentical recipients than in MRD transplant recipients (P = 0.006). Although there was no statistically significant difference in terms of OS, PFS, NRM, and relapse according to whether TBI had been conducted, the results suggested that haploidentical HSCT might overcome its fundamental disadvantage by means of the practical application of TBI.
TBI in haploidentical stem cell transplantation in patients with other hematologic malignancies
The role of allogeneic HSCT in aplastic anemia (AA) has been well established; however, most previous studies have been on bone marrow transplantation with HLA-identical sibling or unrelated donors.43 Few studies have used haploidentical donors and TBI-containing regimens. Clay et al.44 performed haploidentical HSCT using RIC containing TBI 2 Gy and PTCy in 8 patients with refractory AA. Neutrophil engraftment was successful in 6 out of 8, and 1 patient suffered from grade II skin GVHD. In 2015, the Brazilian group reported a retrospective analysis of 16 patients for whom haploidentical HSCT with RIC including TBI (200–600 cGy) and PTCy were applied.45 Platelet engraftment occurred in 75%, and grade II–IV GVHD was observed in 3 patients. The 1-year OS rate was 67.1%. Despite the small number of enrolled patients, these 2 retrospective studies provided encouraging evidence of the possibility of using a haploidentical donor with a TBI-based regimen along with the application of PTCy as GVHD prophylaxis. In 2018, Lee et al.46 performed a prospective study in which doses of ATG and TBI were decreased according to the development of TRM to assess the optimal conditioning regimen for haploidentical HSCT in patients with severe AA. Graft rejection and GVHD prophylaxis consisted of tacrolimus and short-course methotrexate without PTCy. Of the 34 patients enrolled, 24 received 600 cGy of TBI, whereas others received 800 cGy along with fludarabine and ATG. All patients achieved neutrophil engraftment, and the 2-year OS in all patients was 84.6%, with a favorable tendency toward low dose of TBI (91.7% vs. 70.0%, P = 0.155). In addition, a 600 cGy dose of TBI was found to be beneficial for 2-year GVHD-free survival (78.4% vs. 50%, P = 0.115). This study revealed that TBI may play an important role in successful engraftment and in minimizing TRM with an appropriate dose of ATG in patients with severe AA with haploidentical donors.
Allogeneic HSCT is recommended for patients with primary myelofibrosis, depending on the risk score.47 HSCT with haploidentical donors has been suggested as an alternative source of stem cells with the use of PTCy, but there have been no randomized studies to date.48 Although in some studies, haploidentical recipients who received TBI-based conditioning were included, there has been no data to analyze the independent role of TBI in haploidentical HSCT.495051 The MD Anderson Cancer Center is currently conducting an early phase I trial to evaluate the safety and tolerability of haploidentical HSCT with TBI-based regimen and PTCy (ClinicalTrials.gov: NCT03426969). Future studies are needed to elucidate the role of TBI in haploidentical HSCT in patients with primary myelofibrosis.
FUTURE PERSPECTIVES ON TBI IN HAPLOIDENTICAL HSCT
Over the past decades, the clinical outcomes of allogeneic HSCT have improved due to progress in such areas as transplantation methods, infection management, and supportive care.52 As an important part of the conditioning regimen, TBI has shown unique advantages such as uniform distribution over the whole body and decreased exposure to cytotoxic chemotherapeutic agents.2 Based on these favorable aspects, TBI has been suggested for patients who needed intensive conditioning due to high risk of relapse or considerable residual disease burden but were expected to show relatively low efficacy with chemotherapy-only conditioning due to previously heavy exposure to cytotoxic agents.2 Furthermore, various technical improvements have been tried to minimize toxicities related to TBI.3 For example, Jiang et al.53 applied a more targeted form of TBI (10 Gy TBI with augmented dose [12 Gy] to total marrow, central nervous system leukemia, and extramedullary disease sites) in patients with high-risk ALL receiving haploidentical HSCT. They showed sustained full donor stem cell engraftment and excellent eradication of malignant cells with a 1-year DFS of 70.7%. In addition, appropriate shielding and fractionation are needed to decrease the development of diverse toxicities and improve clinical outcomes.2354 However, the heterogeneity of maximum accepted dose to organs and the different fractioned dose in each institution can be obstacles in the investigation of the effectiveness of TBI in HSCT, especially in haploidentical HSCT, considering its relatively higher incidence of overall mortality and TRM.5556 Therefore, it should be critical to assess the most beneficial dose of TBI in haploidentical HSCT. In CIBMTR data which prepared clinical outcomes in HSCT with matched siblings/unrelated or partially matched donors according to the dose of TBI, higher dose of TBI revealed significantly improved relapse rate that was hampered by poorer incidence of NRM concluding that increased dose of TBI presented no survival benefit.57 In that study, TBI was significantly related to chronic GVHD in the first 8 months, but not afterward. Future studies are warranted to assess the most adequate dose of TBI in haploidentical HSCT.
Advancements have been made in haploidentical HSCT along with the improvement of immunosuppressive approaches such as ATG and PTCy.58 In Tables 1 and 2, we summarized the previous studies in which TBI-based conditioning was performed in haploidentical HSCT. In most studies, PTCy 50 mg/kg was administered on days 3 and 4. However, Bacigalupo et al.59 used PTCy on days 3 and 5 in haploidentical BMT, and the incidence of grade III to IV GVHD was 10%. Additionally, one prospective study demonstrated that haploidentical peripheral blood stem cell transplantation with 2 doses of PTCy 25 mg/kg may be feasible for high-risk leukemia and MDS.60 Recently, data from EBMT prepared different immunosuppressive strategies in haploidentical HSCT in patients with acute leukemia.20 In this analysis, an early start of cyclosporine and mycophenolate mofetil with administrations of PTCy on days +3 and +5 showed significantly improved leukemic-free survival and GVHD-free, relapse-free survival compared to other schedules of immunosuppressant. It would be mandatory to assess the most optimal immunosuppressive regimen specialized for haploidentical HSCT. A phase I/II study to compare the efficacy of reduced dose of PTCy with the standard dose is ongoing (ClinicalTrials.gov: NCT03983850). The results of that study may shed light on the optimal administration of PTCy in haploidentical HSCT. Besides PTCy, post-transplantation rituximab also showed the possibility of improving clinical outcomes in TBI-based haploidentical HSCT.35 In particular, peri-transplantation rituximab revealed its efficacy in B-cell lymphoma patients who received HSCT from matched related and unrelated donors; its role in TBI-based haploidentical HSCT would be valuable to assess in the future.61 The role of ex vivo T-cell depletion is another important methodological issue in TBI-based haploidentical HSCT. It showed noticeable outcomes in pediatric patients in one previous study, but has yet to be examined in adult patients, to the best of our knowledge.62 In addition, the use of chimeric antigen receptor T-cells to prevent relapse after TBI-based haploidentical HSCT is another issue that warrants future study.63
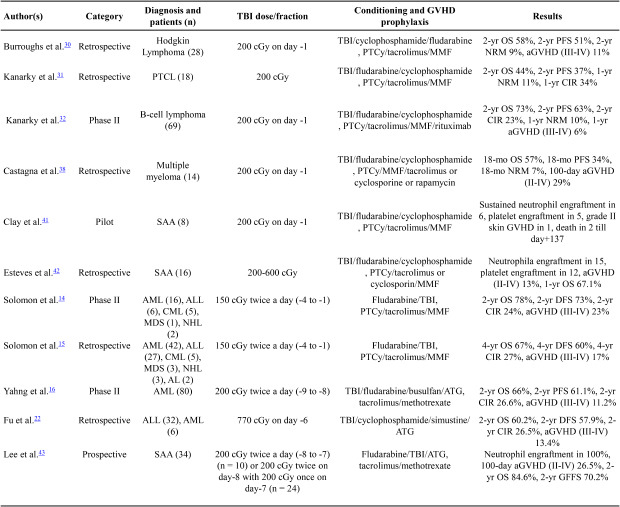
Table 1
Previous studies of haploidentical HSCT using TBI (2–6 gray)-based conditioning regimen
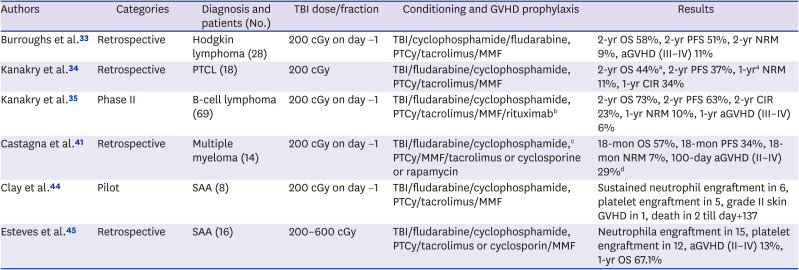
| Authors | Categories | Diagnosis and patients (No.) | TBI dose/fraction | Conditioning and GVHD prophylaxis | Results |
|---|---|---|---|---|---|
| Burroughs et al.33 | Retrospective | Hodgkin lymphoma (28) | 200 cGy on day −1 | TBI/cyclophosphamide/fludarabine, PTCy/tacrolimus/MMF | 2-yr OS 58%, 2-yr PFS 51%, 2-yr NRM 9%, aGVHD (III–IV) 11% |
| Kanakry et al.34 | Retrospective | PTCL (18) | 200 cGy | TBI/fludarabine/cyclophosphamide, PTCy/tacrolimus/MMF | 2-yr OS 44%a, 2-yr PFS 37%, 1-yra NRM 11%, 1-yr CIR 34% |
| Kanakry et al.35 | Phase II | B-cell lymphoma (69) | 200 cGy on day −1 | TBI/fludarabine/cyclophosphamide, PTCy/tacrolimus/MMF/rituximabb | 2-yr OS 73%, 2-yr PFS 63%, 2-yr CIR 23%, 1-yr NRM 10%, 1-yr aGVHD (III–IV) 6% |
| Castagna et al.41 | Retrospective | Multiple myeloma (14) | 200 cGy on day −1 | TBI/fludarabine/cyclophosphamide,c PTCy/MMF/tacrolimus or cyclosporine or rapamycin | 18-mon OS 57%, 18-mon PFS 34%, 18-mon NRM 7%, 100-day aGVHD (II–IV) 29%d |
| Clay et al.44 | Pilot | SAA (8) | 200 cGy on day −1 | TBI/fludarabine/cyclophosphamide, PTCy/tacrolimus/MMF | Sustained neutrophil engraftment in 6, platelet engraftment in 5, grade II skin GVHD in 1, death in 2 till day+137 |
| Esteves et al.45 | Retrospective | SAA (16) | 200–600 cGy | TBI/fludarabine/cyclophosphamide, PTCy/tacrolimus or cyclosporin/MMF | Neutrophila engraftment in 15, platelet engraftment in 12, aGVHD (II–IV) 13%, 1-yr OS 67.1% |
HSCT = hematopoietic stem cell transplantation, TBI = total body irradiation, GVHD = graft-versus-host disease, OS = overall survival, PFS = progression-free survival, CIR = cumulative incidence of relapse, aGVHD = acute graft-versus-host disease, NRM = non-relapse mortality, SAA = severe aplastic anemia.
aIncluded 6 patients with matched donor and reduced intensity conditioning without TBI; bGiven once weekly for 8 weeks from day +30 ± 3 to prevent both relapse and GVHD; c1 patient received TBI/treosulfan/fludarabine; dIncluded 16 patients with different conditioning regimens with or without TBI.
Table 2
Previous studies of haploidentical HSCT using TBI (6–12 gray)-based conditioning regimen
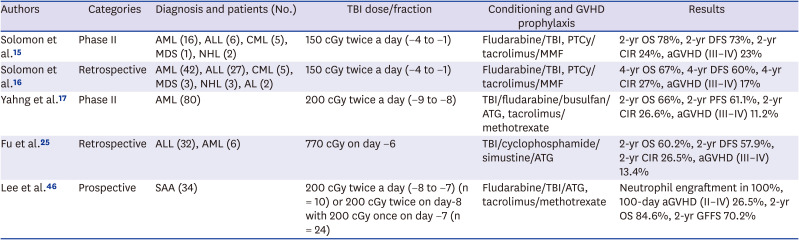
| Authors | Categories | Diagnosis and patients (No.) | TBI dose/fraction | Conditioning and GVHD prophylaxis | Results |
|---|---|---|---|---|---|
| Solomon et al.15 | Phase II | AML (16), ALL (6), CML (5), MDS (1), NHL (2) | 150 cGy twice a day (−4 to −1) | Fludarabine/TBI, PTCy/tacrolimus/MMF | 2-yr OS 78%, 2-yr DFS 73%, 2-yr CIR 24%, aGVHD (III–IV) 23% |
| Solomon et al.16 | Retrospective | AML (42), ALL (27), CML (5), MDS (3), NHL (3), AL (2) | 150 cGy twice a day (−4 to −1) | Fludarabine/TBI, PTCy/tacrolimus/MMF | 4-yr OS 67%, 4-yr DFS 60%, 4-yr CIR 27%, aGVHD (III–IV) 17% |
| Yahng et al.17 | Phase II | AML (80) | 200 cGy twice a day (−9 to −8) | TBI/fludarabine/busulfan/ATG, tacrolimus/methotrexate | 2-yr OS 66%, 2-yr PFS 61.1%, 2-yr CIR 26.6%, aGVHD (III–IV) 11.2% |
| Fu et al.25 | Retrospective | ALL (32), AML (6) | 770 cGy on day −6 | TBI/cyclophosphamide/simustine/ATG | 2-yr OS 60.2%, 2-yr DFS 57.9%, 2-yr CIR 26.5%, aGVHD (III–IV) 13.4% |
| Lee et al.46 | Prospective | SAA (34) | 200 cGy twice a day (−8 to −7) (n = 10) or 200 cGy twice on day-8 with 200 cGy once on day −7 (n = 24) | Fludarabine/TBI/ATG, tacrolimus/methotrexate | Neutrophil engraftment in 100%, 100-day aGVHD (II–IV) 26.5%, 2-yr OS 84.6%, 2-yr GFFS 70.2% |
HSCT = hematopoietic stem cell transplantation, TBI = total body irradiation, GVHD = graft-versus-host disease, AML = acute myeloid leukemia, ALL = acute lymphoblastic leukemia, CML = chronic myelogenous leukemia, MDS = myelodysplastic syndrome, NHL = non-Hodgkin lymphoma, AL = acute leukemia, unspecified, PTCy = post-transplantation cyclophosphamide, MMF = mycophenolate mofetil, OS = overall survival, DFS = disease-free survival, CIR = cumulative incidence of relapse, aGVHD = acute graft-versus-host disease, SAA = severe aplastic anemia, GFFS = GVHD- and failure-free survival.
Traditionally, older adult patients have not been candidates for allogeneic HSCT due to the high risk of TRM.64 However, due to advances in techniques and strategies, selected older adult patients may benefit from allogeneic HSCT, even with haploidentical donors.65 One retrospective study with EBMT and CIBMTR compared the outcomes of PTCy-based haploidentical HSCT with others in patients with diffuse large B-cell lymphoma.66 The number of patients older than 60 years who received HSCT was significantly higher in the haploidentical group. In addition, a significantly higher rate of these patients (86%) received TBI-based conditioning. In this study, the 3-year OS and relapse rates of the haploidentical group were 46% and 41%, respectively, which were not significantly different from the outcomes of matched donors. However, there is no randomized trial in older adult patients supporting the efficacy and safety of TBI-based haploidentical HSCT. The relevance of TBI-based conditioning in older adult patients with haploidentical donors warrants further study, considering the current tendency toward increasing age restriction and lack of matched donors for HSCT.67
CONCLUSION
In this review, we examined previous studies on the use of TBI-based conditioning in haploidentical HSCT. In diverse hematological malignancies, allogeneic HSCT is still the most powerful tool for a cure, and TBI has distinct advantages as a conditioning regimen for HSCT. The use of a haploidentical donor should increase because of its almost unlimited availability. Therefore, continuous efforts to improve the outcome of haploidentical HSCT should be made, and assessment of the appropriate use of TBI in haploidentical HSCT in various conditions will be needed in the future.
 XML Download
XML Download